4453
Reconstructing High-Quality Sodium MR Images from Limited Noisy k-Space Data with Model-Assisted Deep Learning1Beckman Institute for Advanced Science and Technology, University of Illinois, Urbana-Champaign, Urbana, IL, United States, 2Department of Electrical and Computer Engineering, University of Illinois, Urbana-Champaign, Urbana, IL, United States, 3Center for Magnetic Resonance Research, University of Illinois at Chicago, Chicago, IL, United States
Synopsis
Sodium MRI can acquire important biological information about cell integrity and tissue viability, but its clinical application has been limited by low SNR and poor spatial resolution. We propose a novel method to reconstruct high-quality sodium images from limited and noisy k-space data. The new method synergistically integrates model-based reconstruction with deep learning. Simulation and experimental results show that the proposed method can reconstruct high-SNR and high-resolution sodium images, which clearly delineate lesions such as brain tumors.
Introduction
Sodium MRI, complementary to proton MRI, has long been recognized as a powerful tool for noninvasive measurement of tissue sodium concentration (TSC), which is a direct, quantitative bioscale for cell integrity and tissue viability1-6. However, its clinical applications remain limited by low sensitivity due to its low gyromagnetic ratio and biological concentrations. With state-of-the-art data acquisition technology, sodium MRI scans at 3T typically acquire 44×44×44 encodings in 10 minutes with marginal SNR7-9. Larger k-space coverage (e.g., 64×64×64 encodings) can be achieved but at the expense of longer scan time and further reduced SNR10-14. The low spatial resolution resulting from limited k-space coverage and fast transverse relaxation leads to large partial volume effects that are especially problematic when the region of interest is close to CSF spaces.Constrained image reconstruction has shown great potential for overcoming the low SNR and poor resolution problems with sodium MRI. Conventional constrained reconstruction methods exploit the anatomical information from a companion proton scan15,16 or transformed sparsity in sodium images17-20 to enhance the SNR and spatial resolution. However, these methods have several known limitations: (a) minimal improvement in sodium-dependent novel features (e.g., lesion), (b) potential reconstruction error due to inaccurate anatomical boundaries, and (c) ineffectiveness of the sparsity constraint for low-SNR data. Deep learning (DL) methods have recently been proposed for reconstructing sodium images from sparsely sampled data21 or noisy data22. These methods achieved encouraging results, but they also require large amounts of experimental data with ground truth for training and may suffer from the well-known instability problem23,24.
To address these problems, we propose a model-assisted DL method to reconstruct high-quality sodium images from limited noisy k-space data. The new method has been validated using simulation and experimental data, producing very encouraging results.
Methods
The proposed method decomposes the desired sodium image $$$\rho(\boldsymbol{x})$$$ as:$$\rho(\boldsymbol{x})=\sum_{m=-M}^{M}\alpha_{m}\rho_{\mathrm{ref}}(\boldsymbol{x})e^{-i2\pi m\Delta \boldsymbol{k}\cdot \boldsymbol{x}}+\rho_{\mathrm{s}}(\boldsymbol{x}),$$
where $$$\rho_{\mathrm{ref}}(\boldsymbol{x})$$$ represents a reference image for the generalized series (GS) model25-28 used to incorporate anatomical constraints, and $$$\rho_{\mathrm{s}}(\boldsymbol{x})$$$ a sparse component used to capture novel features. This image model was introduced in a recent work29, in which $$$\rho_{\mathrm{ref}}(\boldsymbol{x})$$$ was obtained using a tissue-based compartmental model and $$$\rho_{\mathrm{s}}(\boldsymbol{x})$$$ was obtained using a conventional L1-regularized reconstruction.
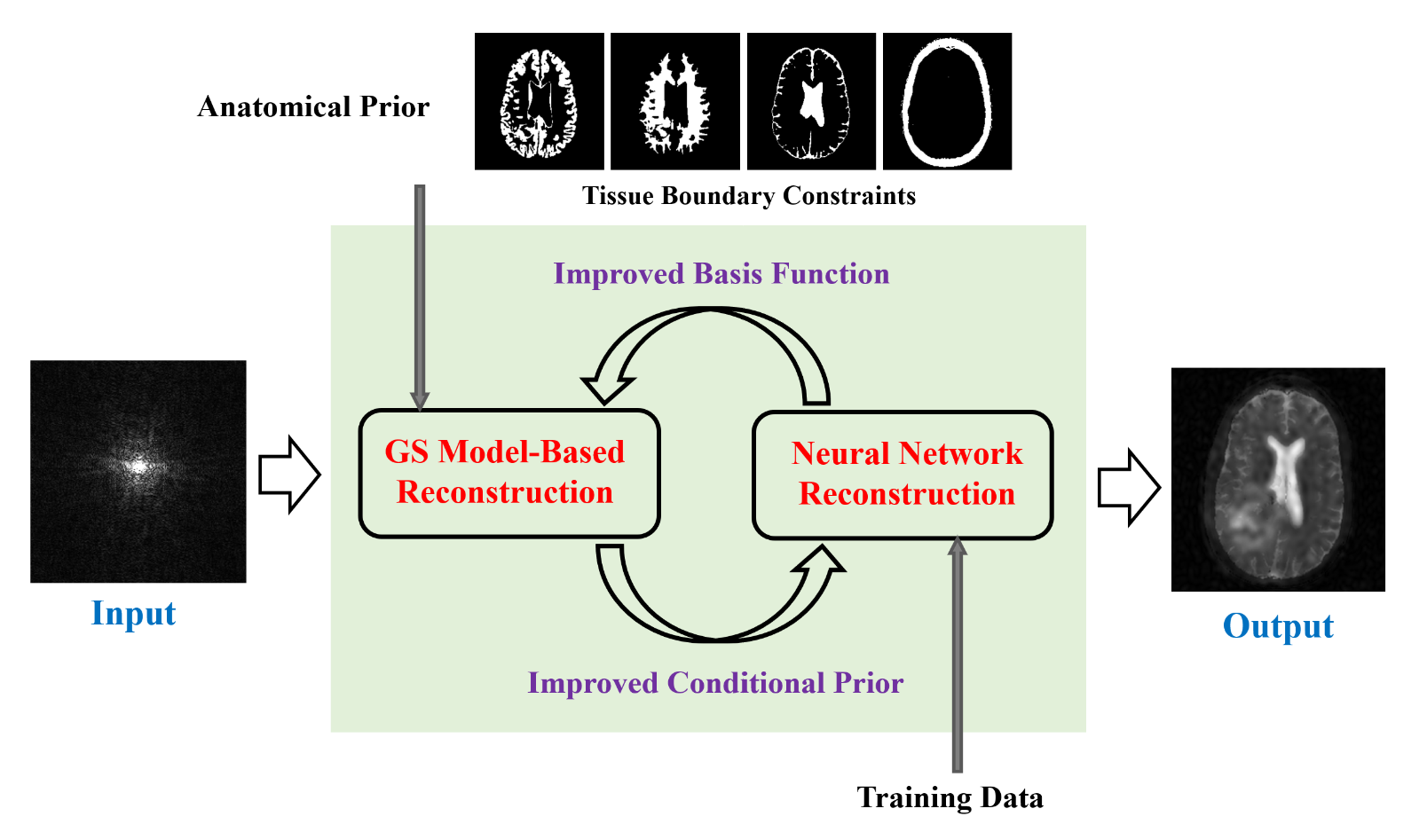
In this work, we further enhance the capability and robustness of this model by integrating the GS model with a DL network, as illustrated in Fig. 1. The proposed method has the following key features: (a) utilizing an unrolled neural network to learn a sparsity-promoting regularization to compensate the GS model, (b) stabilizing the DL module with the output of the GS model as a conditional prior, and (c) updating the basis functions of the GS model progressively using the output of the DL module. Because the DL module is used to compensate the GS model, it can be trained using simulated data. This feature is very desirable since it eliminates the need of large amounts of experimental data with ground truth as in the case of most DL methods.
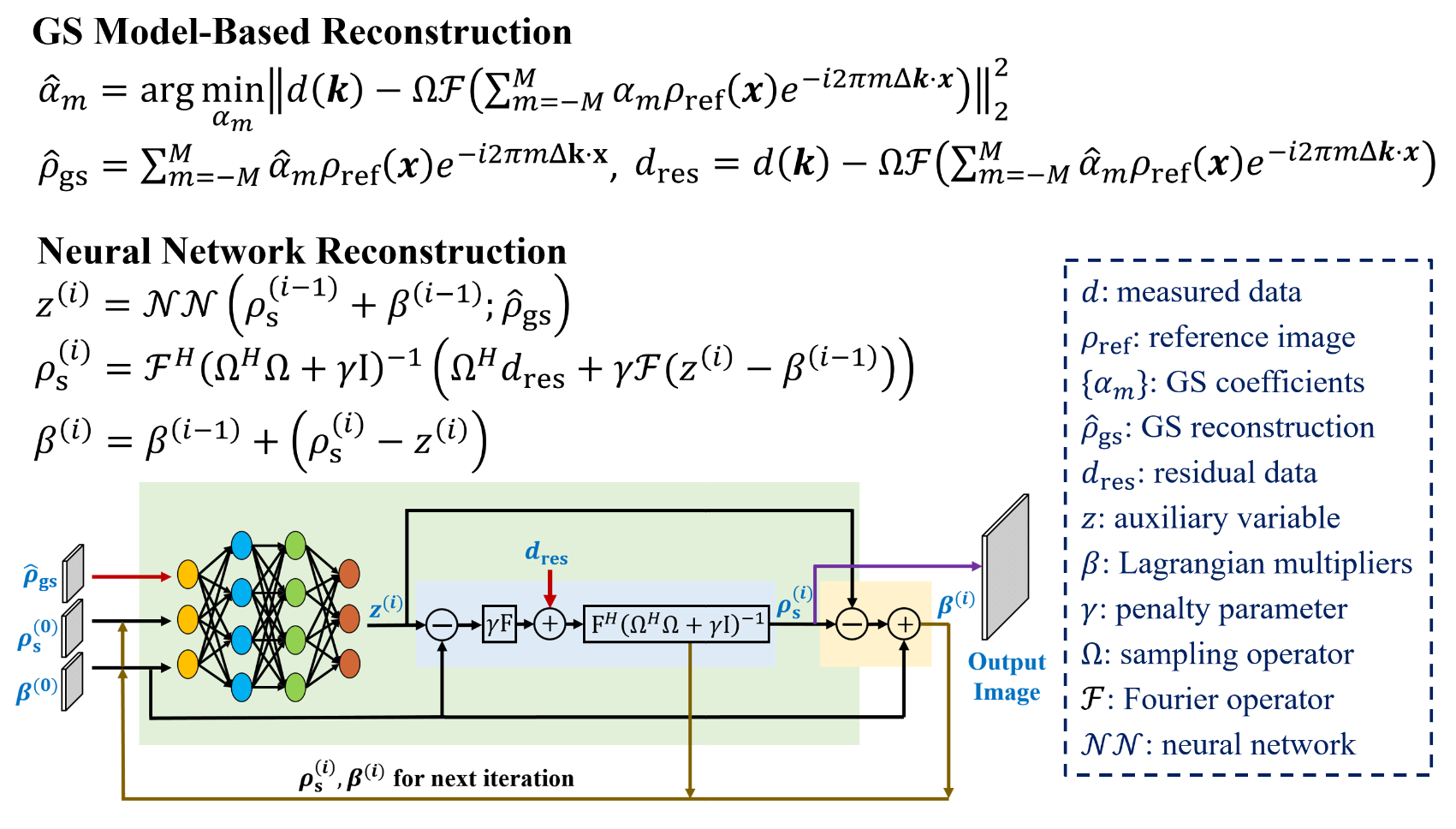
More specifically, in the first iteration, the GS component $$$\hat{\rho}_{\mathrm{gs}}^{(1)}(\boldsymbol{x})$$$ was estimated using a tissue-based compartmental model29. Then a network that unrolled the alternating direction method of multipliers (ADMM) algorithm was used30-32, as described in Fig. 2. Mathematically, it is equivalent to finding an optimal regularization functional $$$R(\cdot)$$$ for $$$\rho_{\mathrm{s}}(\boldsymbol{x})$$$ to compensate the GS model the best:
$$\hat{\rho}_{\mathrm{s}}^{(1)}(\boldsymbol{x})=\arg\min_{\rho_{\mathrm{s}}(\boldsymbol{x})}\left\|d(\boldsymbol{k})-\Omega\mathcal{F}\left(\hat{\rho}_{\mathrm{gs}}^{(1)}(\boldsymbol{x})+\rho_{\mathrm{s}}(\boldsymbol{x})\right)\right\|_2^2+R\left(\rho_{\mathrm{s}}(\boldsymbol{x});\hat{\rho}_{\mathrm{gs}}^{(1)}(\boldsymbol{x})\right).$$
The DL network was trained using synthetic data generated from 160 in vivo datasets with more than 16,000 2D images. After training, the network effectively reconstructed sodium-dependent novel features and compensated any boundary mismatch artifacts that the GS model failed to capture. It is worth noting that both $$$\rho_{\mathrm{s}}(\boldsymbol{x})$$$ and $$$\hat{\rho}_{\mathrm{gs}}^{(1)}(\boldsymbol{x})$$$ were included as the network input so that $$$\hat{\rho}_{\mathrm{gs}}^{(1)}(\boldsymbol{x})$$$ can be effectively used as a conditioner to bring additional prior information to the DL network. The additional information helped stabilize the network for better recovery of $$$\rho_{\mathrm{s}}(\boldsymbol{x})$$$.
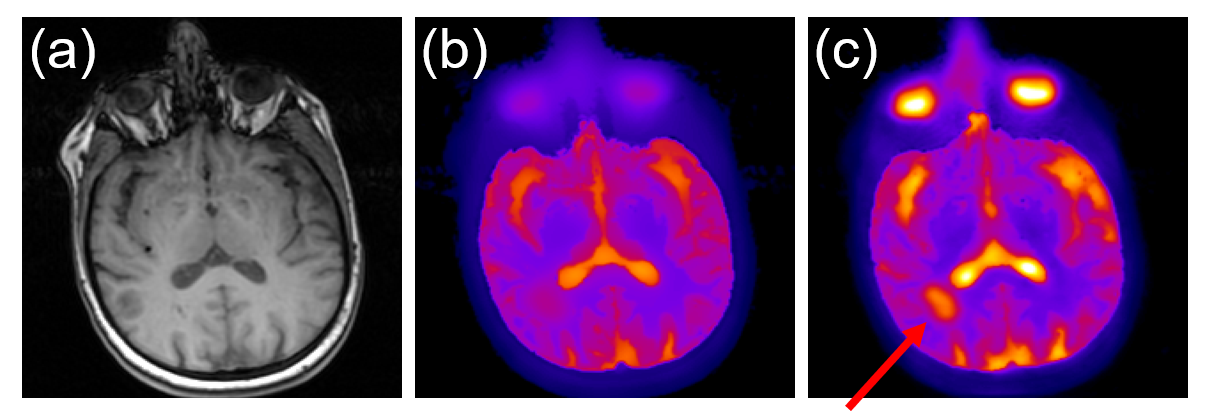
The network, in turn, helped improve the GS model basis functions by updating the reference with $$$\rho_{\mathrm{ref}}^{(2)}(\boldsymbol{x})=\hat{\rho}_{\mathrm{gs}}^{(1)}(\boldsymbol{x})+\hat{\rho}_{\mathrm{s}}^{(1)}(\boldsymbol{x})$$$. With the updated reference (shown in Fig. 3), the GS model provided better reconstruction results. The progressively improved GS reconstructions made $$$\rho_{\mathrm{s}}(\boldsymbol{x})$$$ sparser and easier to recover from limited and noisy data. The alternative update of the GS model and neural network was performed several times until convergence.
Results
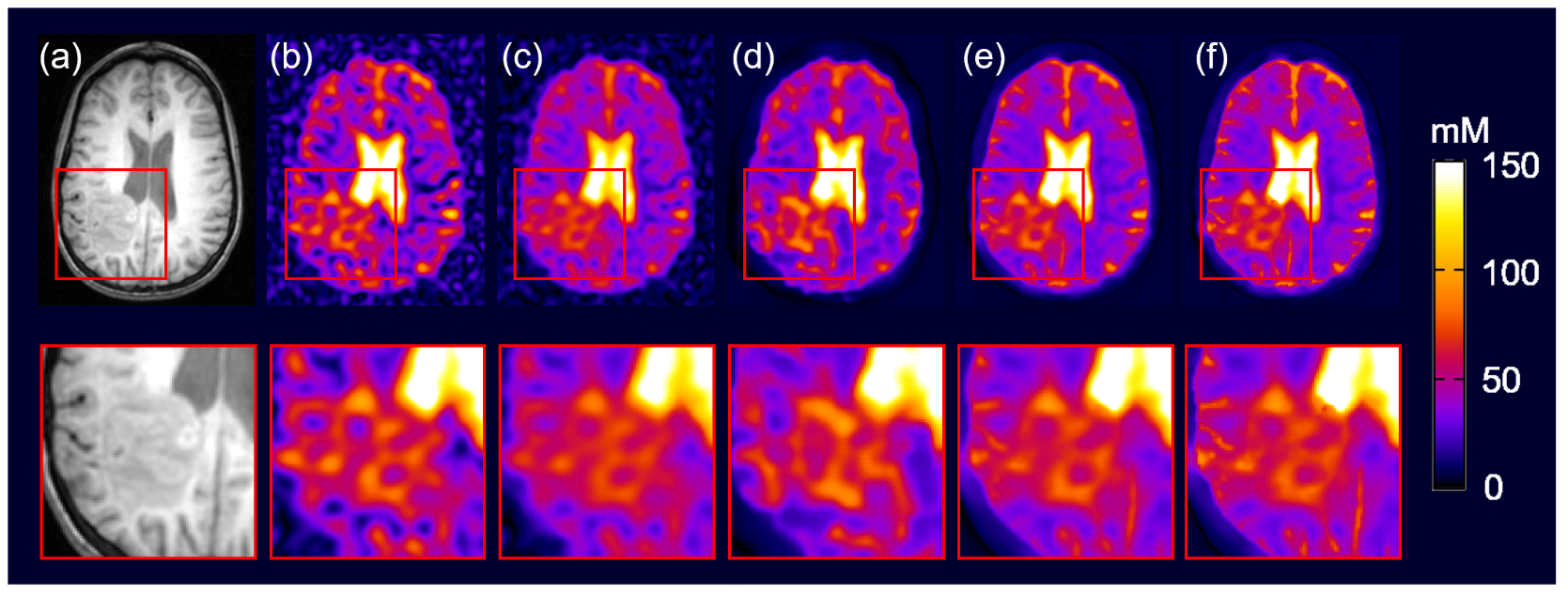
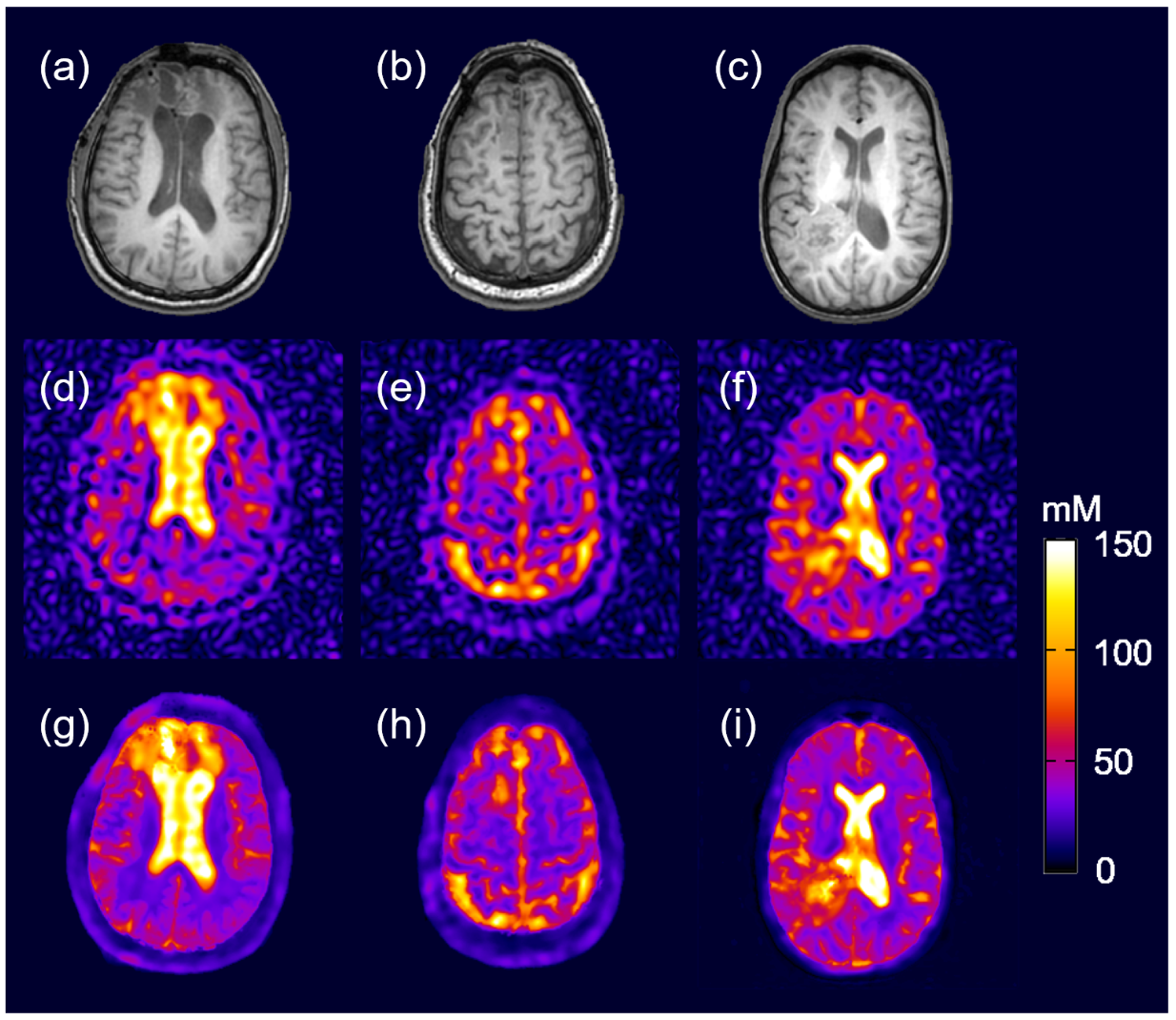
Our method has been validated using simulated and experimental data, producing high-SNR and high-resolution sodium images. Figure 4 shows simulation results using Fourier reconstruction, anatomically constrained reconstruction33, end-to-end neural network21 and our proposed method compared with the ground truth. As can be seen, the proposed method showed significant improvement of SNR and spatial resolution in both anatomical features and the lesion, which matched well with the ground truth. Figure 5 shows TSC maps of brain tumor patients. Again, the proposed method produced high-quality reconstructions with reduced noise-introduced variations and smaller partial volume effects from CSF, leading to much more clear delineation of the lesion.Conclusions
A novel model-assisted DL method has been proposed to enable robust reconstruction of high-quality sodium images from limited noisy k-space data. The proposed method provides an effective solution to the low-SNR and low-resolution problems associated with sodium MRI, which may significantly enhance its clinical use at 3T.Acknowledgements
The work reported in this paper was supported, in part, by the National Institutes of Health (NIH); contract grant number: KRT RO1 CA1295531-01A1.References
1. Lu A, Atkinson IC, Thulborn KR. Sodium magnetic resonance imaging and its bioscale of tissue sodium concentration. In: EMagRes. John Wiley & Sons, Ltd; 2007.
2. Madelin G, Regatte RR. Biomedical applications of sodium MRI in vivo. J Magn Reson Imaging. 2013;38(3):511-529.
3. Madelin G, Lee JS, Regatte RR, Jerschow A. Sodium MRI: Methods and applications. Prog Nucl Magn Reson Spectrosc. 2014;79:14-47.
4. Thulborn KR. Quantitative sodium MR imaging: A review of its evolving role in medicine. Neuroimage. 2018;168:250-268.
5. Poku LO, Phil M, Cheng Y, Wang K, Sun X. 23Na‐MRI as a noninvasive biomarker for cancer diagnosis and prognosis. J Magn Reson Imaging. 2021;53(4):995-1014.
6. Zaric O, Juras V, Szomolanyi P, et al. Frontiers of sodium MRI revisited: From cartilage to brain imaging. J Magn Reson Imaging. 2021;54(1):58-75.
7. Lu A, Atkinson IC, Claiborne TC, Damen FC, Thulborn KR. Quantitative sodium imaging with a flexible twisted projection pulse sequence. Magn Reson Med. 2010;63(6):1583-1593.
8. Atkinson IC, Lu A, Thulborn KR. Clinically constrained optimization of flexTPI acquisition parameters for the tissue sodium concentration bioscale. Magn Reson Med. 2011;66(4):1089-1099.
9. Thulborn KR, Lu A, Atkinson IC, et al. Residual tumor volume, cell volume fraction, and tumor cell kill during fractionated chemoradiation therapy of human glioblastoma using quantitative sodium MR imaging. Clin Cancer Res. 2019;25(4):1226-1232.
10. Nagel AM, Laun FB, Weber M-A, Matthies C, Semmler W, Schad LR. Sodium MRI using a density-adapted 3D radial acquisition technique. Magn Reson Med. 2009;62(6):1565-1573.
11. Qian Y, Stenger VA, Boada FE. Parallel imaging with 3D TPI trajectory: SNR and acceleration benefits. Magn Reson Imaging. 2009;27(5):656-663.
12. Pipe JG, Zwart NR, Aboussouan EA, Robison RK, Devaraj A, Johnson KO. A new design and rationale for 3D orthogonally oversampled k -space trajectories. Magn Reson Med. 2011;66(5):1303-1311.
13. Grover H, Qian Y, Boada FE, Lakshmanan K, Flanagan S, Lui YW. MRI evidence of altered callosal sodium in mild traumatic brain injury. Am J Neuroradiol. 2018;39(12):2200-2204.
14. Neto LPN, Madelin G, Sood TP, et al. Quantitative sodium imaging and gliomas: A feasibility study. Neuroradiology. 2018;60(8):795-802.
15. Gnahm C, Bock M, Bachert P, Semmler W, Behl NGR, Nagel AM. Iterative 3D projection reconstruction of 23Na data with an 1H MRI constraint. Magn Reson Med. 2014;71(5):1720-1732.
16. Gnahm C, Nagel AM. Anatomically weighted second-order total variation reconstruction of 23Na MRI using prior information from 1H MRI. Neuroimage. 2015;105:452-461.
17. Madelin G, Chang G, Otazo R, Jerschow A, Regatte RR. Compressed sensing sodium MRI of cartilage at 7T: Preliminary study. J Magn Reson. 2012;214:360-365.
18. Lachner S, Zaric O, Utzschneider M, et al. Compressed sensing reconstruction of 7 Tesla 23Na multi-channel breast data using 1H MRI constraint. Magn Reson Imaging. 2019;60:145-156.
19. Behl NGR, Gnahm C, BacherT P, Ladd ME, Nagel AM. Three-dimensional dictionary-learning reconstruction of 23Na MRI data. Magn Reson Med. 2016;75(4):1605-1616.
20. Utzschneider M, Behl NGR, Lachner S, et al. Accelerated quantification of tissue sodium concentration in skeletal muscle tissue: Quantitative capability of dictionary learning compressed sensing. Magn Reson Mater Physics, Biol Med. 2020;33(4):495-505.
21. Adlung A, Paschke NK, Golla AK, et al. 23Na MRI in ischemic stroke: Acquisition time reduction using postprocessing with convolutional neural networks. NMR Biomed. 2021;34(4):e4474.
22. Koppers S, Coussoux E, Romanzetti S, Reetz K, Merhof D. Sodium image denoising based on a convolutional denoising autoencoder. In: Bildverarbeitung Für Die Medizin 2019. Springer Vieweg; 2019:98-103.
23. Antun V, Renna F, Poon C, Adcock B, Hansen AC. On instabilities of deep learning in image reconstruction and the potential costs of AI. Proc Natl Acad Sci. 2020;117(48):30088-30095.
24. Knoll F, Hammernik K, Kobler E, Pock T, Recht MP, Sodickson DK. Assessment of the generalization of learned image reconstruction and the potential for transfer learning. Magn Reson Med. 2019;81(1):116-128.
25. Liang Z-P, Lauterbur PC. An efficient method for dynamic magnetic resonance imaging. IEEE Trans Med Imaging. 1994;13(4):677-686.
26. Liang Z-P, Lauterbur PC. A generalized series approach to MR spectroscopic imaging. IEEE Trans Med Imaging. 1991;10(2):132-137.
27. Liang Z-P, Madore B, Glover GH, Pelc NJ. Fast algorithms for GS-model-based image reconstruction in data-sharing Fourier imaging. IEEE Trans Med Imaging. 2003;22(8):1026-1030.
28. Hess CP, Liang Z-P, Lauterbur PC. Maximum cross-entropy generalized series reconstruction. Int J Imaging Syst Technol. 1999;10(3):258-265.
29. Zhao Y, Guo R, Li Y, Thulborn KR, Liang Z-P. High-resolution sodium imaging using anatomical and sparsity constraints for denoising and recovery of novel features. Magn Reson Med. 2021;86(2):625-636.
30. Yang Y, Sun J, Li H, Xu Z. Deep ADMM-Net for compressive sensing MRI. In: Proceedings of the 30th International Conference on Neural Information Processing Systems. Curran Associates Inc.; 2016:10-18.
31. Aggarwal HK, Mani MP, Jacob M. MoDL: Model-based deep learning architecture for inverse problems. IEEE Trans Med Imaging. 2019;38(2):394-405.
32. Schlemper J, Caballero J, Hajnal J V., Price AN, Rueckert D. A deep cascade of convolutional neural networks for dynamic MR image reconstruction. IEEE Trans Med Imaging. 2018;37(2):491-503.
33. Haldar JP, Hernado D, Song SK, Liang Z-P. Anatomically constrained reconstruction from noisy data. Magn Reson Med. 2008;59(4):810-818.
Figures