4358
Ultra-thin slice Time-of-Flight MR angiography for brain with a deep learning constrained Compressed SENSE reconstruction1Philips Japan, Tokyo, Japan, 2Tokyo Metropolitan Police Hospital, Tokyo, Japan, 3Philips Healthcare, Best, Netherlands
Synopsis
Time-of-flight MR angiography (TOF-MRA) is a non-contrast-enhanced imaging technique widely used to visualize intracranial vasculature. In this study, we investigated the use of ultra-thin slice (up to 0.4 mm) to improve the delineation of the cerebral arteries in TOF-MRA. To reduce the noise while preserving the image quality, Compressed SENSE AI (CS-AI) reconstruction was used. Our results showed that the improved noise reduction by CS-AI enabled better visualization of vessels, especially on the thinner slices compared to conventional Compressed-SENSE. The usefulness of CS-AI was also demonstrated in clinical cases with moyamoya disease and suspected aneurysm patients.
Introduction
Time-of-flight MR angiography (TOF-MRA) is a non-contrast-enhanced imaging technique widely used to visualize intracranial vasculature1. The cerebral arteries are highly tortuous and sometimes difficult to visualize clearly by TOF-MRA. Improving the delineation of arteries in the middle cerebral artery (MCA) is of particular interest and acquiring TOF-MRA with very thin slices would improve the visualization of tortuous vessels. However, thinner slices also suffer from more noise in the image, which makes ultra-thin slice imaging challenging.In this study, Compressed SENSE AI (CS-AI) reconstruction2,3 was used to reduce the noise while preserving the image quality under ultra-thin slice TOF-MRA. It is hypothesized that the slice thickness can be significantly reduced while maintaining the image quality by using the CS-AI reconstruction algorithm, thus leading to the better visualization of cerebral vascular patterns. The purpose of this study was to acquire ultra-thin slice 3D TOF-MRA using the CS-AI reconstruction and compare the image quality with conventional Compressed-SENSE (C-SENSE).
Methods
Three healthy volunteers and two patients; one with moyamoya disease and another with suspected aneurysm were examined on 3.0T whole-body clinical systems (Ingenia Elition X, Philips Healthcare) using a 32ch head coil, following informed consent with an IRB-approved protocol.Volunteer study: TOF-MRA was acquired by C-SENSE and CS-AI at slice thicknesses 1.0, 0.8, 0.6, and 0.4 mm, and then reconstructed to 0.5, 0.4, 0.3, and 0.2 mm, respectively. Total scan times were 3:50, 4:46, 6:22, and 9:41 min, respectively. In-plane resolution was 0.55x0.75 mm2 and reconstructed to 0.32x0.32 mm2. 90 slices.
Patient study: TOF-MRA was acquired with C-SENSE and CS-AI at voxel size 0.4x0.8x0.8 mm3 and reconstructed to 0.2x0.2x0.4 mm3. 150 slices, total scan time = 4:09 min. Following parameters were common to all volunteer and patient examinations: FOV=200x200 mm, TR/TE=25/3.5 ms, flip angle=18, acceleration factor=5.4, number of signals averaged (NSA)=1.
Quantitative evaluation: image quality was evaluated by measuring the number of vessels in TOF-MRA. On the volunteer image, a straight line was drawn in the left MCA area on a 90-mm slab maximum intensity projection image (MIP). The signal profile along that line was then obtained for the C-SENSE and CS-AI. Region of interest (ROI) was placed on the background stationary tissues in the brain parenchyma. A signal was defined as coming from a vessel if the signal was greater than STave+5STSD, where STave and STSD are the mean signal intensity and standard deviation in the stationary tissue ROI, respectively.
The CS-AI model used in this study is the extension of the previously introduced AI-based reconstruction algorithm, Adaptive-CS-Net2,3. In CS-AI, the iterative optimization procedure in the C-SENSE reconstruction chain is unrolled for a fixed number of reconstruction blocks. Each block consists mainly of Unet-like architecture, which performs as a denoiser. The model was trained on more than 700,000 images, including 2D and 3D data, and multiple contrasts and anatomical areas.
Results and Discussions:
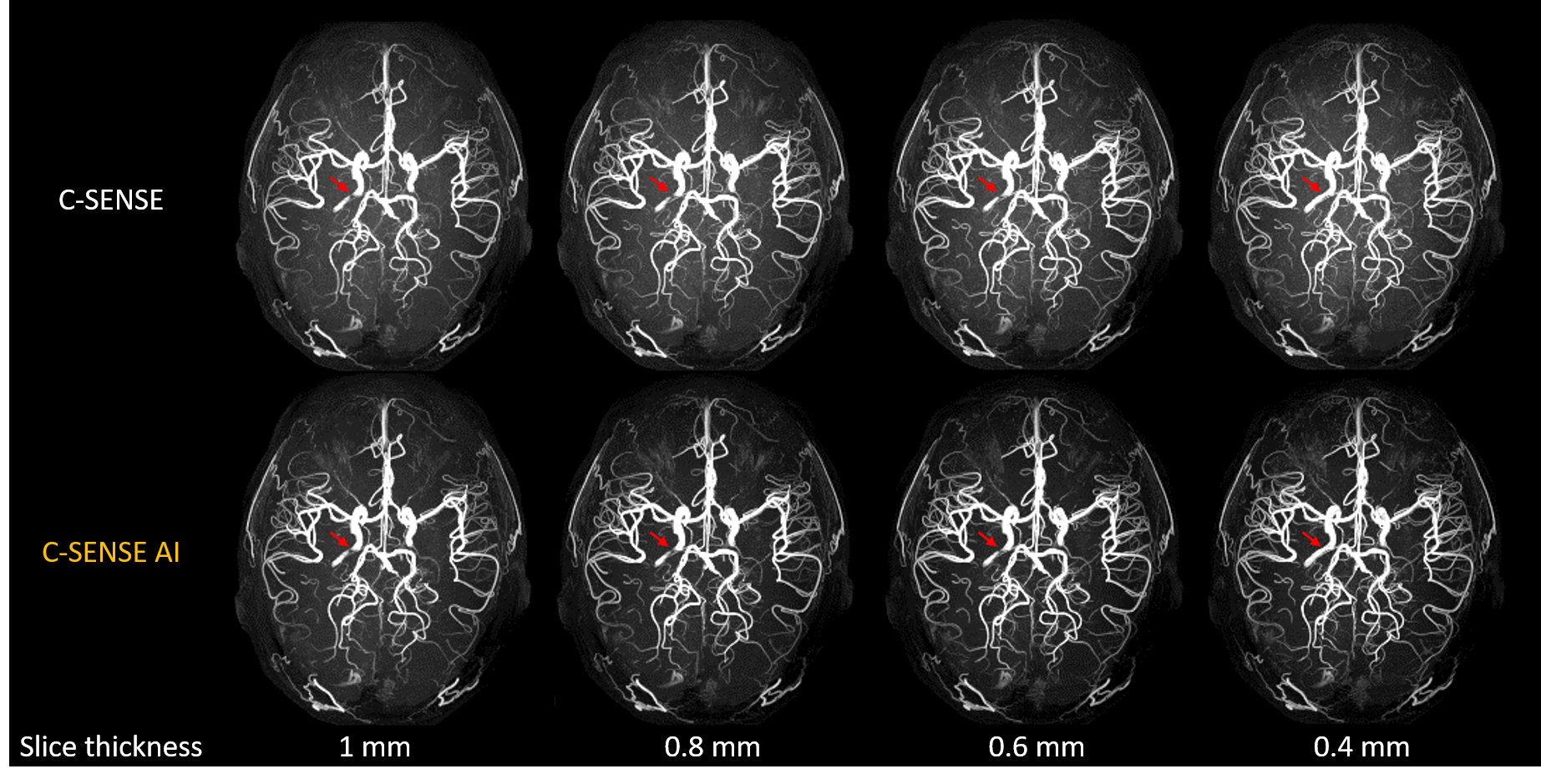
Figure 1 shows the comparison of TOF-MRA between C-SENSE and CS-AI for slice thickness 1.0, 0.8, 0.6, and 0.4 mm. Overall, in C-SENSE, the noise level increased and image quality degraded as the slice thickness reduced. In CS-AI, the noise level did not increase significantly even at 0.4 mm slice thickness.Figure 2 shows the MIP of the TOF-MRA images shown in Fig.1. Because thinner slices can better represent tortuosity of vessels, partial signal loss in the internal carotid artery (red arrows) seen in slices thicker than 0.6 mm was resolved in 0.4 mm. Background noise in CS-AI was visually well suppressed compared to C-SENSE. Figure 3 (b) and (c) show the signal profile for 1.0 and 0.4 mm slices, respectively, along the line drawn in figure 3(a). For both 1.0 and 0.4 mm thicknesses, the baseline signal intensity in CS-AI was lower than that of C-SENSE, while the signal intensity of each peak was higher in CS-AI than C-SENSE. This suggests improved signal-to-noise in CS-AI compared to C-SENSE. The number of vessels detected was 6 and 8 on the 1.0 mm slice, and was 6 and 9 on the 0.4 mm slice for C-SENSE and CS-AI, respectively. This trend was also seen in the other two subjects. This suggests that the improved noise reduction by CS-AI can visualize more vessels compared to C-SENSE, especially when the slice is thinner.
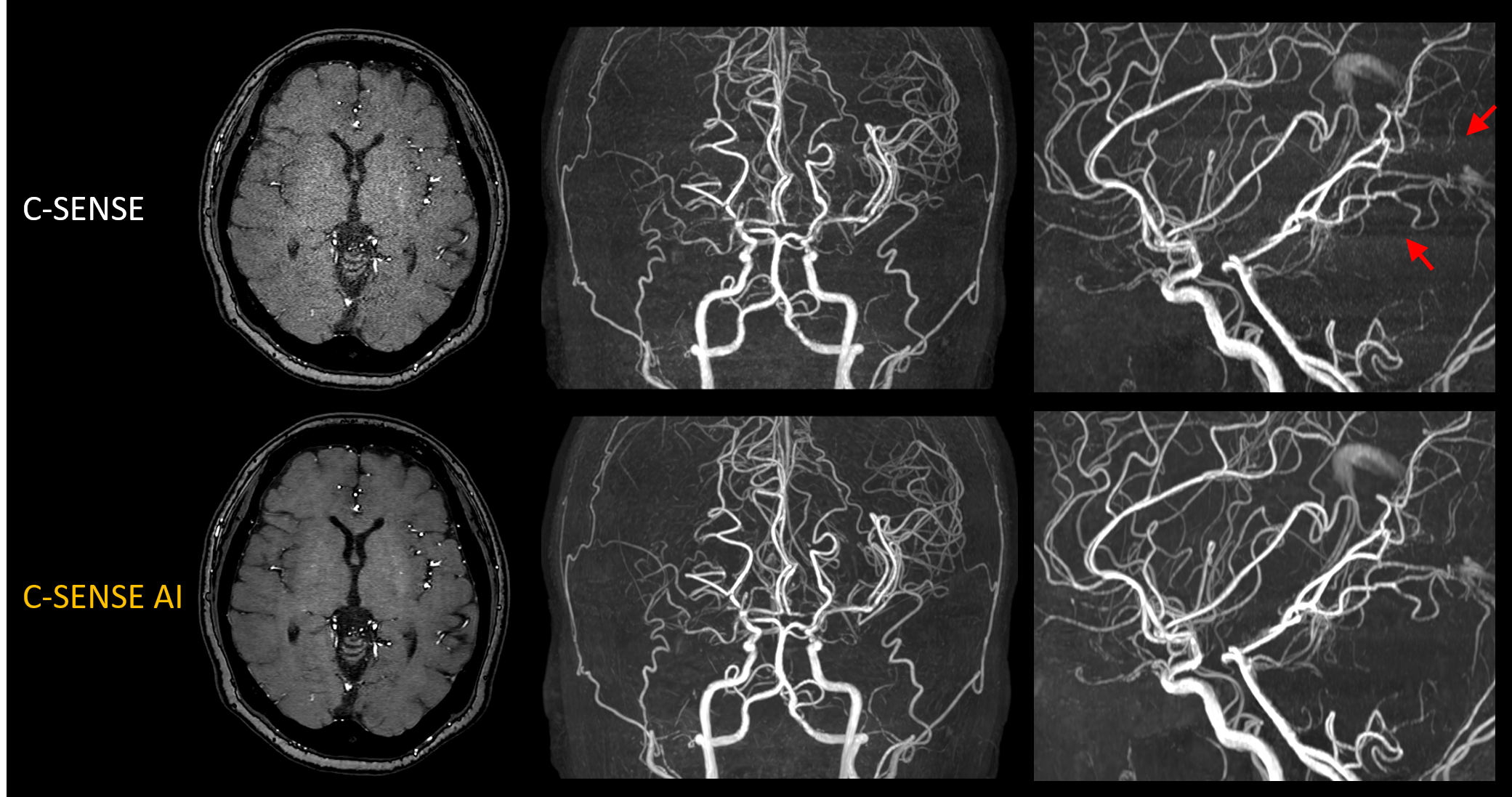
Figure 4 shows the TOF-MRA of the patient with moyamoya disease. CS-AI showed better noise reduction compared to C-SENSE. On the sagittal image, horizontal banding-like artifact was present in C-SENSE (red arrows) but was diminished in CS-AI.
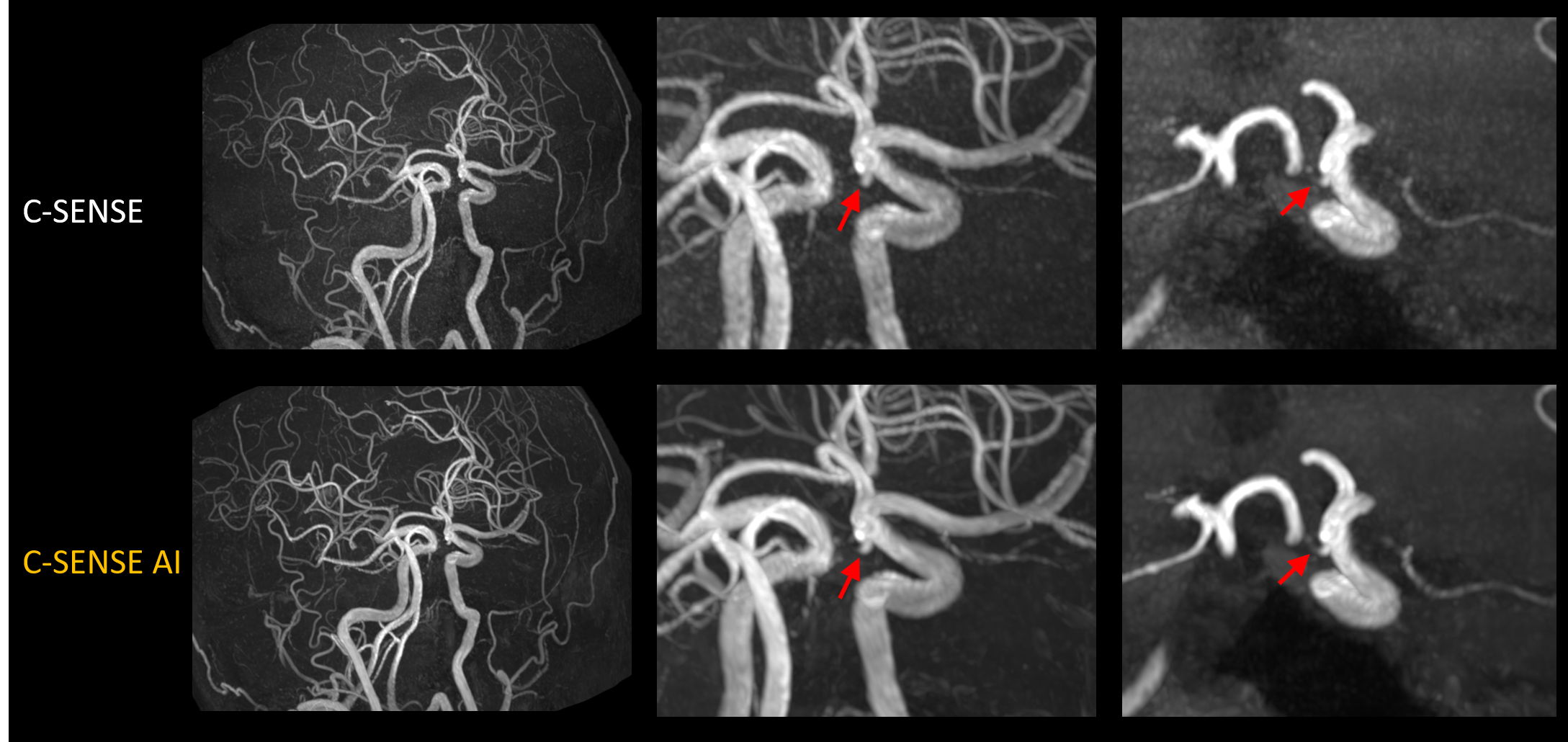
Figure 5 shows the TOF-MRA of the patient with a suspected aneurysm. On C-SENSE it was difficult for clinicians to determine if there was an aneurysm or not (red arrow). But on CS-AI the better delineation of the vessel helped make a diagnosis that it is likely not an aneurysm, but that the vessel is bending towards a confusing direction.
Conclusion
We acquired ultra-thin slice 3D TOF-MRA for the brain using the CS-AI and compared the image quality with the C-SENSE. We showed that the improved noise reduction by CS-AI enabled better visualization of vessels, especially on the thinner slice thicknesses. The usefulness of CS-AI was also demonstrated in clinical cases.Acknowledgements
No acknowledgement found.References
1. Dumoulin CL, Cline HE, Souza SP, Wagle WA, Walker MF. Three‐dimensional time‐of‐flight magnetic resonance angiography using spin saturation. Magn Reson Med. 1989;11(1):35-46. doi:10.1002/mrm.1910110104
2. Pezzotti N, de Weerdt E, Yousefi S, et al. Adaptive-CS-Net: FastMRI with Adaptive Intelligence. arxiv. 2019;(NeurIPS). http://arxiv.org/abs/1912.12259
3. Pezzotti N, Yousefi S, Elmahdy MS, et al. An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction. IEEE Access. 2020;8:204825-204838. doi:10.1109/ACCESS.2020.3034287
Figures