4307
Accelerate Pulmonary Hyperpolarized Gas MRI with Multi-Task Learning1School of Physics, Huazhong University of Science and Technology, Wuhan, China, 2Key Laboratory of Magnetic Resonance in Biological Systems, State Key Laboratory of Magnetic Resonance and Atomic and Molecular Physics, National Center for Magnetic Resonance in Wuhan, Wuhan Institute of Physics and Mathematics, Innovation Academy for Precision Measurement Science and Technology, Wuhan, China
Synopsis
Hyperpolarized gas MRI is a non-invasive and non-radiation imaging modality that can provide lung structure and function information. However, the problem of long imaging time limits its clinical application. Deep learning-based methods have shown great potential to accelerate MRI. In this work, we proposed a multi-task network to perform pulmonary hyperpolarized gas MRI reconstruction and lung region segmentation simultaneously, which allows sharing representations between two tasks. The results show that the proposed multi-task network has better reconstruction performance, stronger robustness and fewer model parameters than the comparison method.
Introduction
Hyperpolarized (HP) gas (such as 3He or 129Xe) MRI can be used for human structural and functional imaging.1 However, HP gas MRI is susceptible to noise or artifacts due to the nonrenewability of HP magnetization. Moreover, most HP gas MRI methods complete the signal acquisition during a single breath-hold, and long-term breath-holding will cause discomfort to the patients. Accordingly, accelerating the acquisition of HP gas MRI is of great significance. Deep learning-based methods have been demonstrated to have significant advantages in accelerating proton MRI.2,3 For HP gas MRI reconstruction, cascaded convolutional neural networks (CNNs) model incorporating prior knowledge of 1H images (called as CasNet) has been proposed.4 However, CasNet mainly performed reconstruction at accelerate factor (AF) of 4 and the reconstruction images lost more fine details with the increase of AF. In this work, we propose a multi-task network that simultaneously learns reconstruction and segmentation tasks. This multi-task network architecture includes an encoder extracting image features and two decoders reconstructing the pulmonary HP gas MR images and segmenting the lung region. The two decoders share the features extracted by the encoder, and the segmentation task focuses on the image edge features. Compared with the single-task reconstruction network (CasNet), the proposed multi-task network can restore more image details at high AFs, effectively improving the reconstruction performance.Methods
Network architectureThe architecture of the proposed multi-task network was presented in Figure 1, which consisted of an encoder (named as Encoder) and two decoders (named as Recon Decoder and Seg Decoder) for simultaneously HP gas MRI reconstruction and lung region segmentation. The zero-filling images as the inputs were fed to the Encoder, and then the features extracted by the Encoder were fed to the Recon Decoder and Seg Decoder. Because the proposed multi-task network learned reconstruction and segmentation at the same time, the Encoder could capture features of two tasks.
The total loss of the network was the sum of the reconstruction loss and the segmentation loss. The reconstruction loss was defined as the mean square error (MSE) between the reconstructed image and its corresponding fully sampled image. The segmentation loss was the Dice loss function, defined as:
$$L_{seg}=1-\frac{2|S_{R}\cap S_{F}|}{|S_{R}|+|S_{F}|}$$where SR is the binary map of the lung region predicted by the network, SF is the binary map of the lung region of the fully sampled image.
Experiments
To evaluate the effectiveness of the proposed multi-task network, 84 subjects in total were enrolled for HP 129Xe MRI reconstruction. The imaging parameters were as follows: repetition time/echo time (TR/TE) = 4.2/1.9 ms, matrix size = 96 × 96, number of slices = 24, slice thickness = 8 mm, flip angle (FA) = 10°, scan time = 8.4 s. After acquiring the HP 129Xe MR images, slices with SNR below 6.6 were removed to confirm image quality. In this way, we obtained a total of 929 HP 129Xe MR images. Then we selected 10% of the images for training and the others for testing. The lung region mask was segmented by the seeded region growing and manual correction. Cartesian undersampling method was used in this work and the AFs were 4, 5, and 6. Peak signal-to-noise ratio (PSNR) and structure similarity (SSIM) were adopted to quantitatively evaluate the image reconstruction quality.
Results
Figure 2 visually presented reconstruction results for different slices of randomly selected test images from testing set, which demonstrated that our proposed multi-task network yielded visually better results than CasNet at different AFs. As shown in Figure 3, the proposed multi-task network outperformed CasNet in terms of PSNR for all test data at AF of 4, 5, and 6, and the increases were 3.54% (31.4688 ± 2.6470 vs 30.3923 ± 2.5939), 3.78% (30.8794 ± 2.6008 vs 29.755 ± 2.4989) and 4.93% (29.7824 ± 2.6393 vs 28.3842 ± 2.5607) . In addition, the proposed method also had better SSIM compared to CasNet, and the increases at AF of 4, 5, and 6 were 2.46% (0.8557 ± 0.0336 vs 0.8352 ± 0.0362), 2.90% (0.8312 ± 0.0418 vs 0.8078 ± 0.0436) and 3.76% (0.8081 ± 0.0487 vs 0.7788 ± 0.0511), respectively. As for the number of parameters, the proposed network (72 M) was 23.40% less than CasNet (94 M).Discussion and Conclusion
The visual results show that the images reconstructed by the proposed method preserve more texture details and are closer to the ground truth than that reconstructed by CasNet. This means that training the two tasks of segmentation and reconstruction at the same time can learn more image features. The quantitative results show that the proposed method has higher PSNR and SSIM than CasNet. Moreover, the increments of PSNR and SSIM increase with the increase of AF. This indicates that the proposed method is more robust than CasNet. Under the constraint of segmentation loss, the multi-task network pays more attention to the image edges, so it can retain more image details at high AFs. In addition, the proposed multi-task network has fewer model parameters than CasNet, which is mainly due to the two decoders share the features extracted by one encoder. Therefore, training/reconstruction time is greatly reduced and the overfitting problem can be prevented.Acknowledgements
This work was supported by the National Natural Science Foundation of China (91859206, 81625011, 21921004, 82001915), the National key Research and Development Project of China (2018YFA0704000) and the Key Research Program of Frontier Sciences (ZDBS-LY-JSC004). Xin Zhou acknowledges the support from the Tencent Foundation through the XPLORER PRIZE.
References
1. Albert MS, Cates GD, Driehuys B, et al. Biological magnetic resonance imaging using laser-polarized 129Xe. Nature. 1994; 370(6486):199-201.
2. Eo T, Jun Y, Kim T, et al. KIKI-net: cross-domain convolutional neural networks for reconstructing undersampled magnetic resonance images. Magn Reson Med. 2018; 80(5):2188-2201.
3. Zhou W, Du H, Mei W, et al. Efficient structurally-strengthened generative adversarial network for MRI reconstruction. Neurocomputing. 2021; 422:51-61.
4. Duan C, Deng H, Xiao S, et al. Fast and accurate reconstruction of human lung gas MRI with deep learning. Magn Reson Med. 2019; 82(6):2273-2285.
Figures
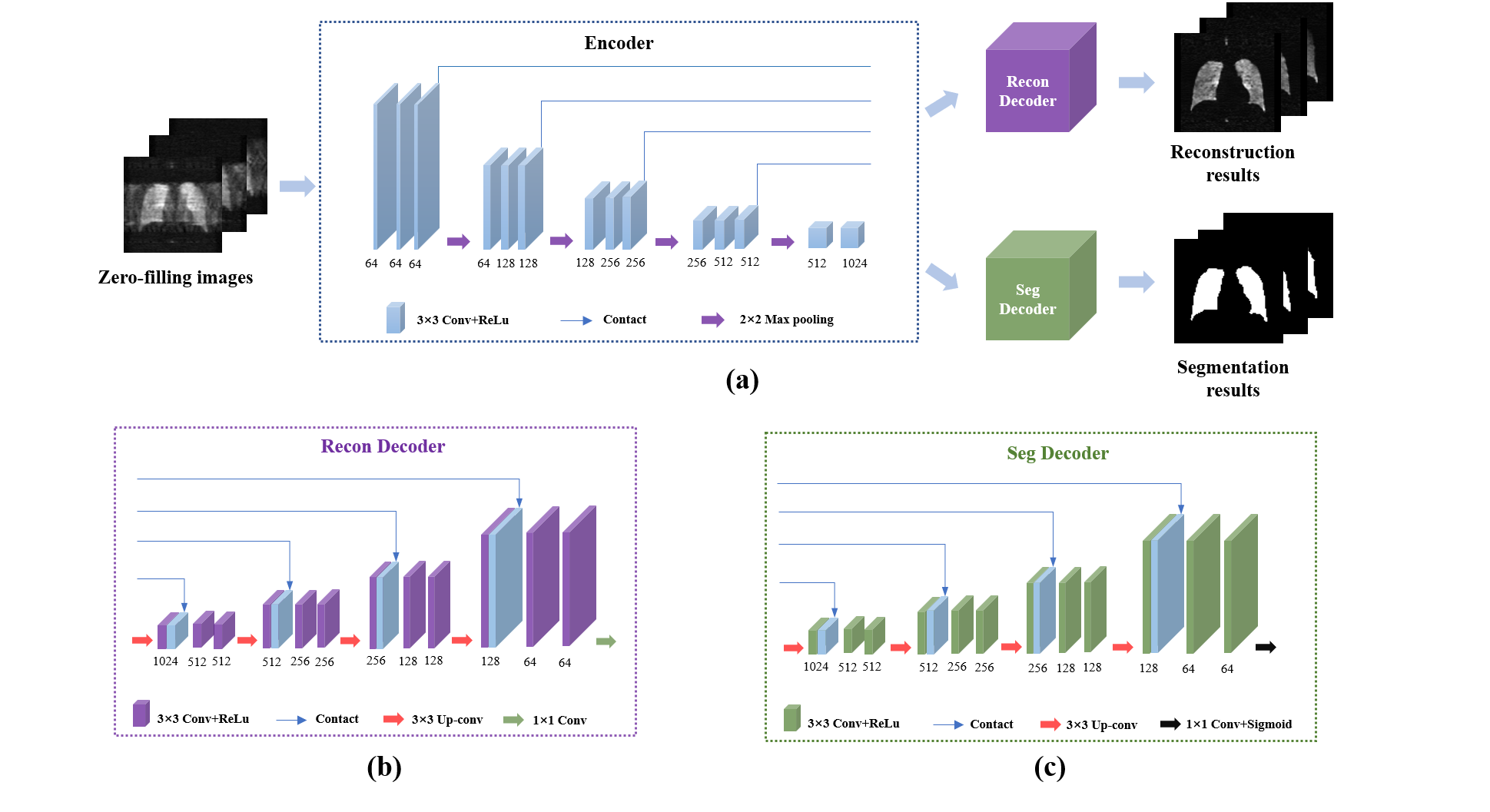
Figure 1. The architecture of the proposed multi-task network. (a) The overall architecture of the proposed network. The network consists of three parts: an encoder that allows sharing features between two tasks, a decoder for reconstruction task (Recon Decoder), and another decoder for segmentation task (Seg Decoder). (b) The architecture of the Recon Decoder. (c) The architecture of the Seg Decoder.
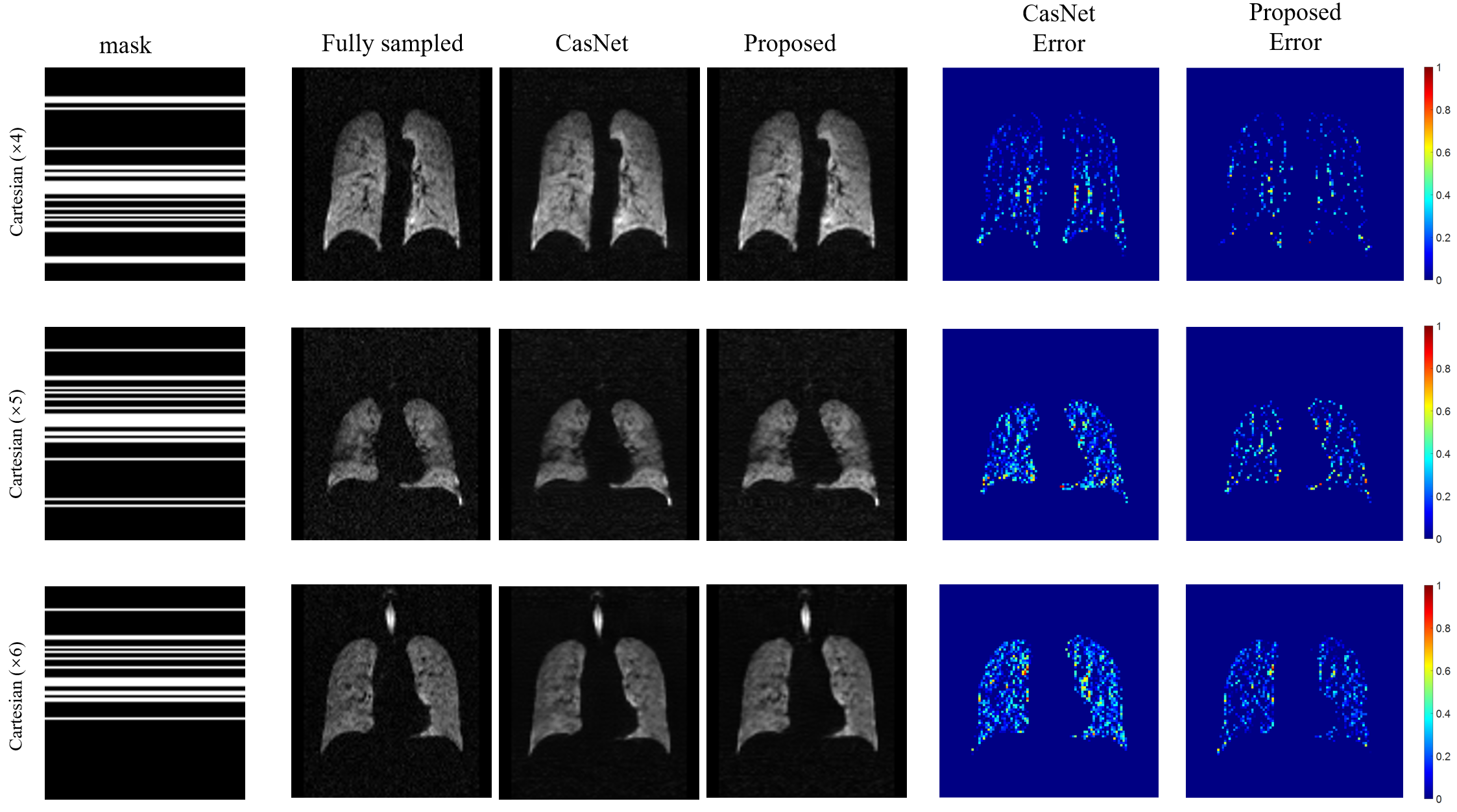
Figure 2. Reconstruction results of CasNet and the proposed network at different accelerate factors. The proposed network has lower reconstruction error than CasNet.
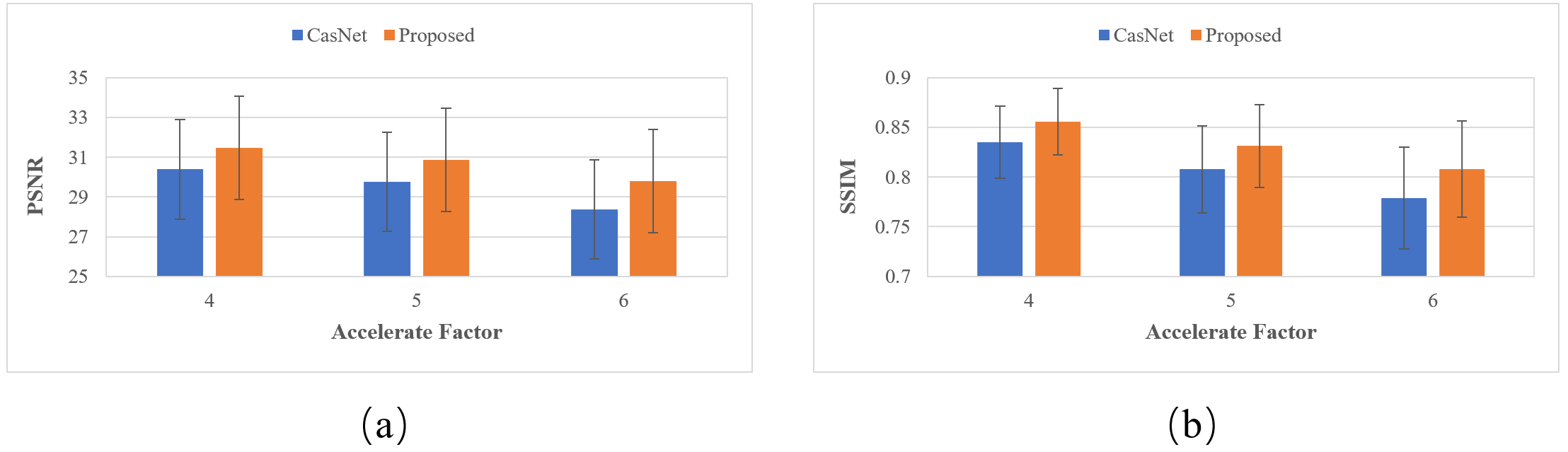
Figure 3. Quantitative comparison between CasNet and the proposed network. (a) PSNR of the results acquired by CasNet and the proposed network. (b) SSIM of the results acquired by CasNet and the proposed network.