4303
Rapid 3D MR cholangiopancreatography in a breath-hold using deep learning constrained Compressed SENSE reconstruction1Department of Radiology, West China Hospital of Sichuan University, Chengdu, China, 2Clinical Science, Philips Healthcare, Chengdu, China
Synopsis
In this work, we aimed to use a deep learning based Compressed SENSE reconstruction algorithm, presented here as Artificial Intelligence Compressed-SENSE (AI-CS), to improve image quality of 3D magnetic resonance cholangiopancreatography (MRCP) in a breath hold (BH). The results demonstrated that AI-CS BH MRCP can enable improved image quality and show great visibility of small ductal structures than other previous methods.
Introduction
Three dimensional (3D) magnetic resonance cholangiopancreatography (MRCP) is a reliable imaging method that allows for the non-invasive evaluation of pancreaticobiliary system in clinics. However, integrating respiratory-triggered (RT) 3D MRCP in routine clinical protocols has been challenging, due to its lone acquisition time of 3-6 minutes and proneness to image motion and blurring artifacts. Two novel single breath-hold (BH) alternatives, gradient and spin-echo (GRASE) sequence based technique1 and compressed-sensing (CS) based technique2 have been proposed to accelerate the scanning speed of MRCP. Though both the two single breath-hold alternatives have been reported to provide promising results3, they are still inadequate for the display of small ductal structures compared with respiratory-navigated MRCP4,5. Recently, artificial intelligence (AI) has been applied for MRI reconstruction. A novel adaptive-CS-Network, presented here as a AI-CS reconstruction is sufficiently powerful to directly reconstruct the undersampled k-space data and demonstrated the superior performance in knee MRI reconstruction6. We hypothesized that AI-CS would enable rapid 3D MRCP in one breath hold with improve image quality, especially duct visualization. Thus, we intend to compare qualitative and quantitative image quality among GRASE-BH MRCP, CS-BH MRCP, AI-CS-BH MRCP and respiratory-triggered MRCP.Methods
The study was approved by the institutional ethics committee. A total of 22 patients (mean age 49.86 ± 17.68 years) with suspected biliary and pancreatic disorders underwent MR examinations on a 3T MR system (Ingenia Elition X, Philips Healthcare) using a 16-element phased-array coil. MR images were obtained using GRASE-BH MRCP, CS-BH MRCP, AI-CS-BH MRCP and respiratory-triggered MRCP. The detailed acquisition parameters were shown as following:(1) GRASE: TR/TE = 1800/390 ms, field of view(FOV) = 350×295×100 mm2, voxel size = 0.59×0.59×1 mm3, NSA = 1, acquisition time (TA) = 16 s; (2) CS: TR/TE = 227/87 ms, FOV = 300×300×100 mm2, voxel size = 0.59×0.59×1 mm3, NSA = 1, CS acceleration factor = 24, TA = 16 s; (3)AI-CS: TR/TE = 227/87 ms, FOV = 300×300×100 mm2, voxel size = 0.59×0.59×1 mm3, NSA = 1, CS acceleration factor = 24, TA= 16 s; (4)RT: TR/TE = 900/600 ms, FOV = 300×300×100 mm2, reconstruction voxel size =0.59×0.59×1 mm3, NSA = 1, TA = 4 min 33 s; In AI-CS approach, the CS reconstruction chain is merely replaced by a convolution neural network (CNN) reconstruction6.Qualitative image evaluation was performed using a 5-point Likert-type scale (5= excellent, 4 = good, 3 = moderate, 2 = poor, 1 = nondiagnostic) in the following categories: overall image quality, artifacts, background suppression and duct visualization of common bile duct, right hepatic duct, anterior branch, posterior branch, left hepatic duct, medial branch, lateral branch, pancreatic duct. For quantitative objective assessment, signal-to-noise ratio (SNR) of the common bile duct (CBD), contrast-to-noise ratio (CNR) of the CBD and liver, and contrast ratio (CR) between periductal tissue and the CBD were measured on the source images. The Friedman test with a post-hoc test was used for statistical analysis. A p-value less than 0.05 was considered as a significant difference.
Results
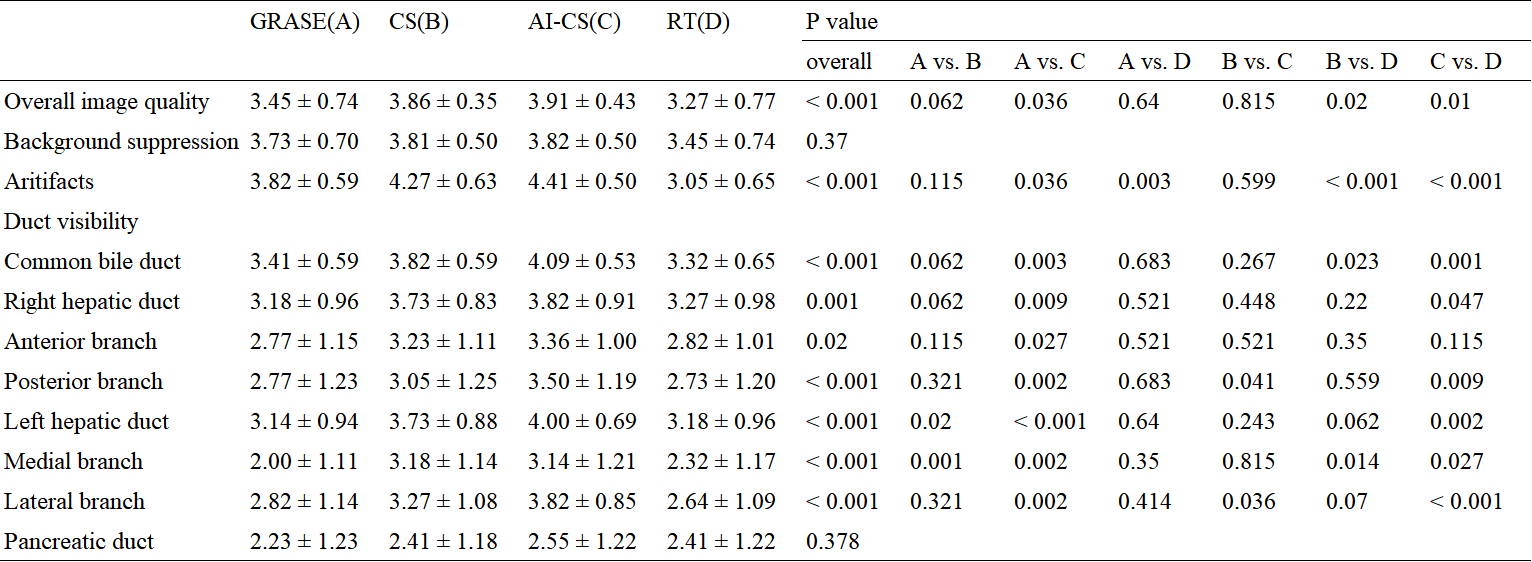
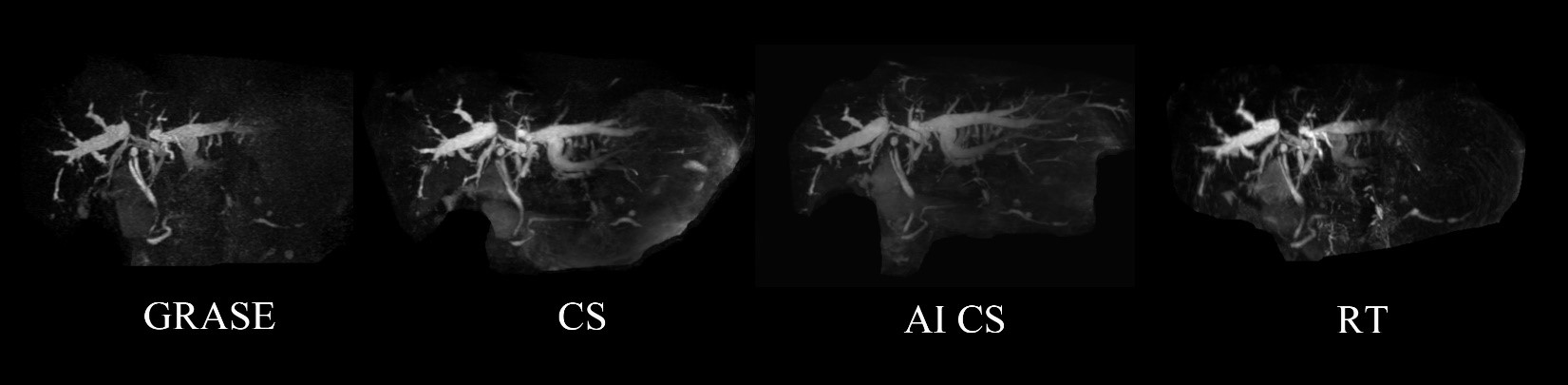
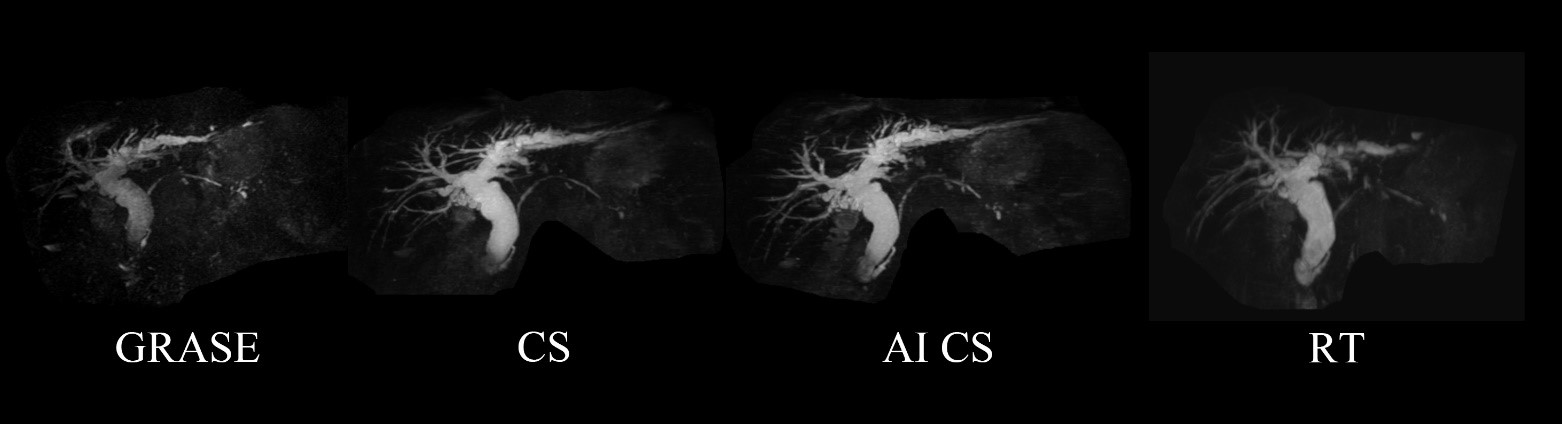
The duct visualization of right hepatic duct posterior branch and left hepatic duct lateral branch were rated significantly highest image score with AI-CS-BH MRCP, followed by CS-BH MRCP, RT-MRCP and GRASE-BH MRCP (p all < 0.05) (Table 1 & Figure 1). The scores with AI-CS-BH MRCP for overall image quality, artifacts, duct visualization of CBD, right hepatic duct, left hepatic duct and left hepatic duct medial branch were also significantly higher than RT MRCP and GRASE-BH MRCP (p all < 0.05) (Table 1 & Figure 2). The duct visualization of right hepatic duct posterior branch with AI-CS-BH MRCP was also rated higher image score than GRASE-BH MRCP (p < 0.05). Background suppression and pancreatic duct didn’t show significant differences among the four imaging modalities.The SNR of the CBD with AI-CS BH MRCP was higher than RT MRCP and GRASE-BH MRCP ( 24.50 ± 2.34 vs. 18.70 ± 2.33 , p = 0.036; 24.50 ± 2.34 vs. 11.26 ± 1.09 , p < 0.05) (Table 2). The CR between periductal tissue and the CBD, and CNR between the CBD and liver with AI-CS BH MRCP were higher than GRASE-BH MRCP (p < 0.05) (Table 2).
Discussion and Conclusion
This study demonstrated that AI-CS BH MRCP was able to provide better image quality than CS-BH MRCP, RT MRCP and GRASE BH MRCP. Although CS-BH MRCP has been reported as an alternative method of RT MRCP, it is still inadequate for visibility of small ductal structure4. The combination of CS and novel AI can enable improved image quality and show great visibility of small ductal structures than other three sequence, especially in secondary intrahepatic duct.Acknowledgements
No acknowledgement found.References
1. Nam JG, Lee JM, Kang HJ, et al. GRASE Revisited: breath-hold three-dimensional (3D) magnetic resonance cholangiopancreatography using a Gradient and Spin Echo (GRASE) technique at 3T. Eur Radiol. 2018;28(9):3721-3728.
2. Feng L, Benkert T, Block KT, et al. Compressed sensing for body MRI. J Magn Reson Imaging. 2017;45(4):966-987.
3. Henninger B, Steurer M, Plaikner M, Weiland E, Jaschke W, Kremser C. Magnetic resonance cholangiopancreatography with compressed sensing at 1.5 T: clinical application for the evaluation of branch duct IPMN of the pancreas. Eur Radiol. 2020;30(11):6014-6021.
4. Lohöfer FK, Kaissis GA, Rasper M, et al. Magnetic resonance cholangiopancreatography at 3 Tesla: Image quality comparison between 3D compressed sensing and 2D single-shot acquisitions. Eur J Radiol. 2019;115:53-58.
5. Zhu L, Wu X, Sun Z, et al. Compressed-Sensing Accelerated 3-Dimensional Magnetic Resonance Cholangiopancreatography: Application in Suspected Pancreatic Diseases. Invest Radiol. 2018;53(3):150-157.
6. Pezzotti N, Yousefi S, Elmahdy M.S, et al. An adaptive intelligence algorithm for undersampled knee MRI reconstruction. IEEE Access 8, 2020;204825–204838.
Figures