4299
New Diagnosis Criteria for Hepatocellular Carcinoma: Gadoxetic Acid-enhanced MRI Integrating CT-Vascular Features May Facilitate Evaluation1Department of Radiology, West China Hospital, Sichuan University, Chengdu, China, 2GE Healthcare China, Beijing, China
Synopsis
Gadoxetic acid-enhanced magnetic resonance imaging (MRI) has been widely used in detection and diagnosis for hepatocellular carcinoma (HCC), while transient severe motion artifact that affects the arterial phase (AP) images quality and reduces diagnosis performance remains a concern. A new diagnosis criterion for HCC integrating CTAP and MRAP images was introduced in this study and achieved a high sensitivity and comparable specificity when compared with the gadoxetic acid-enhanced MRI only. It may be able to improve the diagnostic performance of gadoxetic acid-enhanced MRI in patients with HCCs and further affect the clinical treatment plan.
Introduction
Despite the great advantages of gadoxetic acid-enhanced magnetic resonance imaging (MRI) in diagnosis for hepatocellular carcinoma (HCC), particularly in small HCCs, the transient severe dyspnea-related motion artifact in the arterial phase (AP) still remains a serious concern which may reduce the detection of HCC1. Arterial phase hyperenhancement (APHE) is recommended as the major imaging feature in most dominating guidelines owing to its high sensitivity2-4. In addition, it can reach the optimal diagnostic efficiency when combined with the feature of portal venous phase (PVP) or delayed phase (DP) hypointensity4,5. Given that the importance of the AP in diagnosing HCC, it is an urgent challenge for bridging the gap between transient severe motion artifact and the AP image quality. At present, several strategies have been used to overcome this limitation and are divided into two categories. One is the reduction of the incidence rate of transient severe dyspnea by lowering the injection rate, diluting the contrast agent, or performing respiratory exercises before MR examination6,7. The other is the honing of the MR technique by shortening the scanning time, using a free breath-hold MR sequence, or acquiring multiple AP images8-10. However, once transient severe dyspnea occurs, the AP images cannot be guaranteed in these methods. Previous studies investigated the combined use of MR and computed tomography (CT) imaging features for improving the diagnostic performance of LI-RADS, or found a comparable diagnostic performance of an abbreviated MR protocol +CT features with full MR sequences set11, 12, 13. To our knowledge, few studies have investigated whether the vascular features of dynamic-enhanced CT can be used as an alternative for those of gadoxetic acid-enhanced MRI, or further validate whether the combination can improve the diagnostic performance when compared with gadoxetic acid-enhanced MRI only. Therefore, this study aims to determine whether the integrating use of vascular features on dynamic-enhanced CT can facilitate the diagnosis of HCC based on various diagnostic criteria when compared with the gadoxetic acid-enhanced MRI sequences.Methods
This study was approved by the institutional review board. 142 patients with 169 surgically confirmed nodules (137 HCCs and 32 non-HCCs) were retrospectively included and underwent both gadoxetic acid-enhanced MRl in 3.0 T MR systems and dynamic-enhanced CT in multidetector CT scanners preoperatively. All the images were anonymized and then integrated as two different protocols sets: 1) Protocol-I: full gadoxetic acid-enhanced MRI sequences; 2) Protocol-II: dynamic CT + gadoxetic acid-enhanced MRI but excluding the vascular features related phase (AP) MR images. Three independent reviewers who were blinded to the histopathological and clinical data characterized the nodules according to the 2018 Liver Imaging Reporting and Data System (LI-RADS v2018), European Association for the Study of the Liver (EASL), and 2018 Korean Guidelines. The clinical impact of CTAP and MRAP images for detecting APHE, the diagnostic performance for HCC in L-RADS v2018, EASL and Korean guidelines for combined images (Protocol-II) and MR-only images (Protocol-I) were analyzed and compared. A two-sided p-value of <0.05 indicated statistical significance.Results
For the whole hepatic nodules, CTAP-combined images had a significantly higher detection rate for APHE than the MRAP images (87.57% [148/169] vs.75.15% [127/169; p<0.001). In the subgroup analysis the CTAP-combined images showed significant higher APHE detection rate than MRAP images (97.08% [133/137]vs.82.48%[113/137):p<0.001). For the LI-RADS (Figure 1), the CTAP-combined images significantly raised the sensitivity to 75.91% (104/137) from 70.80% (97/137) on MRAP images (p=0.016), with a minimal decrease of the specificity to 71.88% (23/32) from 75.00% (24/32) (p=1.000). For the EASL (Figure 2), MRAP images achieved a sensitivity of 78.10% (107/137) and a specificity of 71.88%(23/32) for diagnosing HCC. However, when determining APHE on the CTAP, the sensitivity showed numerical increase to 81.02% (111/137) (p=0.152), whereas the specificity decreased to 75.00% (24/32) which was not statistically significant either, p=1.000). For the Korean criteria (Figure 3), the CTAP-combined images substantially increased the sensitivity to 94.89% (130/137) from 83.21% (114/137) on the MRAP images(p<0.001).Discussion
In the study, we introduced a new diagnosis criterion for HCC integrating CTAP and MRAP images and explored whether it could improve the diagnostic performance of the various guideline criteria. The results demonstrated that compared with the MR images only, the CTAP images had a significantly higher detection rates for APHE in both the total nodules and HCC, which was similar to Park et al13 and can be attributed to the following explanations: high frequency of transient serve motion in gadoxetic acid-enhanced MRI, the degree of MRI enhancement following contrast agent is closely related to the amount and relaxation rate of contrast agent, and more importantly, Gd-EOB-DTPA is a dual channel excretory contrast agent. In addition, the results also found that the combination of vascular features on CTAP could significantly improve sensitivity for HCC diagnosis on various criteria (LI-RADS, EASL, and Korean guidelines), particularly for LR-4/5 and the 2018 Korean Guideline. It also exhibited the gratifying result that the specificity of the diagnosis was almost unaffected using this approach.Conclusion
To conclude, the new diagnosis criterion for HCC that integrating CTAP and MRAP images enables a high sensitivity and comparable specificity when compared with the gadoxetic acid-enhanced MRI only, which may further help for the clinical management.Acknowledgements
No acknowledgement found.References
1. Bashir MR, Castelli P, Davenport MS, et al. Respiratory motion artifact affecting hepatic arterial phase MR imaging with gadoxetate disodium is more common in patients with a prior episode of arterial phase motion associated with gadoxetate disodium. Radiology 2015;274:141-8.
2. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology 2011;53:1020-2. 3. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. Eur J Cancer 2012;48:599-641.
4. Radiology. ACo. CT/MRI LI-RADS v2018 core. https:// www.acr.org/-/media/ACR/Files/RADS/LI-RADS/LI-RADS-2018-Core.pdf? Accessed December 4 2018.
5. Chernyak V, Flusberg M, Berman J, et al. Liver Imaging Reporting and Data System Version 2018: Impact on Categorization and Hepatocellular Carcinoma Staging. Liver Transpl 2019;25:1488-502.
6. Davenport MS, Viglianti BL, Al-Hawary MM, et al. Comparison of acute transient dyspnea after intravenous administration of gadoxetate disodium and gadobenate dimeglumine: effect on arterial phase image quality. Radiology 2013;266:452-61.
7. Haradome H, Grazioli L, Tsunoo M, et al. Can MR fluoroscopic triggering technique and slow rate injection provide appropriate arterial phase images with reducing artifacts on gadoxetic acid-DTPA (Gd-EOB-DTPA)-enhanced hepatic MR imaging? J Magn Reson Imaging 2010;32:334-40.
8. Lee SS, Byun JH, Hong HS, et al. Image quality and focal lesion detection on T2-weighted MR imaging of the liver: comparison of two high-resolution free-breathing imaging techniques with two breath-hold imaging techniques. J Magn Reson Imaging 2007;26:323-30.
9. Ikram NS, Yee J, Weinstein S, et al. Multiple arterial phase MRI of arterial hypervascular hepatic lesions: improved arterial phase capture and lesion enhancement. Abdom Radiol (NY) 2017;42:870-6.
10. Min JH, Kim YK, Kang TW, et al. Artifacts during the arterial phase of gadoxetate disodium-enhanced MRI: Multiple arterial phases using view-sharing from two different vendors versus single arterial phase imaging. Eur Radiol 2018;28:3335-46.
11. Basha MAA, AlAzzazy MZ, Ahmed AF, et al. Does a combined CT and MRI protocol enhance the diagnostic efficacy of LI-RADS in the categorization of hepatic observations? A prospective comparative study. Eur Radiol 2018;28:2592-603.
12. Kim M, Kang TW, Cha DI, et al. Identification of Arterial Hyperenhancement in CT and MRI in Patients with Hepatocellular Carcinoma: Value of Unenhanced Images. Korean J Radiol 2019;20:236-45.
13. Park SH, Kim B, Kim SY, et al. Abbreviated MRI with optional multiphasic CT as an alternative to full-sequence MRI: LI-RADS validation in a HCC-screening cohort. Eur Radiol 2020;30:2302-11.
Figures
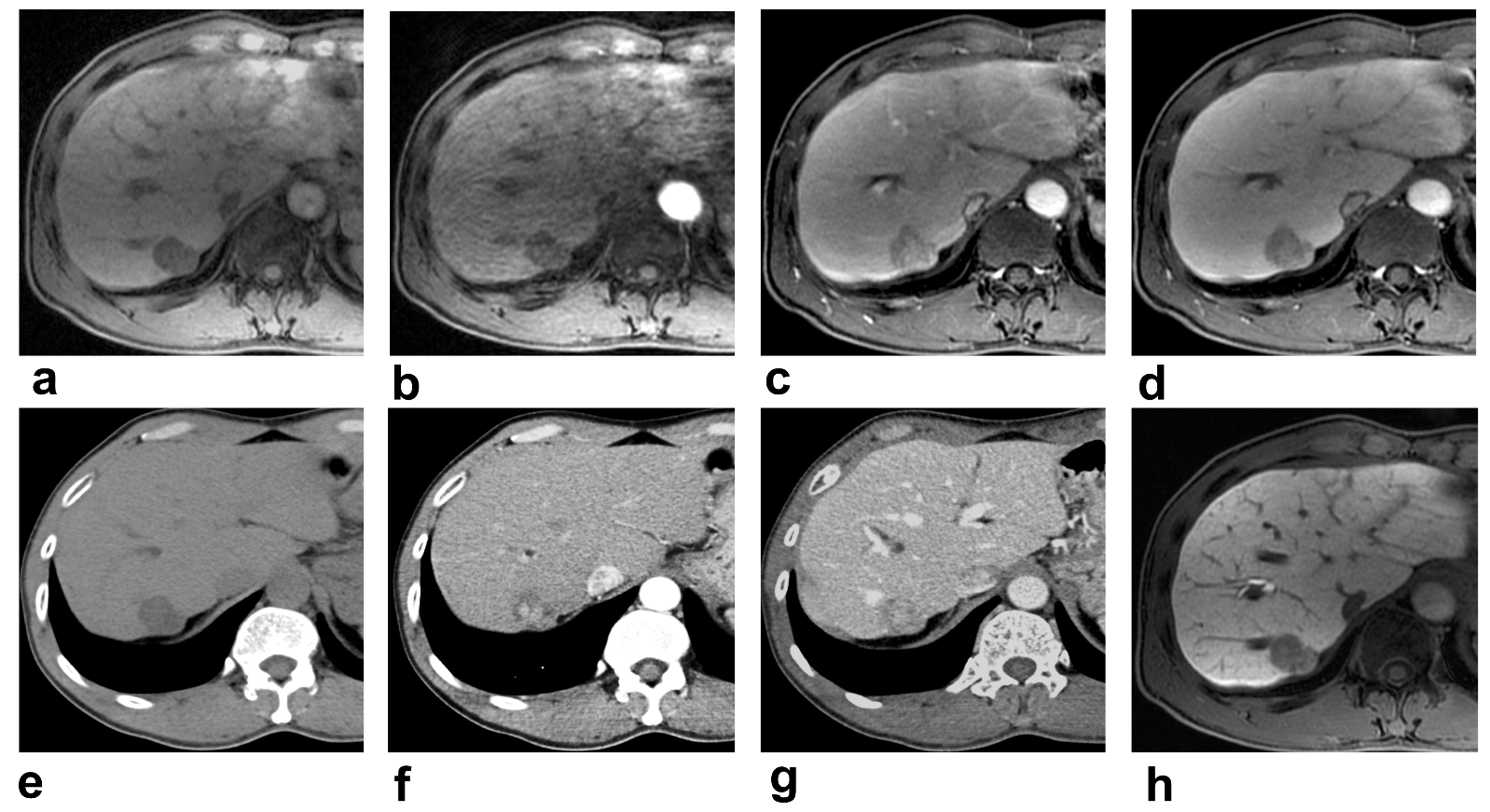
Figure 1. Histologically confirmed HCC in a 55-year-old man.
On MR images: (a) The plain MR image: hypointensity lesion (>2 cm) on the right liver lobe. (b, c) AP, PVP MR images: No typical APHE. Nonperipheral washout is obtained. (d) DP MR image: Typical nonperipheral washout. (h) Hepatobiliary phase MR image: hypointensity.
On CT images: (e) The plain CT image: A hypointensity lesion. (f) AP CT image: APHE. (g) PVP CT image: No typical nonperipheral washout.
Thus, using the LI-RADS v 2018, the lesion was categorized as LR-4 on MR-only images, but as LR-5 on the CTAP-combined images.
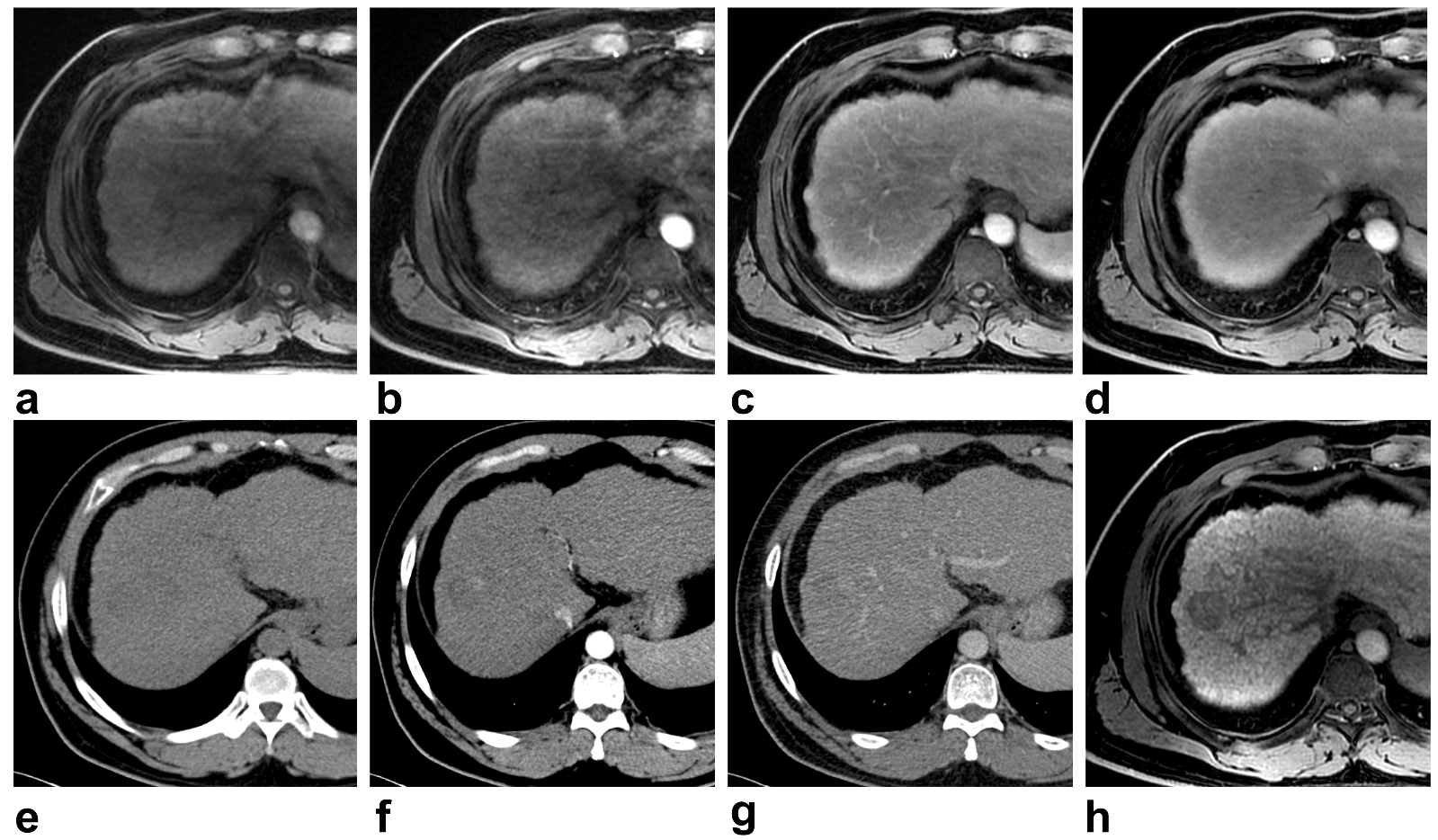
Figure 2. Histologically confirmed HCC in a 43-year-old man.
On MR images: (a) The plain MR image: hypointensity lesion (>2 cm) on the right liver lobe. (b) AP MR image: No typical APHE. (c, d) PVP, DP MR images: Nonperipheral washout and enhancing capsule. (h) Hepatobiliary phase MR image: hypointensity.
On CT images: (e) The plain CT image: A hypointensity lesion. (f) AP CT image: Nodular APHE. (g) PVP CT image: No typical nonperipheral washout.
Thus, using the EASL, the lesion was categorized as non-HCC on MR-only images, but as HCC on the CTAP-combined images.
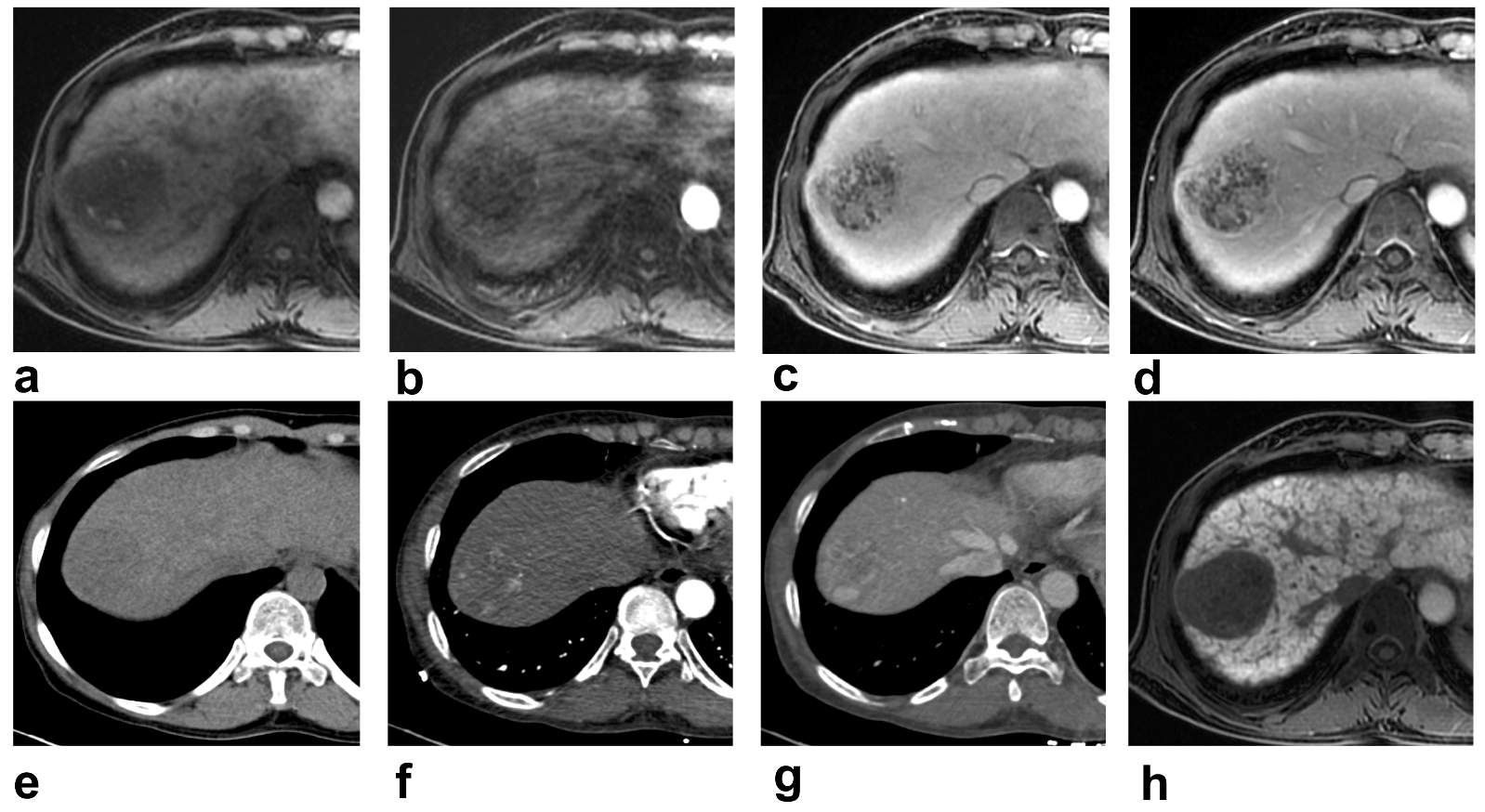
Figure 3. Histologically confirmed HCC in a 49-year-old woman.
On MR images: (a) The plain MR image: hypointensity lesion on the right liver lobe. (b) AP MR image: No typical APHE. (c, d) PVP, DP MR images: Nonperipheral washout. (h) Hepatobiliary phase MR image: Homogenous hypointensity.
On CT images: (e) The plain CT image: A hypointensity lesion. (f) AP CT image: Nodular APHE. (g) PVP CT image: No typical nonperipheral washout.
Thus, using the Korean criteria, the lesion was categorized as non-HCC on MR-only images, but as HCC on the CTAP-combined images.