4262
Diagnostic values and agreement of Gadoxetic Acid-enhanced MRI and Dual Tracer PET/CT (18F-FDG and 11C-Acetate) in Hepatocellular carcinoma
Solomon Yig-Joon Ka1, Gladys Goh Lo1, Christine Shing Yen Lo1, and Cindy Xue2,3
1Department of Diagnostic & Interventional Radiology, Hong Kong Sanatorium and Hospital, Hong Kong, Hong Kong, 2Research Department, Hong Kong Sanatorium and Hospital, Hong Kong, Hong Kong, 3Department of Imaging and Interventional Radiology, The Chinese University of Hong Kong, Hong Kong, Hong Kong
1Department of Diagnostic & Interventional Radiology, Hong Kong Sanatorium and Hospital, Hong Kong, Hong Kong, 2Research Department, Hong Kong Sanatorium and Hospital, Hong Kong, Hong Kong, 3Department of Imaging and Interventional Radiology, The Chinese University of Hong Kong, Hong Kong, Hong Kong
Synopsis
The diagnoses of hepatocellular carcinoma (HCC) are mostly made at advanced stage, which is associated with unfavorable prognosis and suboptimal survival. While dual-tracer PET/CT (dt-PET/CT) and gadoxetic acid-enhanced MRI are effective in detecting liver lesions, diagnostic performance of gadoxetic acid-enhanced MRI in identifying small HCC lesions compared with dt-PET/CT remains unclear. Here, we compare the sensitivity and specificity of each imaging modality to diagnose HCC. Gadoxetic acid-enhanced MRI has higher sensitivity in detecting HCC lesions than using dt-PET/CT, especially in smaller HCC lesions. Thus, gadoxetic acid-MRI could provide clinical value in the early diagnosis of HCC.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer and the 6th most common cancer globally, with 840,000 new cases per year [1]. The diagnoses of HCC are mostly made at the advanced stage, which is associated with unfavorable prognosis and suboptimal survival [1]. While dual-tracer PET/CT with 18F-fluorodeoxyglucose (FDG) and 11C-acetate (ACT) (dt-PET/CT) demonstrates improved sensitivity in detecting HCC lesions [2], gadoxetic acid-enhanced MRI is effective in detecting small liver lesions [3]. However, the diagnostic performance of gadoxetic acid-enhanced MRI in identifying small HCC lesions compared with dt-PET/CT remains unclear. In this study, we ought to compare the performance of gadoxetic acid-enhanced MRI and dt-PET/CT in detecting HCC.Materials and Methods
A total of 48 patients (Female: 16, Male: 32; mean age= 60.2 years old [range: 25-93]) with liver nodules suspicious of HCC, and/or HBV carrier who had undergone both gadoxetic acid-enhanced MRI and dt-PET/CT at the Hong Kong Sanatorium Hospital, were retrospectively included. The interval between two scans should be less than six months. The diagnosis of HCC was obtained by either histopathology results after percutaneous biopsy/ surgical resection and/or based on radiological hallmark in gadoxetic acid-enhanced MRI and dt-PET/CT examination. Only lesions with measurement results from both imaging modalities were included in this study. HCC lesions were categorized into two classes: (1) large HCC lesion (≥2 cm) (2) small HCC lesion (< 2cm).The sensitivity and specificity of each imaging modality to diagnose HCC were calculated and compared using McNemar’s test. Student T-test was conducted to compare the size of the lesions detected using both imaging modalities. A P-value smaller than 0.05 indicated statistical significance. All statistical tests were conducted using Microsoft Excel and SPSS ver. 20.
Results
In total, there were 79 HCC lesions found in 33 patients. There were no significant differences in the sensitivities in detecting HCC lesions using gadoxetic acid-enhanced MRI (72.2% (57/79)) or using dt-PET/CT (69.65 (55/79)) (P=0.883). Both imaging modalities obtained 100% specificity, with no false-positive findings found using either imaging modality.The average size of the HCC lesions detected using gadoxetic acid-enhanced MRI (1.77±1.54cm) was significantly smaller than the average size detected using dt-PET/CT (3.14±2.65cm) (P<0.05). The sensitivities of gadoxetic acid-enhanced MRI in detecting (1) large HCC lesions and (2) small HCC lesions were 69.7% and 78.9%, respectively, whereas those achieved by dual-tracer PET/CT were 87.9% (1) and 64.9% (2). The differences in sensitivity in detecting HCC lesions in both size classes were not significant ((1)P=0.18; (2) P=0.215). Remarkably, among the 41 small HCC lesions detected by gadoxetic acid-enhanced MRI, 18 lesions had estimated size <1cm with a mean size of 0.69±0.15cm, whereas no lesion of this size range was detected by dt-PET/CT. Figure 1 shows one of the HCC cases detected by gadoxetic acid-enhanced MRI (Figure 1A, Figure 1B), while the dt-PET/CT scan showed mild focal increased ACT uptake (Figure 1C) without increased FDG uptake (Figure 1D).
Discussion
To the best of our knowledge, this is the first study comparing head-to-head on the diagnostic performance between gadoxetic acid-enhanced MRI and dt-PET/CT for detecting HCC lesions. This study showed that gadoxetic acid-enhanced MRI has higher sensitivity in detecting HCC lesions than using dt-PET/CT, although both imaging modalities have high specificity.Furthermore, the better sensitivity in detecting small HCC lesions and the smaller average size of lesions detected by gadoxetic acid-enhanced MRI compared to those detected by dt-PET/CT, implies that gadoxetic acid-enhanced MRI outperforms dt-PET/CT for detecting smaller HCC lesions. This suggested that gadoxetic acid-enhanced MRI could be more effective in identifying early-stage HCCs.
In addition, gadoxetic acid-enhanced MRI also provides an additional advantage over dt-PET/C, where it requires no radiation involvement. This could be useful for patients who need frequent and/or long-term imaging surveillance for their disease management, which might include patients with risk factors of HCC, such as chronic hepatitis, cirrhosis, etc.
This study was limited in the retrospective nature of the study, which might introduce unavoidable selection bias. The data were also collected from a single center; hence the generalizability of the results would be affected. A further prospective study using multi-center data is warranted.
In conclusion, gadoxetic acid-MRI is more effective in detecting HCC lesions, especially the smaller lesions than dt-PET/CT. Thus, gadoxetic acid-MRI could provide clinical value in the early diagnosis of HCC.
Acknowledgements
No acknowledgement found.References
[1]Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. doi:10.3322/caac.21492. [2] Park JW, Ji HK, Seok KK, Keon WK, Kyung WP, Choi J Il, et al. A prospective evaluation of 18F-FDG and 11C-acetate PET/CT for detection of primary and metastatic hepatocellular carcinoma. J Nucl Med 2008;49:1912–21. doi:10.2967/jnumed.108.055087. [3] Guo J, Seo Y, Ren S, Hong S, Lee D, Kim S, et al. Diagnostic performance of contrast-enhanced multidetector computed tomography and gadoxetic acid disodium-enhanced magnetic resonance imaging in detecting hepatocellular carcinoma: direct comparison and a meta-analysis. Abdom Radiol 2016;41:1960–72. doi:10.1007/s00261-016-0807-7.Figures
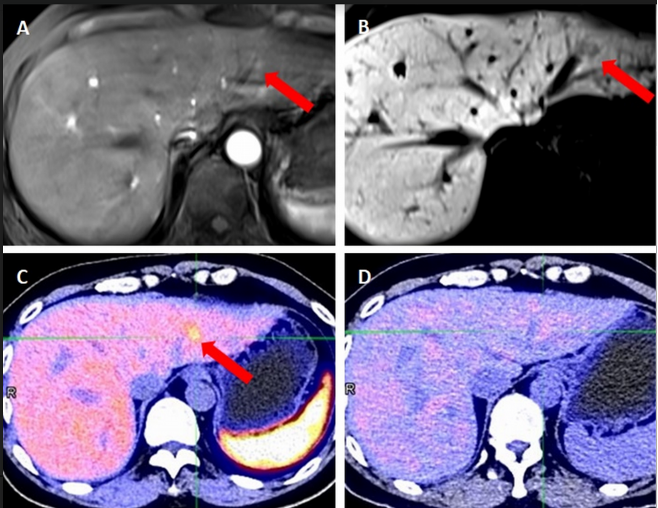
Figure 1 Identification of HCC with gadoxetic acid-enhanced MRI and dt-PET/CT (indicated by red arrow), A) axial arterial phase, B) axial HBP, C) ACT-PET image, and D) FDG-PET image
DOI: https://doi.org/10.58530/2022/4262