4258
The spectrum of MRI-PDFF, MRS, and two different histopathologic methods (AI vs. pathologist) in the quantification of hepatic steatosis1Radiology, Korea University Guro Hospital, Seoul, Korea, Republic of, 2Korea University Guro Hospital, Seoul, Korea, Republic of
Synopsis
The aim of our study was to 1) provide spectrum of values of multi-echo mDixon MRI-PDFF, FFMRS, and FFs measured by two different histopathologic methods (pathologist and automatic fat vacuole segmentation), and 2) to evaluate the correlation among them. The values of MRI-PDFF and FFMRS were significantly higher than FFAI and significantly lower than FFpathologist. Except for one case (97.9%,46/47), FFMRS always showed higher value than MRI-PDFF and the average difference was 2.06 %. MRS and MRI-PDFF showed strong correlation with each other and with each histopathologic method. MRI-PDFF or MRS could be used as an alternative non-invasive reference standard.
Purpose
In non-alcoholic fatty liver disease (NAFLD), the grade of hepatic steatosis is evaluated semi-quantitatively, in which the fraction of macrovesicular fat-containing hepatocytes is measured and then graded as a discrete value (S0-3)1. However, the proton density fat fraction (PDFF) measured by MR imaging (MRI) and FF measured by MR spectroscopy (FFMRS) is a continuous value. Therefore, a quantitative method using automatic fat vacuole segmentation may be needed. MRS is generally considered the method of choice for accurate non-invasive quantification of hepatic fat2. Several quantitative MRI techniques including Dixon methods have also provided accurate quantification of hepatic fat3. The aim of our study was to 1) provide spectrum of values of MRI-PDFF, FFMRS, and FFs measured by two different histopathologic methods, 2) to evaluate the correlation among them, and 3) to evaluate the diagnostic performance of MRI-PDFF and MRS for grading hepatic steatosis.Materials and Methods
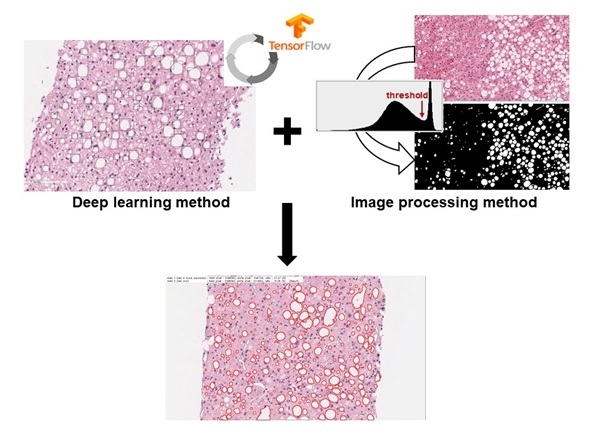
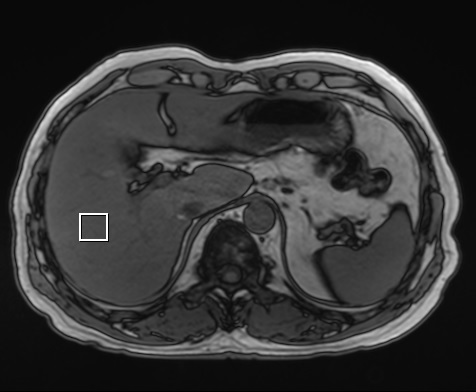
This retrospective study was approved by our institutional review board and the requirement for informed consent was waived. Forty-seven patients who underwent liver biopsy for the evaluation of NAFLD were included from October 2016 to June 2017. All patients also underwent MRI-PDFF and MRS.Hepatic steatosis was assessed histopathologically by using two different methods. First, the fraction of macrovesicular fat-containing hepatocytes was determined by an experienced pathologist’s visual estimation (FFpathologist). Steatosis grade was assigned as S0 (<5%), S1 (5-33%), S2 (34-66%), and S3 (>67%)1. Second, the FF was calculated by automatic fat vacuole segmentation using a deep learning method (FFAI). Entire microscope slides of the liver biopsy were scanned, and at 200× magnification, five randomly selected images were obtained from each slide. Two methods were used to determine the fat areas: 1) a deep learning method using TensorFlow, version 1.3.0 (Google, Mountain View, CA, USA), and 2) an image processing method (Figure 1). The percentage of fat fraction correspond to the area of the fat divided by the total tissue area. MR imaging was performed with a 3 T MR scanner (MAGNETOM Skyra, Siemens Healthineers, Erlangen, Germany). Single-voxel MRS was performed using a prototypical high-speed T2-corrected multi-echo (HISTO) technique4. A single voxel (20×20×20 mm) was placed in the right hepatic posterior segment (Figure 2). Parameters included repetition time (TR), 3000 msec; mixing time, 10 msec; and 5 echo times (TEs) of 12, 24, 36, 48, and 72 msec. Each MRS acquisition was performed within 15 seconds during one breath hold. This process was repeated three times, and the mean value was used.
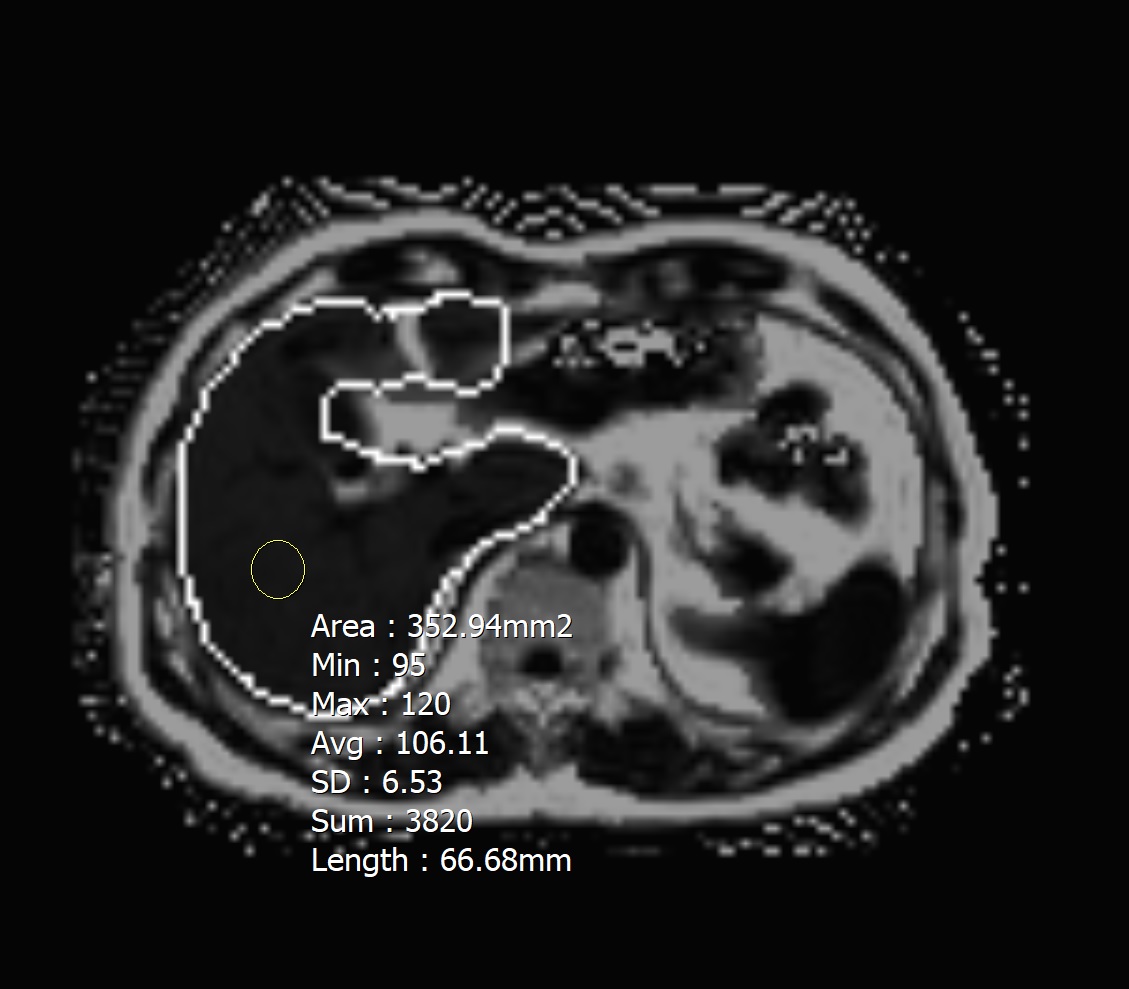
Axial multi-echo (six-echo) modified Dixon gradient echo sequence was also acquired for the measurement of hepatic PDFF for 13 seconds breath hold. Parameters included flip angle, 4˚; TR, 9.0 msec; and 6 TEs of 1.23, 2.46, 3.69, 4.92, 6.15, and 7.38 msec. A circular ROI was drawn in the right hepatic posterior segment at the same location as in the MRS (Figure 3). Three ROIs were measured, and the mean value was used.
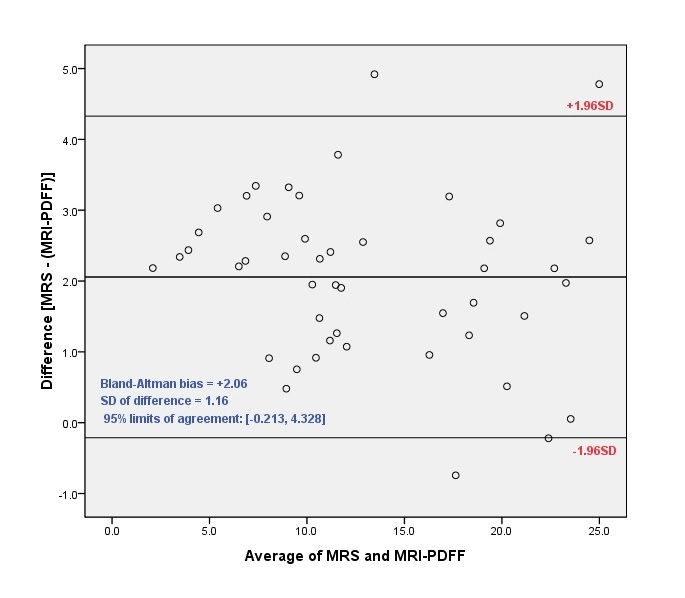
The mean FF values were presented as mean ± standard deviation (SD). Correlations between MRI-PDFF and MRS, between two different histopathologic methods, and between MRI-PDFF/MRS and each histopathologic method were assessed using Pearson correlation tests. The agreement between MRI-PDFF and MRS was assessed by Bland-Altman analysis and the 95% limit of agreement (LOA) was calculated. The diagnostic performance of MRI-PDFF and MRS were assessed using receiver operating characteristic (ROC) curve analyses and the areas under the curve (AUCs) were obtained.
Results
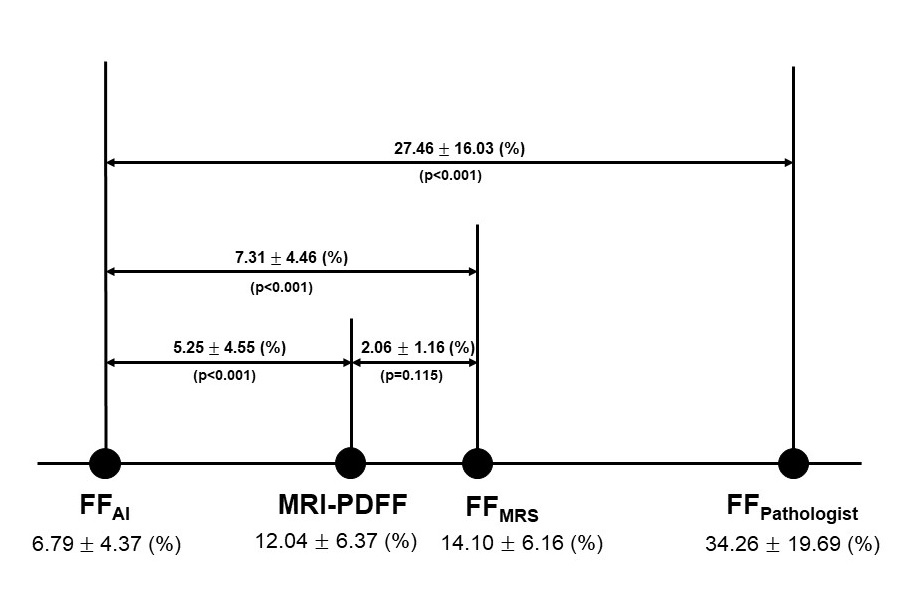
Forty-seven patients (16 men, 31 women; mean age 51.3±12.6 years; range 19-75 years) were included. The means±SD of MRI-PDFF, FFMRS, FFpathologist, and FFAI were 12.04±6.37, 14.01±6.16, 34.26±19.69, and 6.79±4.37 (%), respectively (Figure 4). Bland-Altman bias (the mean of the MRI-PDFF MRS differences) was 2.06 % (95% LOA, -0.213%, 4.328%) (Figure 5). MRI-PDFF and MRS showed very strong correlation (r = 0.983, p <0.001). Two different histopathologic methods also showed very strong correlation (r = 0.872, p <0.001). For the FFpathologist, both MRI-PDFF and MRS demonstrated strong correlation (r = 0.701, p <0.001 and r = 0.709, p <0.001, respectively). For the FFAI, both MRI-PDFF and MRS also demonstrated strong correlation (r = 0.700, p <0.001 and r = 0.690, p <0.001, respectively). The AUCs of MRI-PDFF for grading ≥S2 and ≥S3 were 0.846 and 0.855, respectively. The AUCs of MRS for grading ≥S2 and ≥S3 were 0.860 and 0.878, respectively.Discussion
The values of MRI-PDFF and FFMRS were significantly higher than FFAI and significantly lower than FFpathologist. These results are thought to be due to different histopathological methods; FFpathologist corresponds to the proportion of hepatocytes including macrovesicular fat1 and FFAI corresponds to the area of macrovesicular fat in the entire area. Except for one case (97.9%, 46/47), FFMRS always showed higher value than MRI-PDFF and the average difference was 2.06 %. MRS and MRI-PDFF also showed strong correlation with each other and with each histopathologic method.Conclusion
Although it is difficult to measure the amount of “real” hepatic fat, the results of our study demonstrated that MRI-PDFF or MRS can be used as an alternative non-invasive reference standard. However, there is a certain difference between two modalities, so care should be taken in their use.Acknowledgements
Young-Sun Lee (Department of internal medicine) and Baek-Hui Kim (Department of pathology) contributed to collect clinical and pathologic data.
Mun Young Paek (Siemens Healthineers Limited, Seoul, Korea) contributed to design of MRI sequence and protocols.
Jong Man Kim contributed to calculate the fat fraction by automatic fat vacuole segmentation using deep learning and image processing method.
References
1. Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313-21.
2. d'Assignies G, Ruel M, Khiat A, Lepanto L, Chagnon M, Kauffmann C, et al. Noninvasive quantitation of human liver steatosis using magnetic resonance and bioassay methods. Eur Radiol. 2009;19(8):2033-40.
3. Kukuk GM, Hittatiya K, Sprinkart AM, Eggers H, Gieseke J, Block W, et al. Comparison between modified Dixon MRI techniques, MR spectroscopic relaxometry, and different histologic quantification methods in the assessment of hepatic steatosis. Eur Radiol. 2015;25(10):2869-79.
4. Pineda N, Sharma P, Xu Q, Hu X, Vos M, Martin DR. Measurement of hepatic lipid: high-speed T2-corrected multiecho acquisition at 1H MR spectroscopy--a rapid and accurate technique. Radiology. 2009;252(2):568-76.
Figures