4247
The feasibility of ZTE MR lung imaging in the assessment of pulmonary nodules or masses: a prospective head-to-head comparison with CT1Medical Imaging, Yueyang Central Hospital, Medical Imaging, Yueyang Central Hospital, Yueyang, Hunan, China, China, 2Department of Radiology, The Third Xiangya Hospital, Central South University, Changsha, Hunan, China, Department of Radiology, The Third Xiangya Hospital, Central South University, Changsha, Hunan, China, Changsha, Hunan, China, China, 3GE Healthcare, MR Research China, Beijing, Beijing, China, China
Synopsis
The feasibility of zero echo time MR lung imaging in the assessment of pulmonary nodules or masses: a prospective head-to-head comparison with CT.
Introduction
Pulmonary nodules or masses are commonly detected by chest CT in routine clinical practice. Most patients with pulmonary nodules need regular imaging surveillance for individual treatment decisions and care management. Patients with lung malignancies frequently received follow-up imaging for the evaluation of clinical response and disease recurrence. Lung MRI is desirably utilized for frequent follow-up imaging examinations with the feature of non-ionizing radiation. However, conventional MR imaging was hindered by the intrinsic physical properties of the lung (e.g. air and scarce proton signals). Zero echo time magnetic resonance imaging (ZTE-MRI) is a newly introduced gradient echo-based MRI sequence with a minimum susceptibility effect that can overcome the abovementioned challenges [1-3] and offer better signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR). However, the performance of lung ZTE-MRI on the detecting pulmonary nodules or masses in comparison with conventional CT in routine practice is still not fully illustrated.Material and Methods
This prospective study was approved by our Institutional Review Board . 71 patients were confirmed for the existence of solid pulmonary nodules or masses by CT images and were enrolled and underwent lung ZTE-MRI scans within 3 days. ZTE-MRI and CT images were compared in terms of subjective image quality and imaging features. Unidimensional diameter and 3-dimensional volume of nodules or masses on both methods were manually measured and compared through statistical analysis.Results
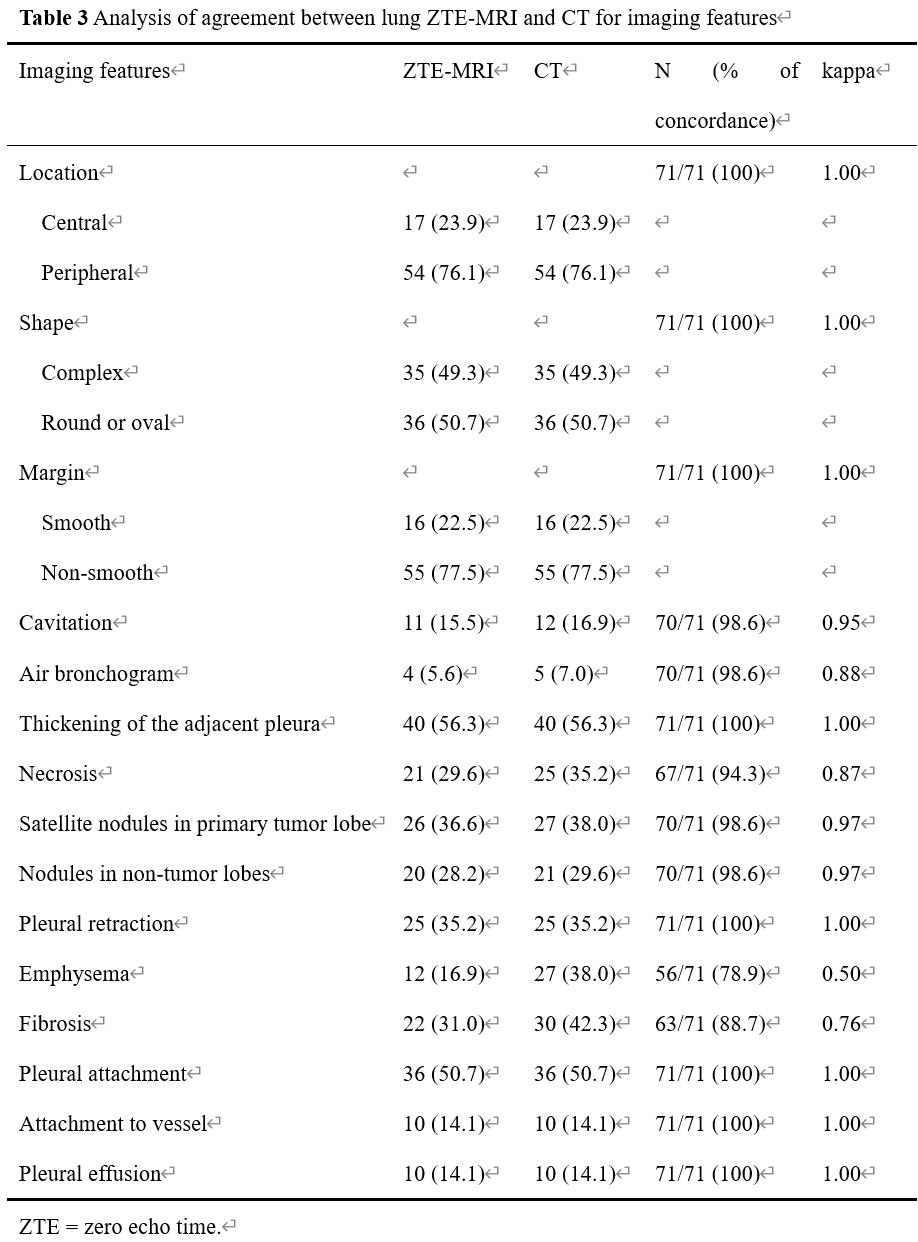
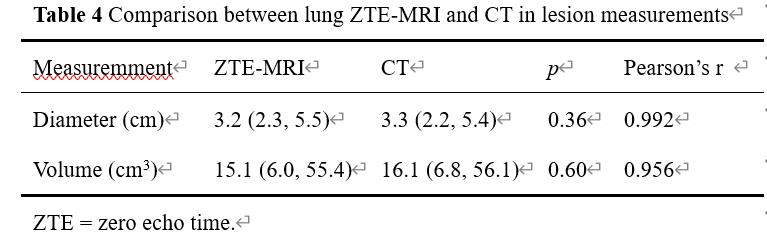
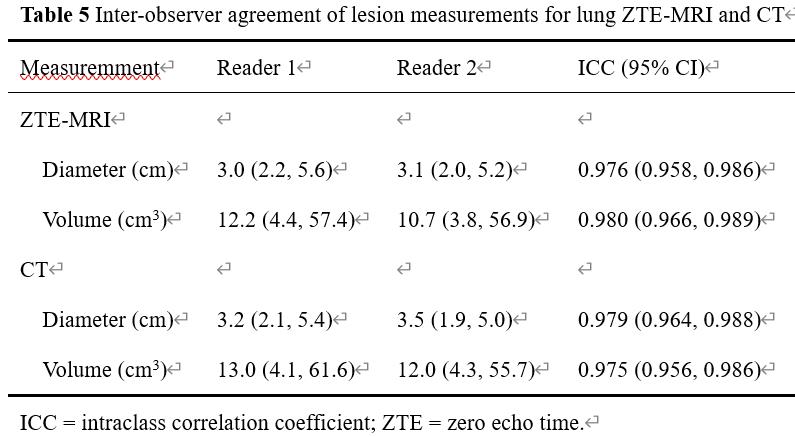
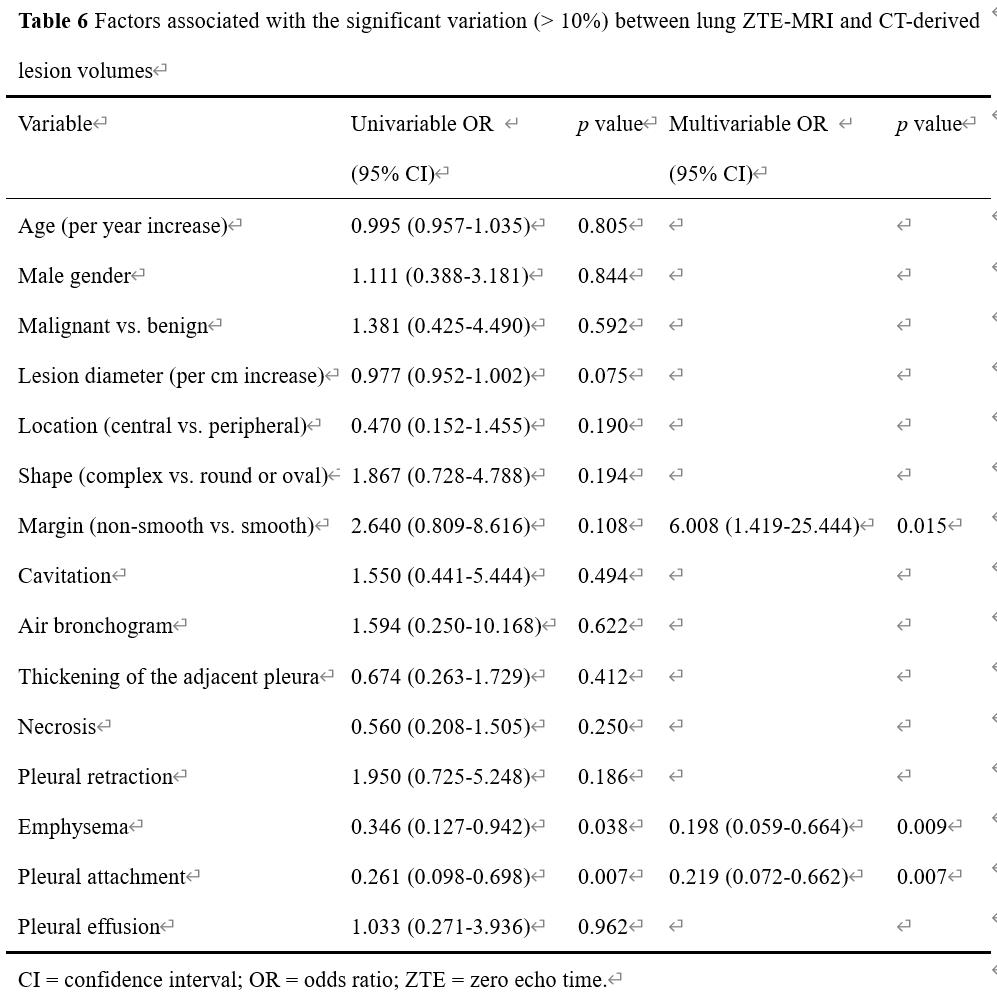
54/71 (76.1%) patients were diagnosed with lung cancer. Subjective image quality was superior in CT compared with ZTE-MRI (p < 0.001). Inter-modality agreement for the imaging features was moderate for emphysema (Kappa = 0.50), substantial for fibrosis (Kappa = 0.76), and excellent (kappa = 0.87-1.00) for all the other features. The diameter and volume between ZTE-MRI and CT showed no significant difference (both p > 0.05) and revealed nearly excellent inter-observer agreement (intraclass correlation coefficient [ICC] = 0.975~0.980, p = 0.36 for diameter and p = 0.60 for volume). Multivariable analysis showed that non-smooth margin (odds ratio [OR] = 6.008, p = 0.015) was an independent predictor for significant inter-modality variation of volume between ZTE-MRI and CT.Discussion and Conclusion
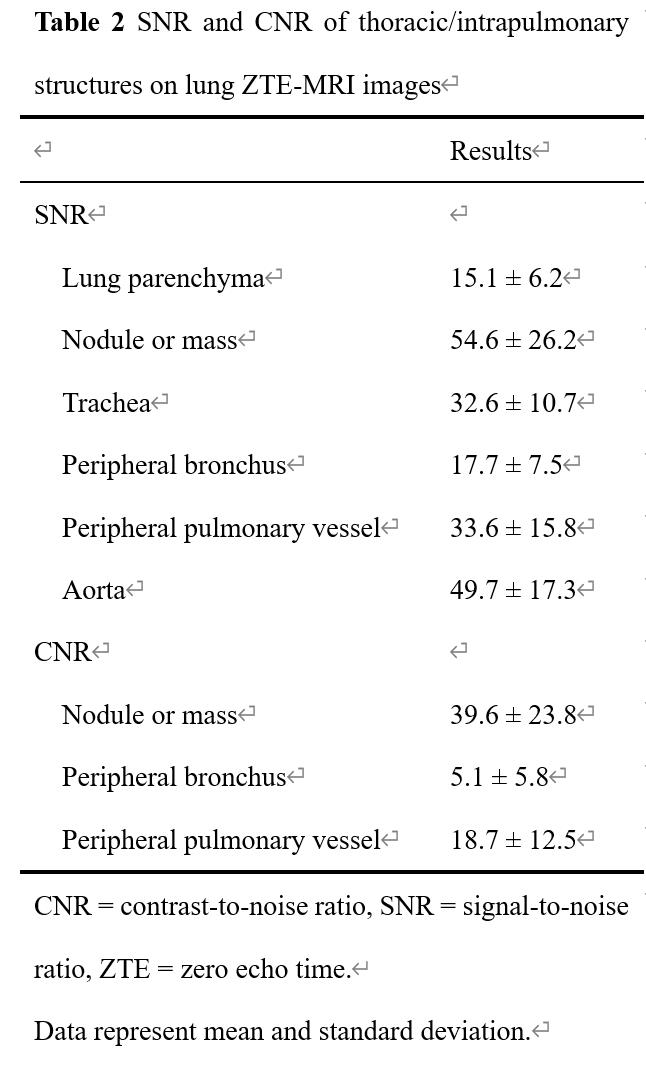
ZTE imaging is a 3D slab excitated fast spin echo-based sequence with k space of center-out filling technique [5, 6]. SNR and CNR of intrapulmonary structures to nodule or mass on ZTE-MR images were consistent with one previous report [4]. In our study, ZTE-MRI images were acquired in a quiet and free-breath mode. Long-time scanning may induce respiratory motion artifacts in some patients, especially for those with severe emphysema or poor lung function. Notably, the lesion-pleura interface margin can be more clearly depicted by ZTE-MRI. MRI offers superior contrast between pleura and adjacent tissues compared to CT. Our results indicated that ZTE-MRI sequence may be served as an important approach for the assessment of pleural invasion of pulmonary lesions. The clinical utility of ZTE-MRI for the detection of pleural invasion in patients with lung malignancies is deserved being verified. The lesion size varying with time during the follow-up period is the cornerstone for treatment response of lung tumor in the conventional Response Evaluation Criteria in Solid Tumors (RECIST). Furthermore, volumetric measurement may provide more complete information of treatment response and predicting survival rate of lung cancer patients particularly with large, irregular lesions, thus allowing for faster assessment of new treatments. Tsim et al reported that MRI volumetry gained superiority and potential over CT for malignant pleural mesothelioma in terms of the association with patient survival [7]. High-resolution ZTE-MRI should be useful for the size evaluation including diameter and volume measurements of pulmonary nodules or masses, which has the potential to obviate frequent chest CT scans, especially in patients who are vulnerable to radiation exposure. Besides, the possible factors for significant inter-modality variations of lesion volume between ZTE-MRI and CT was non-smooth margin, an independent predictor. This may be explained by the significant differences of image display between the peripheral part of the irregular lesions and the adjacent lung tissue on the two imaging modalities. Several limitations including relatively small sample size,only solid pulmonary nodules or masses.ZTE lung imaging is feasible as a part of routine chest MRI in the assessment and surveillance of pulmonary nodules or masses, presenting perfect agreement with CT in terms of imaging features and size measurement.Acknowledgements
No acknowledgement found.References
1.Gibiino F, Sacolick L, Menini A, Landini L, Wiesinger F (2015) Free-breathing, zero-TE MR lung imaging. Magma 28:207-215.
2.Breighner RE, Endo Y, Konin GP, Gulotta LV, Koff MF, Potter HG (2018) Technical Developments: Zero Echo Time Imaging of the Shoulder: Enhanced Osseous Detail by Using MR Imaging. Radiology 286:960-966.
3.Weiger M, Pruessmann KP (2019) Short-T(2) MRI: Principles and recent advances. Prog Nucl Magn Reson Spectrosc 114-115:237-270.
4.Bae K, Jeon KN, Hwang MJ et al (2020) Respiratory motion-resolved fourdimensional zero echo time (4D ZTE) lung MRI using retrospective soft gating: feasibility and image quality compared with 3D ZTE. Eur Radiol 30:5130-5138.
5.Weiger M, Brunner DO, Dietrich BE, Müller CF, Pruessmann KP (2013) ZTE imaging in humans. Magn Reson Med 70:328-332.
6. Zhang C, Dou W, Yu K et al (2021) The feasibility of non-contrast-enhanced zero echo time magnetic resonance angiography for characterization of intracranial atherosclerotic disease. Quantitative Imaging in Medicine and Surgery 11:2442-2452.
7. Tsim S, Cowell GW, Kidd A et al (2020) A comparison between MRI and CT in the assessment of primary tumour volume in mesothelioma. LUNG CANCER 150:12-20.
Figures
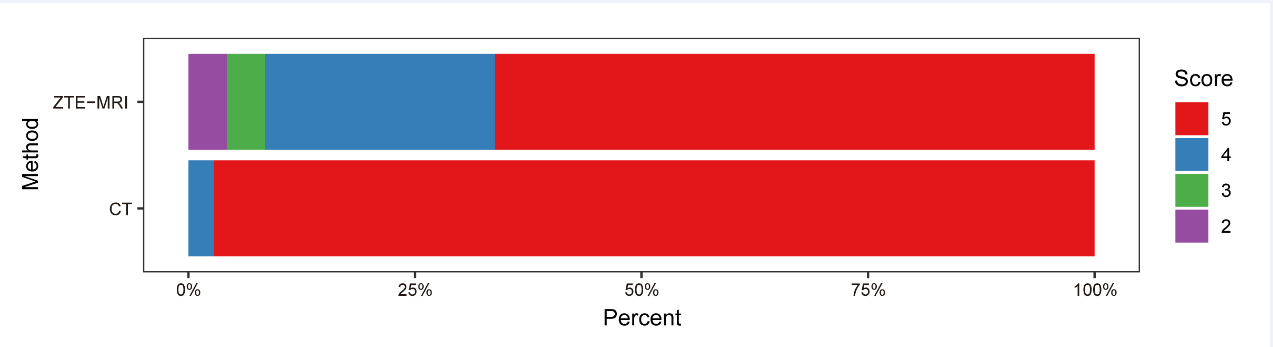
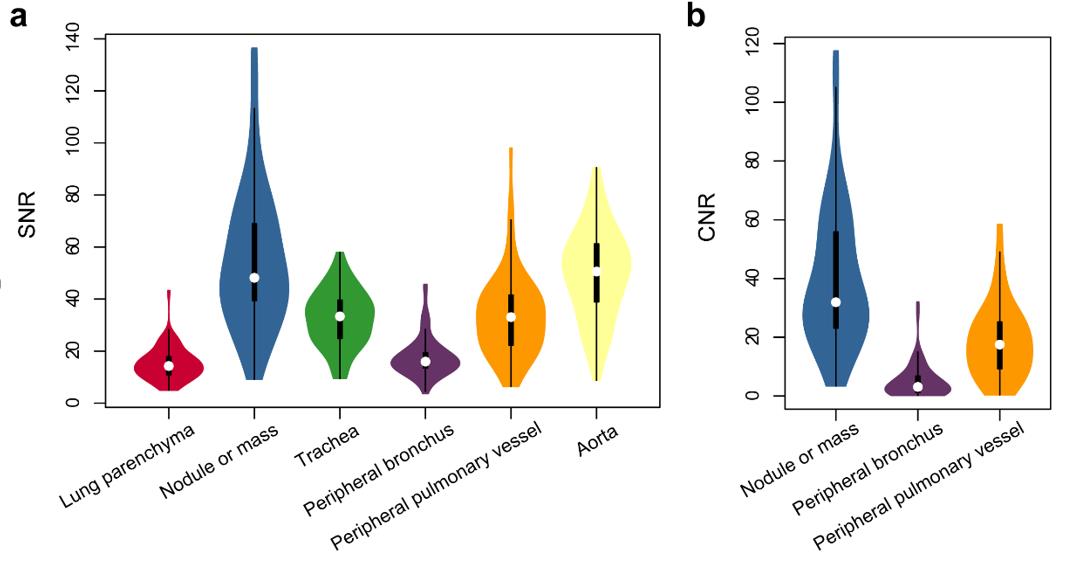
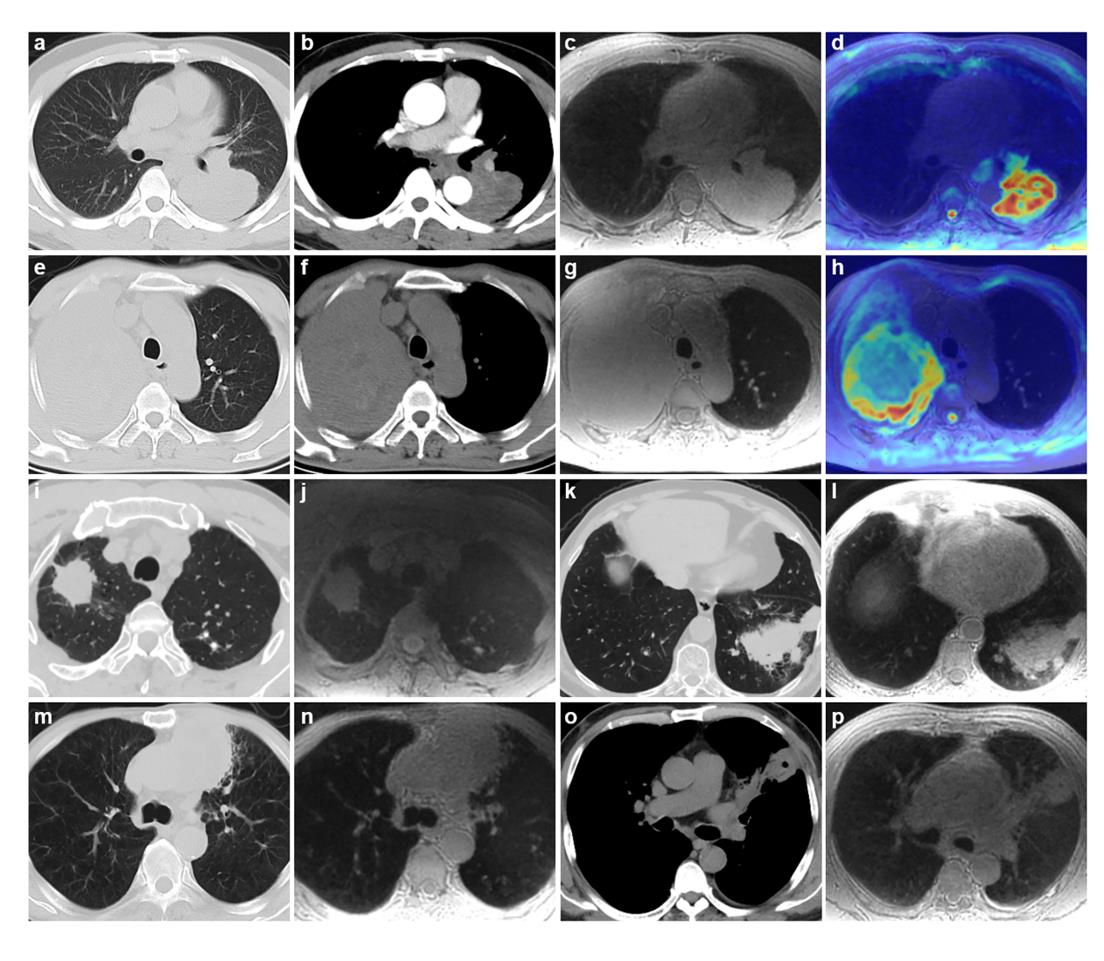
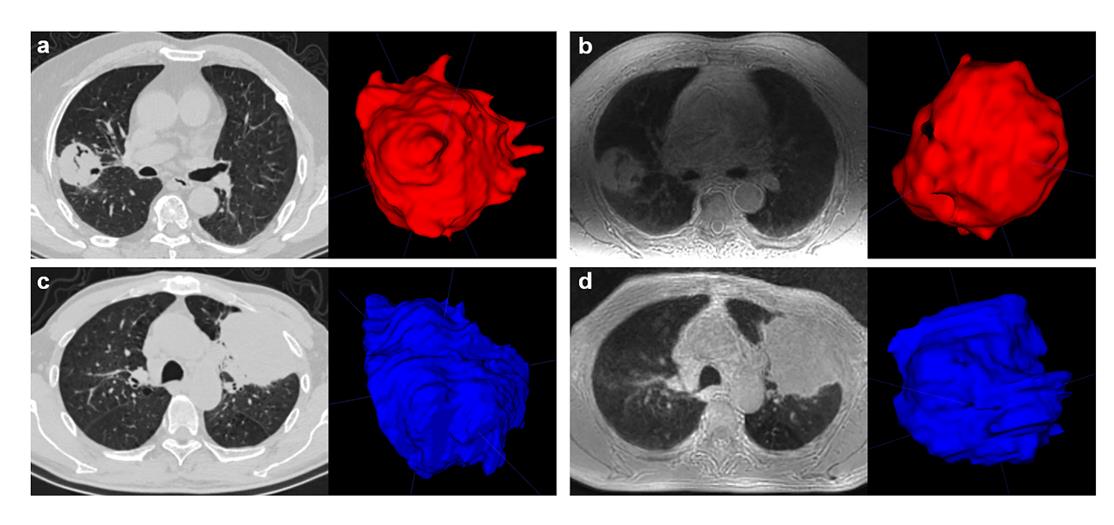
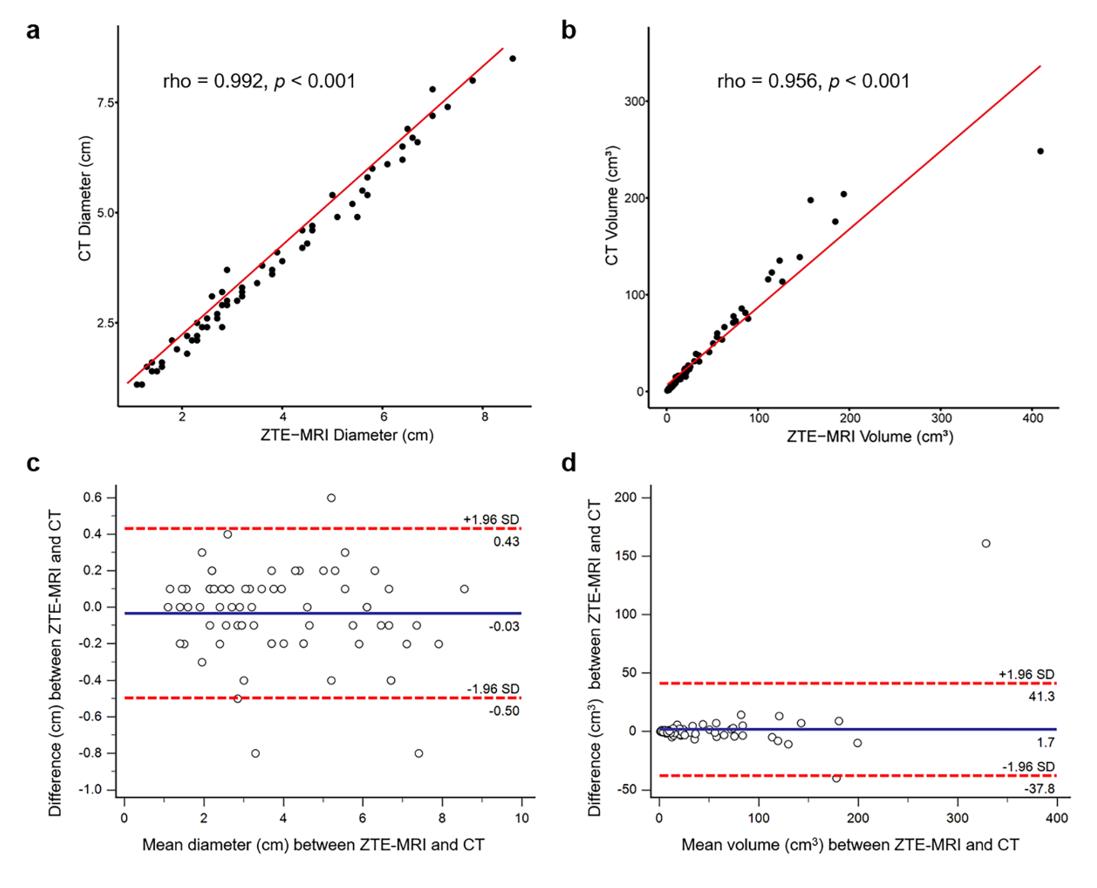
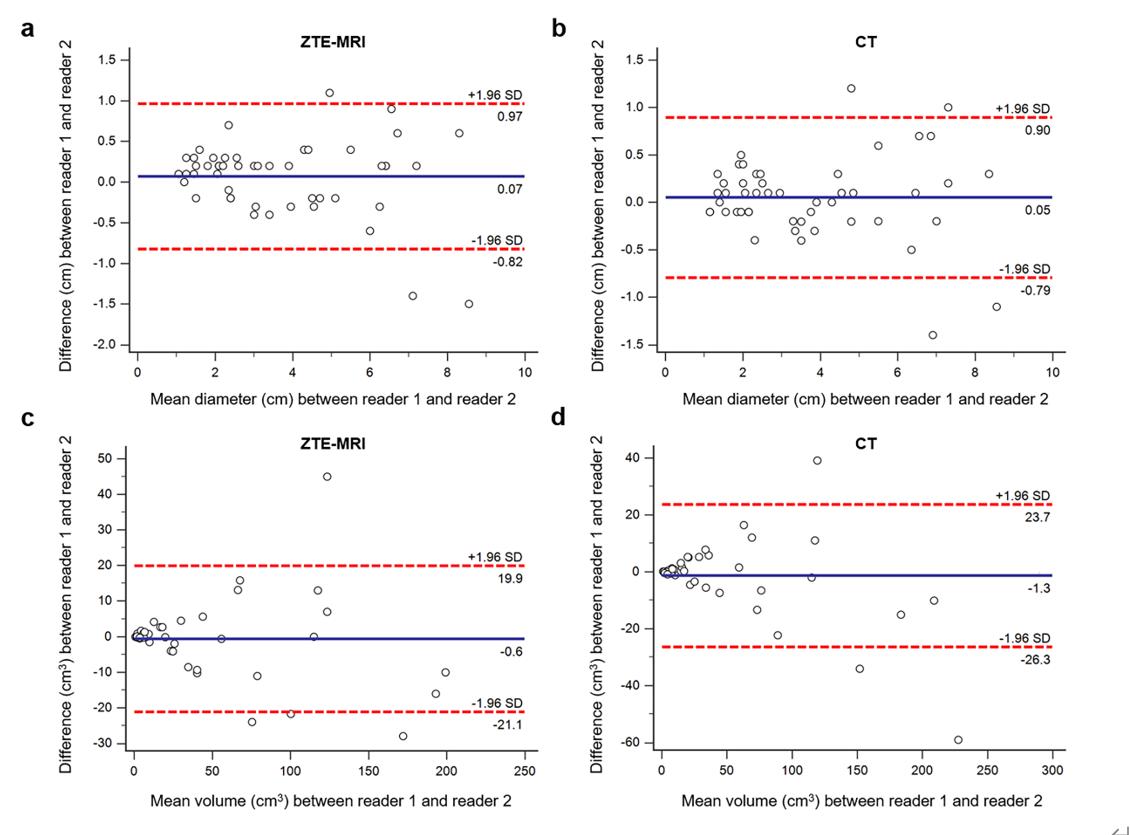
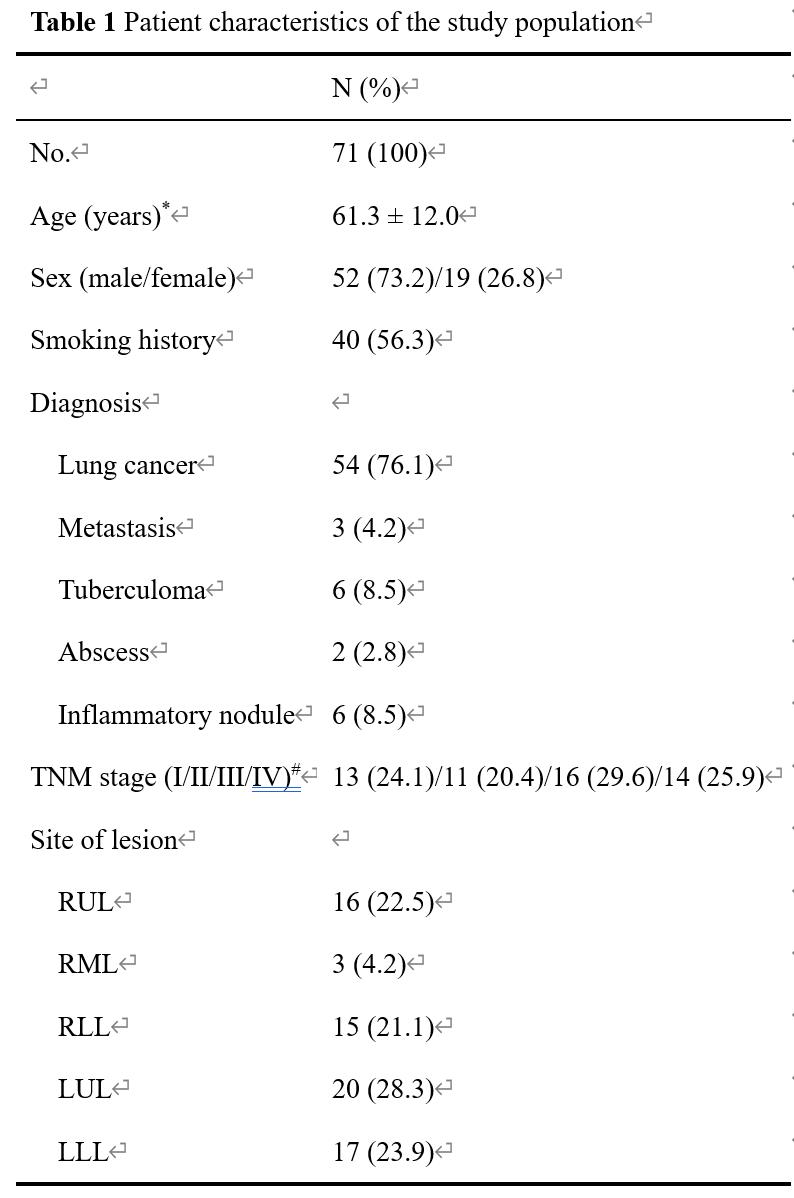
Table 1 Patient characteristics of the study population