4233
Dynamic contrast-enhanced magnetic resonance imaging of endometrial cancer with/without squamous differentiation
Mayumi Takeuchi1, Kenji Matsuzaki2, Yoshimi Bando3, and Masafumi Harada1
1Department of Radiology, Tokushima University, Tokushima, Japan, 2Department of Radiological Technology, Tokushima Bunri University, Sanuki-city, Japan, 3Division of Pathology, Tokushima University Hospital, Tokushima, Japan
1Department of Radiology, Tokushima University, Tokushima, Japan, 2Department of Radiological Technology, Tokushima Bunri University, Sanuki-city, Japan, 3Division of Pathology, Tokushima University Hospital, Tokushima, Japan
Synopsis
DCE-MRI of endometrial cancer including 41 low-grade type I cancers without squamous differentiation (LG) and 39 with squamous differentiation (LG_w/SD), and 20 high-grade type II cancers (HG) was retrospectively evaluated. Significant difference in the time-intensity curves was found between LG and HG, and LG and LG_w/SD, whereas no significant difference was seen between HG and LG_w/SD. Curve type 3 (initial signal rise which is steeper than that of the myometrium) was more frequent in HG (60%) and LG_w/SD (77%) than in LG (34%). It should be recognized as a pitfall that HG and LG_w/SD may show similar early strong enhancement.
Introduction
Endometrial cancer is the most common gynecological malignancy and its prognosis depends on various factors such as histological subtype and grade, tumor stage including depth of myometrial invasion, and nodal status 1. Endometrial cancers are divided into estrogen-dependent type I (G1-2 endometrioid carcinomas) and clinically aggressive estrogen-independent type II (G3 endometrioid, serous, and clear cell carcinomas) 2. Because type II cancer have a high risk for nodal metastases and combined pelvic and para-aortic lymphadenectomy result in improved survival in patients, preoperative prediction of subtypes is important in planning the surgical procedure 3. Fukunaga et al. reported that endometrial cancer with strong enhancement on DCE-MRI is suggestive of type II cancer 3. However, type I cancer may also sometimes show strong enhancement. Misdiagnosis of low-grade endometrial cancer as high-grade cancer may affect the treatment strategy. We hypothesized that endometrioid carcinoma with squamous differentiation would be strongly enhanced in the early phase, because squamous cell carcinoma of the uterine cervix shows early strong enhancement 4.The purpose of this study is to compare the DCE-MRI findings of endometrial cancers with and without squamous differentiation to test the hypothesis.Methods
We retrospectively analyzed preoperative MRI studies of 39 patients (31-80 years, mean 57) with low-grade (25 G1 and 14 G2) endometrioid carcinoma with squamous differentiation (LG w/ SD), 41 patients (39-84 years, mean 59) with low-grade (29 G1 and 12 G2) endometrioid carcinoma without squamous differentiation (LG), and 20 patients (49-84 years, mean 65) with high-grade endometrial cancers (HG) including 10 G3 endometrioid carcinomas, 5 serous carcinomas, and 5 clear cell carcinomas. 3D DCE-MR imaging of the pelvis was performed after administration of a gadolinium chelate (0.1 mmol/kg at 2 mL/s), which was flushed with 20 mL saline, by using a 3D gradient recalled echo T1-weighted liver acquisition volume acceleration sequence (LAVA) by using 3T MRI unit (Discovery MR750, GE). Images were acquired at multiple phases of contrast medium enhancement in sagittal plane (pre-contrast and post-contrast at 25 or 30, 50, 70, 90 and 110 seconds). Semiquantitative analysis of DCE-MR images was performed with the region-of-interest (ROI) technique. ROIs were placed within normal outer myometrium as the internal reference and within the most enhanced portion in endometrial mass in the early phase (< 60 sec.) 5, 6. The time-intensity curve was made by using Functool Software on the workstation (AW2.0, GE healthcare). A gradual increase in the signal without a well defined shoulder (curve type 1), a moderate initial rise in the signal relative to that of the myometrium (curve type 2) and an initial rise in the signal that was steeper than that of the myometrium (curve type 3) were visually evaluated 5, 6. Curve type 3 is subdivided into type 3A (signal rise is reversed at the second phase) and 3B (signal rise is still steeper at the second phase).Results
Time-intensity curve (TIC) patterns of the endometrial cancers are summarized in Table 1 (Fig. 1), according to their histology. Significant difference in the TICs were found between LG (Fig. 2) and HG (Fig. 3) (p < 0.05), and LG and LG w/ SD (Fig. 4) (p < 0.0005). No significant difference in the TICs was found between HG and LG w/ SD. Curve type 1 appeared specific for low-grade cancers (LG and LG w/ SD) but relatively rare (15% and 5%, respectively) (Fig. 5), and was never observed in HG. Curve type 3 was more frequent in HG (60%) and LG w/ SD (77%) than in LG (34%). Especially, there was a difference in the frequency of type 3B between the former two types (HG and LG w/ SD, 35% and 51%, respectively), and LG (15%).Discussions
DCE-MRI is a well-established method for evaluating tumor angiogenesis. Thomassin-Naggara et al. reported that the early enhancement patterns of ovarian epithelial tumors are associated with tumor angiogenic factors 5, 6. Fukunaga et al. showed that strong enhancement of type II endometrial cancers reflecting these angiogenic factors, and that DCE-MRI is useful for the differentiation between the two types of endometrial cancers 3. In our study, there is a significant difference in the TICs between LG and HG, which is consistent with the results of Fukunaga et al. However, LG w/ SD and HG tends to show similar early enhancement patterns. Especially, 51% of LG w/ SD showed type 3B TIC, which means strong enhancement in the early phase (< 60 sec.) of DCE-MRI 5, 6 compared with the myometrium. Squamous differentiation is present in about 10–25% of endometrioid carcinomas, and is not associated with different prognosis 1. Thus, low-grade type I cancer with squamous differentiation should not be misdiagnosed as high-grade type II cancer for the adequate therapeutic planning. In order to differentiate between Type I cancers with squamous differentiation and Type II cancers, careful diagnosis should be made based on findings other than DCE-MRI, such as patient’s age, invasive tendency, and diffusion restriction 7.Conclusion
Based on the DCE-MRI enhancement pattern, type I cancer with squamous differentiation and type II cancer may show similar strong enhancement in the early phase, and it should be recognized as a pitfall.Acknowledgements
No acknowledgement found.References
- Bosse T, et al. Endometrioid carcinoma of the uterine corpus. In: WHO Classification of Tumours Editorial Board. WHO Classification of Tumours, 5th ed., Vol.4 Female Genital Tumours. pp. 252-55, WORLD HEALTH ORGANIZATION, 2020.
- Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol 15:10-7, 1983.
- Fukunaga T, et al. Accuracy of semiquantitative dynamic contrast-enhanced MRI for differentiating type II from type I endometrial carcinoma. J Magn Reson Imaging 41:1662-8, 2015.
- Yamashita Y, et al. Carcinoma of the cervix: dynamic MR imaging. Radiology. 182:643-8, 1992.
- Thomassin-Naggara I, et al. Epithelial ovarian tumors: value of dynamic contrast-enhanced MR imaging and correlation with tumor angiogenesis. Radiology 248:148-59, 2008.
- Thomassin-Naggara I, et al. Dynamic contrast-enhanced magnetic resonance imaging: a useful tool for characterizing ovarian epithelial tumors. J Magn Reson Imaging 28:111-20, 2008.
- Chen J, et al. The value of the apparent diffusion coefficient in differentiating type II from type I endometrial carcinoma. Acta Radiol 62:959-65, 2021.
Figures
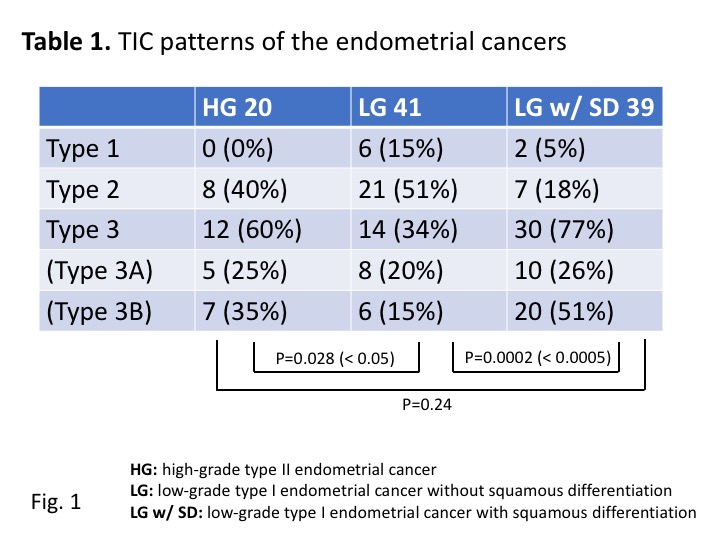
Table 1: TIC patterns of the endometrial cancers
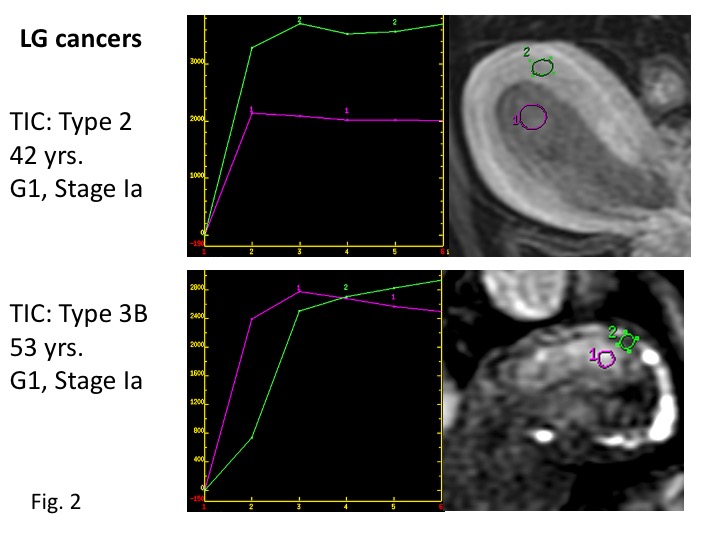
Low-grade Type I endometrial cancers without squamous differentiation (LG) Upper: LG cancer exhibiting type 2 TIC (common). Lower: LG cancer exhibiting type 3B TIC (rare). Histopathological examination revealed prominent inflammatory cell infiltration, which may cause the early strong enhancement.
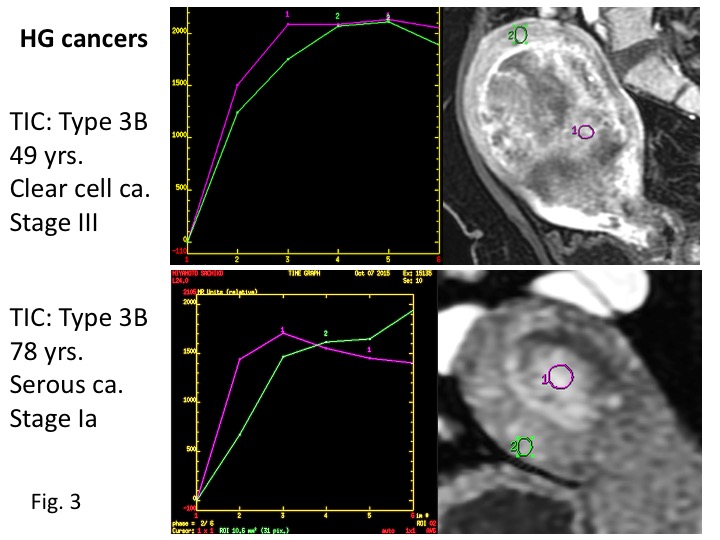
High-grade type II endometrial cancers (HG) Upper: Large HG cancer exhibiting type 3B TIC. Heterogeneous enhancement containing strong enhanced areas in the early phase is observed. Lower: HG cancer exhibiting type 3B TIC. Early strong enhancement of the tumor is observed.
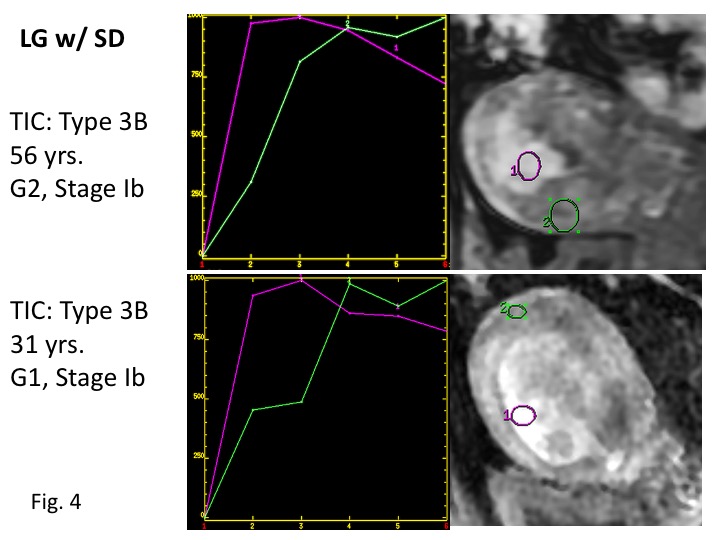
Low-grade Type I endometrial cancers with squamous differentiation (LG w/ SD) Upper/Lower: LG cancers with squamous differentiation exhibiting type 3B TIC. Early strong enhancement of the tumors is observed.
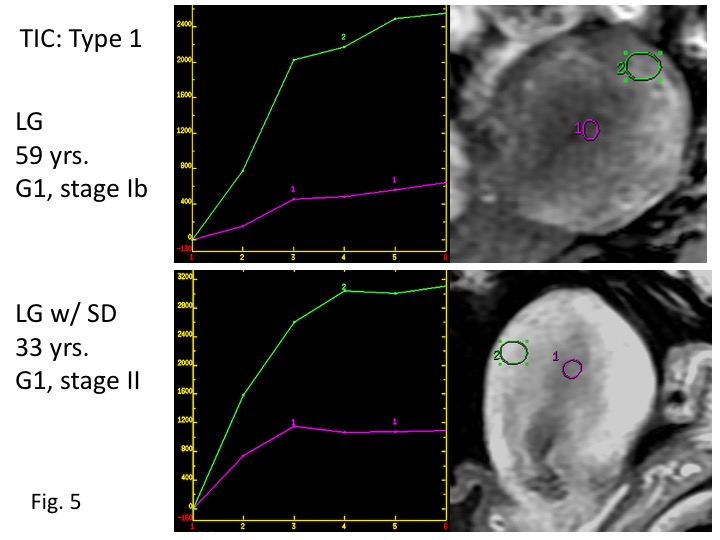
TIC Type 1: Upper: LG cancer exhibiting type 1 TIC .Lower: LG cancer with squamous differentiation exhibiting type 1 TIC.
DOI: https://doi.org/10.58530/2022/4233