4222
Differentiation between hepatocellular carcinoma (HCC) and hepatic metastasis (HM) by mDIXON quant and IVIM imaging1Department of Radiology, the First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Philips Healthcare, Beijing, China
Synopsis
Hepatocellular carcinoma (HCC) and hepatic metastasis (HM) are associated with distinct treatment and prognosis, while the differential diagnosis of HCC and HM still remains challenging. This study aims to explore the value of mDIXON quant and IVIM imaging in the differential diagnosis of HCC and HM. Results shown that the combination of R2*and IVIM measurements may offer a good biomarker for differential diagnosis of HCC and HM.
Introduction
HCC is a fatal malignant tumor [1]. Besides, liver is one of most commonly organs to which various primary malignant tumor metastasized [2,3]. Given that HCC and HM are associated with distinct treatment and prognosis. It is critical to differentiate these two types of lesions. The mDIXON quant imaging is a highly reproducible imaging technique for accurate fat quantification and R2* measurement [4]. IVIM, based on diffusion-weighted imaging, was reported to be valuable for evaluation of the focal liver lesions [5]. The purpose of this study was to explore the value of combination of mDIXON quant and IVIM imaging in the differential diagnosis of HCC and HM.Methods
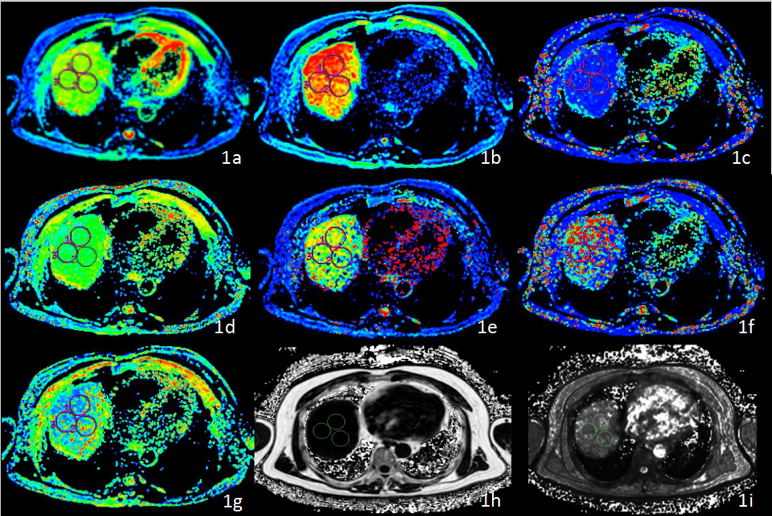
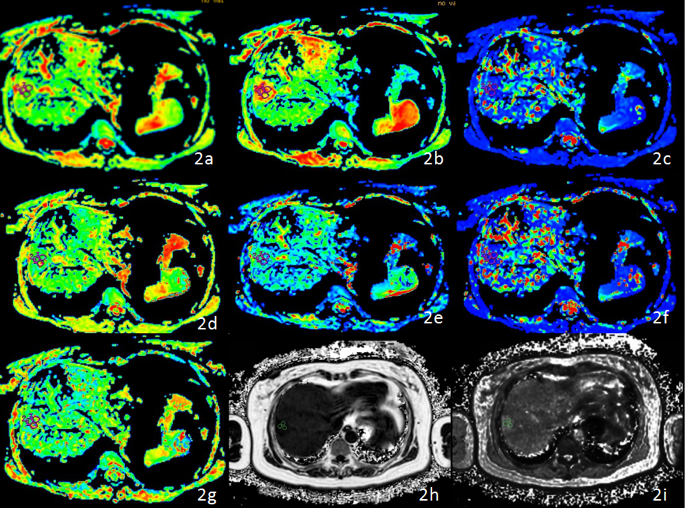
This study has been approved by the local IRB. 57 patients with 73 lesions (HCC or HM) were recruited in this study including 35 HCC patients with 35 lesions (30 men; mean age, 61 years; range, 31–81 years) and 22 HM patients with 38 lesions (24 men; mean age, 61 years; range, 48–89 years) with clinical symptom and image preliminary diagnosis. All patients were scanned using a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, the Netherlands) with a 16-channel abdominal coil. The detail scan parameters were shown in Table 1. The mDIXON quant and IVIM raw data were transferred to the Intellispace Portal workstation (Philips Healthcare) and the GE AW 4.6 workstation (GE Healthcare) respectively for post-processing. Referring to the lesion information obtained on T2w images, the radiologist manually placed the ROIs (100 - 200 mm2) on the axial slice with largest lesion visualization on the fat fraction (FF) and R2* maps by mDIXON Quant, and standard ADC mapping, slow ADC mapping using Mono-exponential fitting (slow ADC Mono), fast ADC mapping using Mono-exponential fitting (fast ADC Mono), fraction of fast ADC mapping using Mono-exponential fitting (fraction of fast ADC Mono), slow ADC mapping bi-exponential (Slow ADC_Bi), fast ADC mapping using bi-exponential fitting (fast ADC_Bi), fraction of fast ADC mapping using bi-exponential fitting by IVIM (fraction of fast ADC_Bi) (Figures 1 and 2). The measured mDIXON Quant and IVIM parameters were compared between the HCC and HM groups using Mann-Whitney U test except fraction of fast ADC Mono and fraction of fast ADC Bi by IVIM, which were compared by using t test. ROC curve was used to analyze the diagnosis performances for parameters that were significantly different between HCC and HM groups, and logistic regression was used to calculate the combined values of mDIXON Quant and IVIM parameters (with significantly different parameters) in the diagnosis of HCC and HM. The AUC values were compared using the Delong test. A p value < 0.05 was considered to be statistically significant.Results
Parameters measured by mDIXON Quant and IVIM in HCC and HM were shown in Table 2. R2*, standard ADC, fast ADC_Mono, fast ADC_Bi, and fraction of fast ADC_ Bi showed significant difference between groups, whereas the others did not. The ROC analyses showed the diagnostic performance of R2*, standard ADC, fast ADC_Mono, fast ADC_Bi, and fraction of fast ADC_Bi in differentiating HCC from HM, with AUCs of 0.782, 0.712, 0.674, 0.669, and 0.677, respectively (Table 3). The AUC of mDIXON Quant (R2*), IVIM (standard ADC+fast ADC Mono+fast ADC_Bi+fraction of fast ADC_Bi), and the combination of mDIXON-Quant and IVIM parameters (R2*+standard ADC+fast ADC Mono+fast ADC_Bi+fraction of fast ADC_Bi) were 0.782, 0.739 and 0.834. The combination of mDIXON-quant and IVIM parameters shown the highest AUC value of 0.834 , and the diagnostic sensitivity and specificity were 71.1% and 88.6% respectively with a cut-off value of 0.607 (Table 4).Discussion and Conclusion
R2* was thought to be closely related to local oxygen content. In our study, R2* was significantly higher for HCC than HM, of which the reason might be that HCC cells proliferated faster and needed more oxygen supply, plus numerous immature neovascularization, making HCC less oxygen supply. Our study demonstrated that IVIM could be applied to differentiate HCC from HM. In summary, mDIXON quant combined with IVIM imaging has great potential in differential diagnosis of HCC and HM.Acknowledgements
No acknowledgement found.References
1.Motola-Kuba D, Zamora-Valdés D, Uribe M et al. Hepatocellular carcinoma. An overview. Ann Hepatol, 2006, 5 (1): 16-24.
2.Thomassen I, van Gestel YR, Lemmens VE et al. Incidence, prognosis, and treatment options for patients with synchronous peritoneal carcinomatosis and liver metastases from colorectal origin. Dis. Colon Rectum, 2013, 56 (12): 1373-80.
3. Rajasekaran Rathnakumar G, Gupta A, John F et al. A case of gastric small cell carcinoma with metastases to bone and liver.J Gastrointest Oncol, 2019, 10 (5): 1027-1031.
4. Pacicco Thomas,Ratner Shayna,Xi Yin et al. Pelvic muscle size and myosteatosis: Relationship with age, gender, and obesity.[J] .Indian J Radiol Imaging, 2019, 29: 155-162.
5. Klauss M, Mayer P, Maier-Hein K et al. IVIM-diffusion-MRI for the differentiation of solid benign and malign hypervascular liver lesions-Evaluation with two different MR scanners. Eur J Radiol, 2016, 85 (7): 1289-94.
Figures
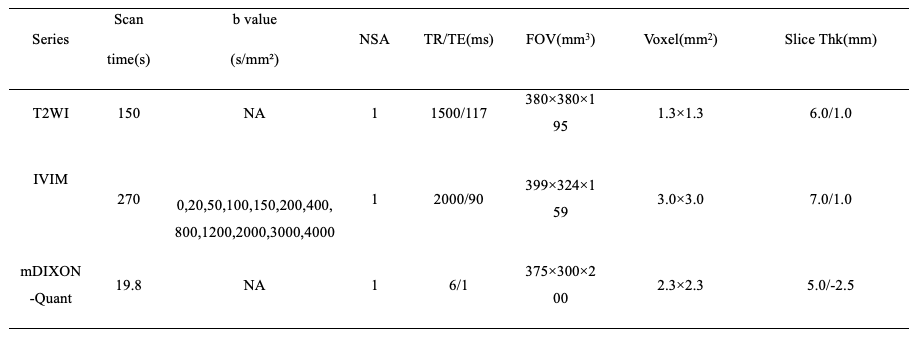
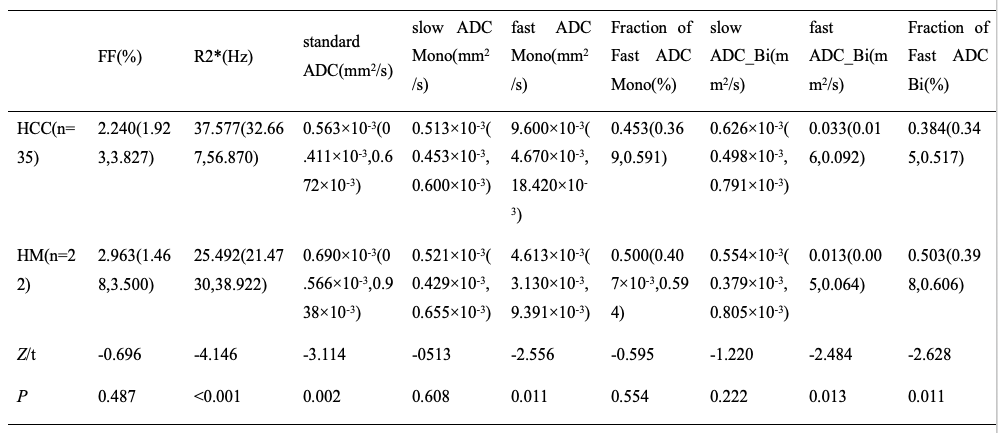
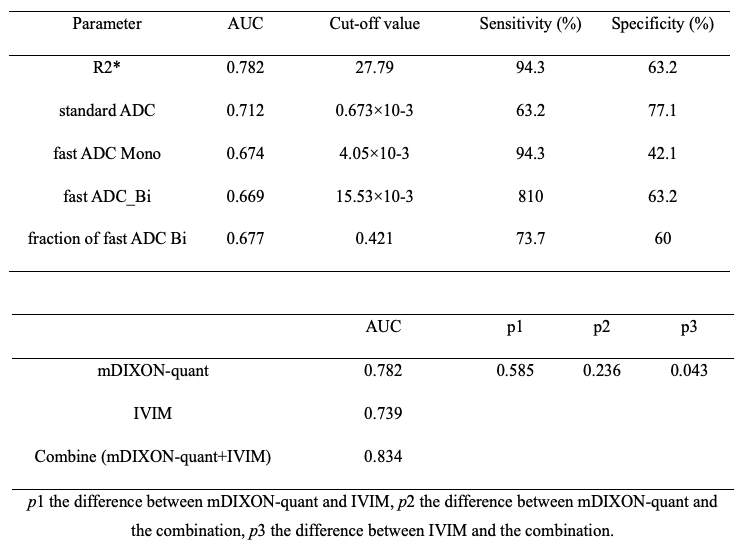
Table 3. Diagnostic performances of mDIXON-Quant and IVIM parameters.
Table 4. Difference among AUC values of mDIXON-Quant, IVIM and their combination.