4212
3D-isotropic T1WI in liver MRI with compressed sensing and artificial intelligence reconstruction1The First Hospital of Jilin University, Changchun, China, 2Philips Healthcare, Beijing, China
Synopsis
3D-isotropic volumetric data acquisition provides higher spatial resolution and signal-to-noise ratios, and facilitates multi-planar reformations. But the application was limited due to long scan time. Recently, compressed sensing (CS) has been proposed as a new method for reducing the number of k-space samples. However, one of the drawbacks of CS is a relatively lower SNR than for PI (parallel imaging). Artificial intelligence reconstruction has been introduced for improving imaging quality. The aim of this study is to investigate the feasibility of 3D-isotropic T1 weighted imaging (T1WI) with compressed sense AI reconstruction in the liver magnetic resonance imaging.
Introduction
Magnetic resonance imaging (MRI) has emerged as an important noninvasive imaging modality for the assessment of focal and diffuse liver diseases. And the performance of MRI can be substantially improved when utilizing dynamic imaging after intravenous administered gadolinium-based contrast agents[1]. 3D-isotropic volumetric data acquisition provides higher spatial resolution and signal-to-noise ratios, and facilitates multi-planar reformations. It is useful for accurate evaluation of liver and vessel anatomy in dynamic imaging and small lesion detection in late-phase acquisitions, particularly in scans enhanced with the hepatocyte-specific contrast agent Gd-EOB-DTPA[2, 3]. Compressed sensing (CS) achieves scan time reduction beyond that possible with conventional parallel imaging acceleration. However, using very high acceleration factors (AF) with very high resolution can result in degradation of image quality due to insufficient noise removal. Recently, integrating artificial intelligence (AI) into MRI reconstruction has attracted much attention to further accelerate scans. The purpose of this study is to investigate the feasibility of 3D-isotropic T1WI with compressed sensing and AI reconstruction in the liver MRI, and compare the image quality with 3D-isotropic T1WI accelerated with CS and conventional method.Methods
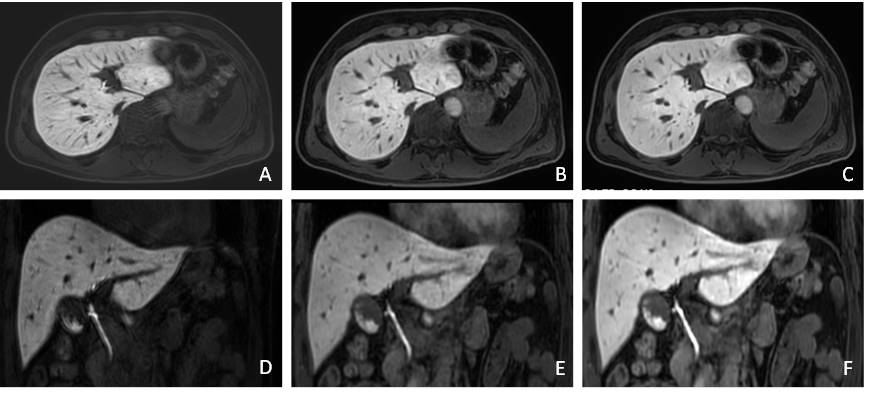
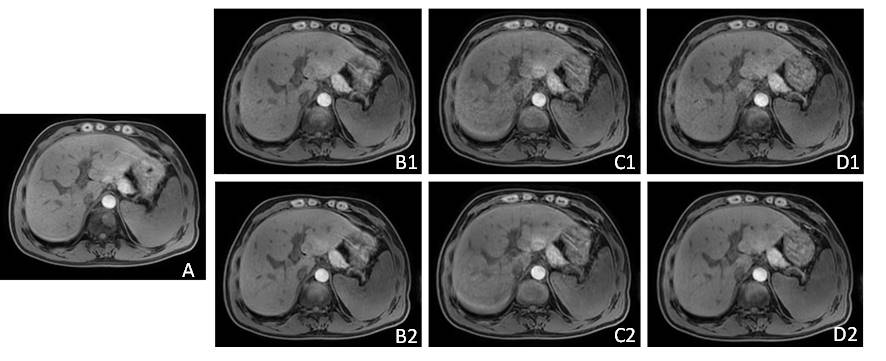
A total of 28 patients (22 males, 6 females, age range: 30-74 years, mean age: 57.07 years) were examined on a 3.0T MR scanner (Ingenia Elition X, Philips Healthcare). Each subject received customized 3D-isotropic T1WI (1.75mmx1.75mmx1.75mm) sequences with three different AF, including CS-SENSE (CS 4,CS 5, CS 6) and CS-AI technology(CS-AI 4, CS-AI 5, CS-AI 6). The commercially available unenhanced 3D non-isotropic T1WI (1.6mmx1.7mmx3.0mm) sequence was acquired with parallel imaging acceleration of 2.8 (SENSE 2.8) as reference. A total of 26 patients (18 males, 8 females, age range: 30-67 years, mean age: 51.46 years) who performed Gd-EOB-DTPA examination were examined on a 3.0T MR scanner (Ingenia Elition X, Philips Healthcare). Each subject received customized enhanced 3D-isotropic T1WI (1.75mmx1.75mmx1.75mm) at hepatobiliary phase and was reconstructed by CS-SENSE and CS-AI with acceleration of 6. The commercially available enhanced axial 3D T1WI (1.5mmx1.6mmx4mm, SENSE 2.8) and coronal 3D T1WI (1.6mmx1.7mmx3.0mm SENSE 2.8) sequences were also acquired as reference. The signal intensity and standard deviations values were measured at the liver and lesion in all groups and calculate the image signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR). Friedman test and post hoc analysis was used to detect differences in the SNR and CNR between the CS, CS-AI and reference sequence.Results
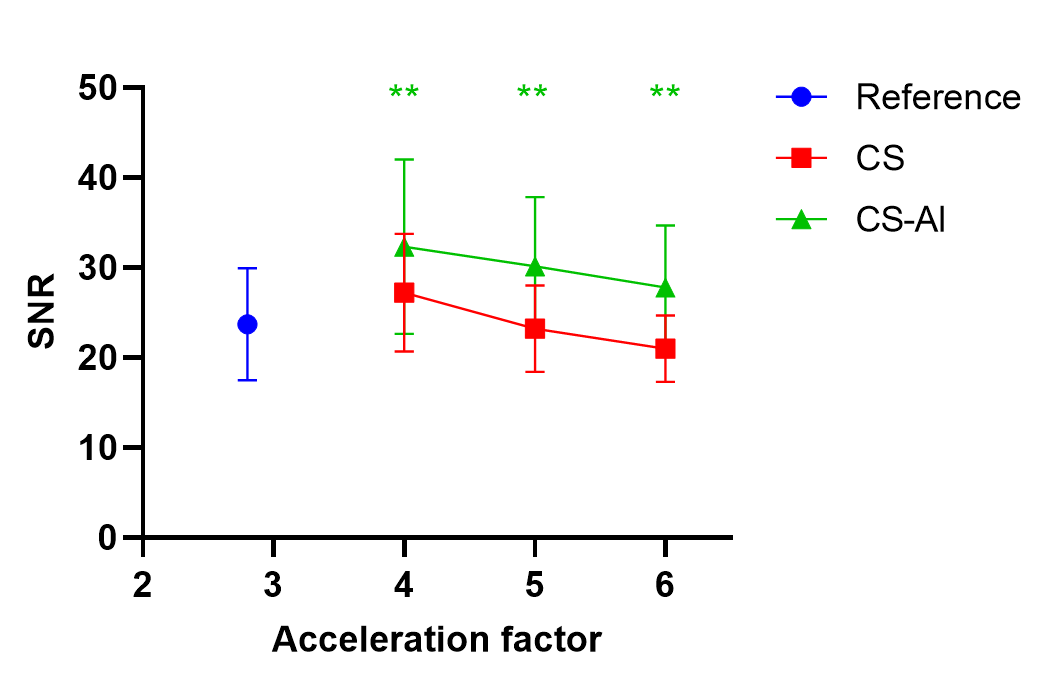
For unenhanced imaging, the scan time decreased with increasing AF (reference 15s, CS/CS-AI 4 20s, CS/CS-AI 5 18s, CS/CS-AI 6 14s). The SNR of CS-AI with different AF were all significantly higher than CS (all P<0.001). As the increasing of AF, the SNR was gradually decreasing both in CS groups and CS-AI groups. The SNR of conventional non-isotropic T1WI was superior to CS 5 and CS 6, while inferior to CS-AI 6. Considering the shorter acquisition time and satisfactory SNR, the acceleration factor 6 for CS-AI technique was recommended. For enhanced imaging, the acquisition time was 14s, 11s and 15s for 3D T1WI using CS 6/CS-AI 6, conventional axial and coronal hepatobiliary phase MRI. In axial and coronal scans, the SNR of CS-AI 6 were significantly superior to that of CS 6 and conventional hepatobiliary phase MRI (P<0.01). The CNR of CS-AI 6 was superior to CS 6 both in the axial and coronal scans, but there were no significant difference of CNR between CS 6/CS-AI 6 and conventional hepatobiliary phase MRI, except for CS-AI 6 and conventional hepatobiliary phase MRI in coronal scans.Discussion and conclusion
This preliminary study shows that the SNR of CS-AI was superior to CS and conventional 3D non-isotropic T1WI, no matter in unenhanced or hepatobiliary phase, and the CNR of CS-AI was similar or even superior to CS and the conventional 3D non-isotropic T1WI at hepatobiliary phase. Besides, with the 3D-isotropic T1WI CS-AI, we can leave out the additional coronal hepatobiliary phase scan and perform multi-planar reformations, which can evaluate tumor border more accurately and facilitate vessel reformations with MRI. Further clinical investigation and optimization of imaging parameters is needed to assess if 3D isotropic T1WI CS-AI can consistently provide diagnostic performance comparable even superior to conventional methods.Acknowledgements
NoneReferences
1.Holalkere, N., et al., Characterization of small liver lesions: Added role of MR after MDCT. 2006. 30(4): p. 591-6.
2. AlObaidy, M., et al., High-resolution 3D-GRE imaging of the abdomen using controlled aliasing acceleration technique - a feasibility study. Eur Radiol, 2015. 25(12): p. 3596-605.
3. Gustas, C., et al., Evaluation of the Articular Cartilage of the Knee Joint Using an Isotropic Resolution 3D Fast Spin-Echo Sequence With Conventional and Radial Reformatted Images. 2015. 205(2): p. 371-9.
Figures
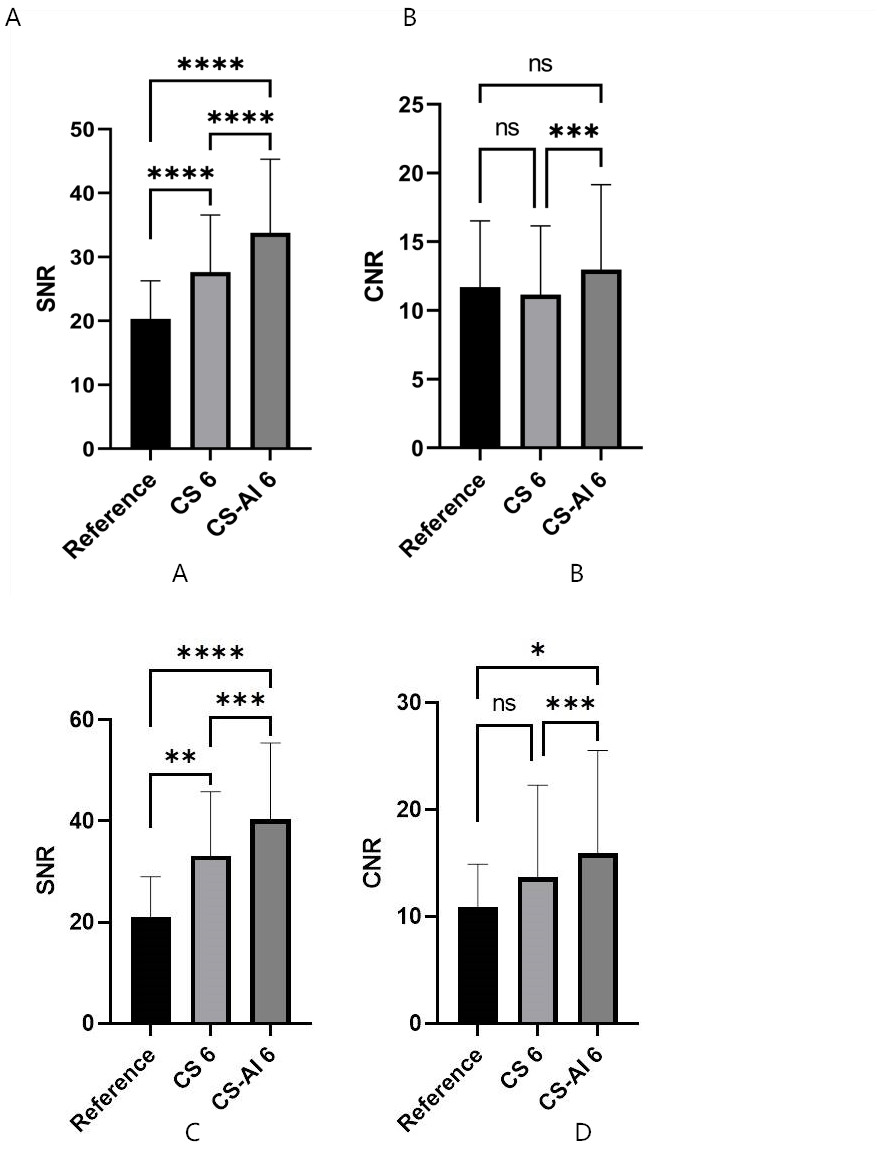
Comparison of quantitative analysis between 3D isotropic T1WI using CS 6 and CS-AI6 for axial and coronal hepatobiliary phase MRI, with conventional 3D non-isotropic T1WI as reference: A, C. SNR for axial and coronal hepatobiliary phase MRI; B, D. CNR for axial and coronal hepatobiliary phase MRI