4210
Diagnostic Performance of Gd-EOB-DTPA for Hepatocellular Carcinoma Based on LI-RADS v2018, Compared With v20171the Third People’s Hospital of Nantong, Nantong, China, 2Philips Healthcare, Shanghai, China
Synopsis
The purpose of this study was to compare the diagnostic performance of the LI-RADS v2017 and v2018 for HCC in patients with cirrhosis using Gd-EOB-DTPA. We retrospectively analyzed Clinical data of 213 patients(246 observations)with cirrhosis who underwent Gd-EOB-DTPA from October 2015 to July 2020 were retrospectively collected. MRI major features were reviewed by two radiologists. The LI-RADS categories were assigned according to v2017 and v2018. Our study showed that Updated LR-5 criteria on Gd-EOB-DTPA, the diagnostic performance of LI-RADS v2018 for diagnosing HCC is superior to v2017, particularly in small HCC (10–19 mm), with a greater sensitivity and similar specificity.
Introduction
The Liver Imaging-Reporting and Data System (LI-RADS) is a comprehensive system to standardize interpretation and radiological reporting in patients at risk of hepatocellular carcinoma (HCC). In 2018, LI-RADS is consistent with and fully integrated into the American Association for the Study of Liver Diseases (AASLD) 2018 HCC clinical practice guidance.6,16 In LI-RADS v2018, the definition of threshold growth was revised and simplified to ≥50% diameter increase in <6 months to achieve concordance with definitions advocated by AASLD and the Organ Procurement and Transplantation Network (OPTN). Another major revision was that the criteria of LR-5 (10-19 mm + arterial phase hyperenhancement [APHE] + washout = LR-5), which was revised to match those advocated by AASLD. LR-5g and LR-5us were eliminated in v2018 compared with v20171-7. Therefore, the purpose of this study was to compare the performance of LI-RADS between v2017 and v2018 for the non-invasive diagnosis of HCCs using Gd-EOB-MRI and to evaluate the effect of revisions introduced in v2018.Methods
Clinical data of 213 patients(246 observations)with cirrhosis who underwent Gd-EOB-DTPA in the Third People's Hospital of Nantong City from October 2015 to July 2020 were retrospectively collected. MRI major features were reviewed by two radiologists. The LI-RADS categories were assigned according to v2017 and v2018. The receiver operating characteristic (ROC) curve was used to compare the efficacy of LI-RADS v2017 and v2018 with histopathology results or follow-up imaging as references standards.Results
A total of 246 hepatic observations (165 HCCs, 31 non-HCC malignancies and 50 benign lesions) were included. 15.4%(38/246)observations were assigned a different category according to LI-RADS v2018 compared with v2017. The threshold growths of 84.6% (33/39) observations in v2017 were revised to subthreshold growth in v2018, 30.3%(10/33)observations were down-categorized (categorized as LR-5 by LI-RADS v2017 to LR-4 by v2018, n=7; categorized as LR-4 by LI-RADS v2017 to LR-3 by v2018, n=3 ). 45.9% (28/61) observations categorized LR-4 by LI-RADS v2017 were up-categorized to LR-5 by v2018 due to changes in the LR-5 criteria, and 89.3%(25/28)were sHCC. When adopting LR-5 as a predictor of HCC, the sensitivity (66.7% vs 55.8%, P=0.001), and accuracy(83.9% vs 77.9%, P<0.001) were increased for LI-RADS v2018 compared with v2017, particularly in small observations (10–19 mm), LI-RADS v2018 yielded much higher sensitivity than v2017(62.9% vs 40.4%, P<0.001), with relatively little impairment of specificity(88.7% vs 91.2%, P=0.250). However, the diagnostic performances of MRI for diagnosing HCC were not changed while adopting LR-4/5 as a predictor.Conclusions
Updated LR-5 criteria on Gd-EOB-DTPA, the diagnostic performance of LI-RADS v2018 for diagnosing HCC is superior to v2017, particularly in small HCC (10–19 mm), with a greater sensitivity and similar specificity.Acknowledgements
noneReferences
[1] Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma[J]. Hepatology, 2018, 67(1):358-380.
[2] American College of Radiology: Liver Imaging Reporting and Data System. https://nrdr.acr.org/lirads/. 2018.
[3] Yoon JH, Lee JM, Lee YJ, et al. Added Value of sequentially performed gadoxetic acid-enhanced liver MRI for the diagnosis of small (10-19 mm) or atypical hepatic observations at contrast-enhanced CT: A prospective comparison[J]. J Magn Reson Imaging, 2019, 49(2):574-587.
[4] Song JS, Choi EJ, Hwang SB, et al. LI-RADS v2014 categorization of hepatocellular carcinoma: Intraindividual comparison between gadopentetate dimeglumine-enhanced MRI and gadoxetic acid-enhanced MRI[J]. Eur Radiol, 2019, 29(1):401–410.
[5] Ko A, Park HJ, Lee ES, et al. Comparison of the diagnostic performance of the 2017 and 2018 versions of LI-RADS for hepatocellular carcinoma on gadoxetic acid enhanced MRI[J]. Clin Radiol, 2020, 75(4):319.e1-319.e9.
[6] Ren AH, Zhao PF, Yang DW, et al. Diagnostic Performance of MR for Hepatocellular Carcinoma Based on LI-RADS v2018, Compared With v2017[J]. J Magn Reson Imaging, 2019, 50(3):746-755.
[7] Kierans AS, Song C, Gavlin A, et al. Diagnostic Performance of LI-RADS Version 2018, LI-RADS Version 2017, and OPTN Criteria for Hepatocellular Carcinoma[J]. AJR Am J Roentgenol, 2020, 215(5):1085-1092.
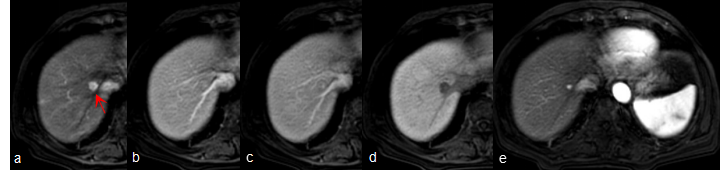
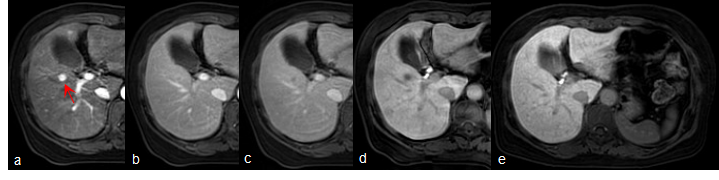
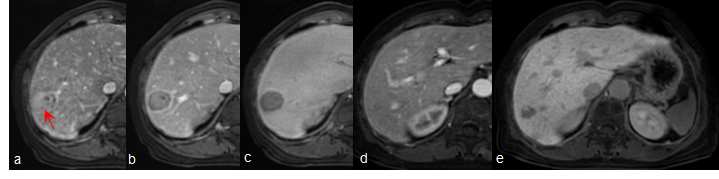
Figures