4181
Evaluation of Secondary Prevention Effectiveness of Ginkgo Biloba Extract (EGb 761) in Acute Ischemic Stroke by QSM and Venous Oxygen Saturation1Department of Radiology, Ningbo First Hospital, Ningbo Hospital of Zhejiang University, Ningbo, China, 2Department of Neurology, Ningbo First Hospital, Ningbo, China, 3Department of Neurosurgery, Ningbo First Hospital, Ningbo, China, 4Department of Gerontology, Ningbo First Hospital, Ningbo, China, 5MR Scientific Marketing, SIEMENS Healthineers, Shanghai, China
Synopsis
In this study, we applied quantitative susceptibility mapping (QSM) and venous oxygen saturation measurement in acute ischemic stroke patients who took ginkgo biloba extract (EGb 761) treatment. EGb 761’s secondary prevention effectiveness of ischemic stroke patients with cerebral microbleeds was similar to Aspirin. Furthermore, Ginkgo biloba extract could not only improve neuroprotective efficiency and prognosis by increasing oxygen saturation of the vein near infarction, but also could reduce the incidence of adverse side effects such as gastrointestinal ulcers and bleeding usually caused by Aspirin.
Introduction
Ginkgo biloba extract (EGb 761) is a standardized dry extract of Ginkgo biloba leaves traditionally used in eastern Asia. It can eliminate oxygen-free radicals and reduce the consumption of antioxidant enzymes, also can improve neural function by reducing oxidative stress injury. EGb 761 also has anti-inflammatory and anti-thrombotic capabilities in stroke, cerebrovascular diseases treatment, and central nervous system protection. In order to evaluate the number of cerebral microbleeds and venous oxygen saturation of patients treated with EGb 761 after ischemic stroke. Then analyzed EGb 761’s effectiveness and safety in preventing stroke recurrence, whether it could provide clinical evidence for individualized secondary prevention in patients with cerebral infarction and microbleeds.Methods and Materials
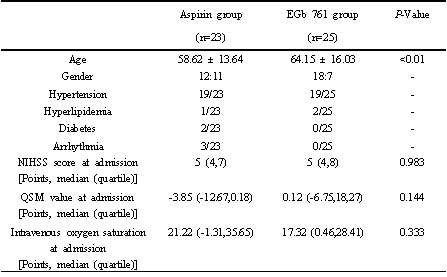
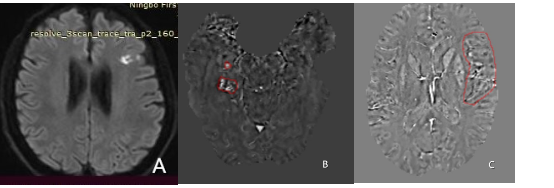
Totally 49 acute ischemic stroke patients were enrolled in this study. 24 patients were assigned to the Aspirin treatment group and 25 patients were assigned to the EGb 761 treatment group according to the order of discharge. All patients received standard medicine doses followed by the 2014 Chinese guidelines for diagnosis, treatment, and secondary prevention of acute ischemic stroke. At discharge, patients of the EGb 761 group were given Ginkgo biloba extract (Yangzijiang pharmaceutical, 40mg), 2 tablets at a time, 3 times a day; patients of the Aspirin group were given Aspirin enteric-coated tablets 100 mg once a day. All patients underwent routine MR imaging examination and quantitative susceptibility mapping (QSM) on a 3.0T system (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) at admission, discharge, and follow-up observation in the third and sixth months. The observational events included cerebral hemorrhage and cerebral infarction. QSM was used to calculate the magnetic susceptibility of cerebral microbleeds and cerebral venous saturation in ROIs. According to the previous study’s result, there was a certain relationship between magnetic susceptibility value and cerebral venous saturation, which can be converted by the following formula: Δ χVein-Tissue = κC χdo.Hct(1-Y) χVein-Tissue = κC χdo.Hct(1-Y) (Δχ: susceptibility value; Y: blood oxygen saturation; Δ χVein-Tissue: normal susceptibility difference between stroke side and contralateral side; χDo: the ratio of the susceptibility (4π-χ0.27ppm) of hypoxic and total oxygenated blood per unit blood cell volume[1]; HCT: the volume fraction of venous red blood cells in the pia minges). Obviously, the greater susceptibility difference between the stroke side and the normal brain tissue side was, the smaller the change of venous oxygen saturation was. The independent sample T-test and Mann-Whitney U-test were used to compare parameters between two groups. Corrected P-value < 0.05 were considered as significant difference. NIHSS score and modified Rankin Scale (mRS) were used during the follow-up periods to analyze the relationship among susceptibility, venous oxygen saturation, and treatment efficiency of neurological deficit.Results
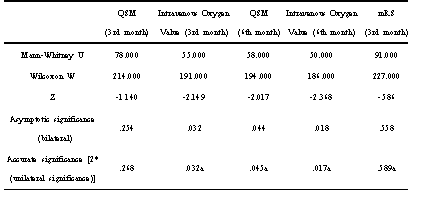
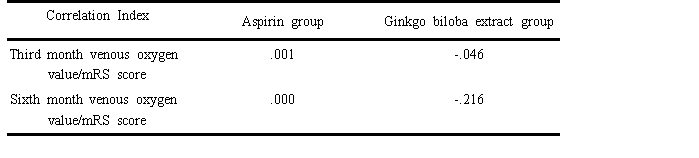
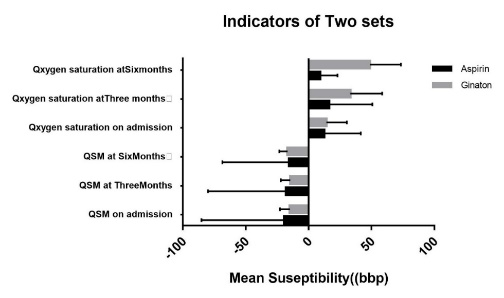
There was no significant difference in baseline age, gender, and admission to NIHSS (P < 0.05) (Table 1.2). After 3 and 6 months of follow-up, QSM values showed that the magnetic susceptibility of patients in both groups remained stable, suggesting that the microbleeds foci remained stable and no new microbleeds were observed, but the venous oxygen saturation of the EGb 761 treatment group has apparently increased at the third and sixth months of follow-up (Figure 1), and the venous oxygen saturation was negatively correlated with the mRS score (Table 3). Furthermore, the venous oxygen saturation’s improvement of the EGb 761 treatment group was more marked than that of the Aspirin group.Conclusion
Ginkgo biloba extract played a similar role as Aspirin in the secondary prevention of cerebral microbleeds in patients with ischemic stroke. However, EGb 761 could improve neuroprotective efficiency by increasing venous oxygen saturation, meanwhile, it could reduce the incidence of adverse side effects such as gastrointestinal ulcers and bleeding caused by Aspirin.Abbreviations
EGb: Ginkgo biloba extract;AIS: artemisinin combination therapy;
PAF: platelet-activating factor;
QSM: quantitative susceptibility mapping;
SWI: susceptibility-weighted imaging;
NIHSS: National Institution of Health Stroke Scale;
mRS: modified Rankin Scale.
Acknowledgements
No acknowledgement found.References
[1] Haacke EM, Xu Y, Cheng YC, Reichenbach JR. Susceptibility weighted imaging (SWI). Magn Reson Med. 2004. 52(3): 612-8.
[2] Liu L, Wang D, Wong KS, Wang Y. Stroke and stroke care in China: huge burden, significant workload, and a national priority. Stroke. 2011. 42(12): 3651-4.
[3] DeFeudis FV. Ginkgo Biloba Extract (EGb 761): Pharmacological Activities and Clinical Applications. 1991. Elsevier, Paris.
[4] Commission CP. Pharmacopeia of the People’s Republic of China. 2015. China Medical Science Press, Beijing.
[5] Diamond BJ, Shiflett SC, Feiwel N, et al. Ginkgo biloba extract: mechanisms and clinical indications. Arch Phys Med Rehabil. 2000. 81(5): 668-78.
[6] Research Progress on pharmacological action and clinical application of Ginkgo biloba extract. Liaoning Journal of Traditional Chinese Medicine. 2017. 44(02): 426-429.
[7] Singh SK, Srivastav S, Castellani RJ, Plascencia-Villa G, Perry G. Neuroprotective and Antioxidant Effect of Ginkgo biloba Extract Against AD and Other Neurological Disorders. Neurotherapeutics. 2019. 16(3): 666-674.
[8] Liang W, Xu W, Zhu J, et al. Ginkgo biloba extract improves brain uptake of ginsenosides by increasing blood-brain barrier permeability via activating A1 adenosine receptor signaling pathway. J Ethnopharmacol. 2020. 246: 112243.
[9] Liu T, Surapaneni K, Lou M, Cheng L, Spincemaille P, Wang Y. Cerebral microbleeds: burden assessment by using quantitative susceptibility mapping. Radiology. 2012. 262(1): 269-78.
[10] Fan AP, Bilgic B, Gagnon L, et al. Quantitative oxygenation venography from MRI phase. Magn Reson Med. 2014. 72(1): 149-59.
Figures