4170
Fast 3D Wheel Acquisition: Comparison of Efficacy for Cerebral MR Angiography with Conventional Parallel Imaging
Satomu Hanamatsu1, Kazuhiro Murayama2, Yoshiharu Ohno3, Kaori Yamamoto4, Yuki Obama1, Hirotaka Ikeda1, Hiroyuki Nagata1, Masato Ikedo4, Masao Yui4, Akiyoshi Iwase5, and Hiroshi Toyama1
1Radiology, Fujita Health University, School of Medicine, Toyoake, Japan, 2Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University, School of Medicine, Toyoake, Japan, 3Radiology, Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University, School of Medicine, Toyoake, Japan, 4Canon Medical Systems Corporation, Otawara, Japan, 5Radiology, Fujita Health University, Hospital, Toyoake, Japan
1Radiology, Fujita Health University, School of Medicine, Toyoake, Japan, 2Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University, School of Medicine, Toyoake, Japan, 3Radiology, Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University, School of Medicine, Toyoake, Japan, 4Canon Medical Systems Corporation, Otawara, Japan, 5Radiology, Fujita Health University, Hospital, Toyoake, Japan
Synopsis
To the best of our knowledges, there are no major papers that assess the influence of Fast 3D wheel to cerebral MR angiography in patients with cerebrovascular diseases. We hypothesize that “Fast 3D wheel (Fast 3Dw)” has a potential to reduce examination time without degradation of image quality and aneurysm or vascular evaluations, when compared with PI. The purpose of this study was to directly compare the efficacy of Fast 3Dw for cerebral MR angiography with conventional PI in patients with cerebral aneurysm.
Introduction
Cerebral MR angiography has been one of the fundamental imaging tools for screening or evaluation of cerebrovascular diseases in routine clinical practice. Since 2004, conventional parallel imaging (PI) techniques has been widely applied in not only neuro, but also other MR imaging in routine clinical practice. The two parallel imaging methods are most commonly used on clinical scanners today, sensitivity encoding (SENSE) and generalized auto-calibrating partially parallel acquisitions (GRAPPA) in all MR vendors1, 2. In addition, compressed sensing is clinically utilized by several MR vendors and tested for its’ utility as compared with PI3-6. One of the drawbacks of CS is reduced quantitative and qualitative image qualities3-6, and deep learning reconstruction (DLR) would be better to be applied as well as CS in routine clinical practice6. In this situation, “Fast 3D mode” is recently introduced from Canon Medical Systems as new methods for k-space data acquisition. In contrast to conventional 3D MRI, which mainly obtains k-space data with a slice encoding in k-space for each TR, “Fast 3D multiple”, which is one of the Fast 3D acquisitions, obtains k space data with multiple slices encoding in each TR. In addition, another Fast 3D acquisition named as “Fast 3D wheel” obtains reduced k-space data as segmented radial scan from low frequency data at k-space center to the high frequency data at the periphery of k-space. When applied these techniques, we can reduce examination time without degradation of image quality and obtain good image quality without DLR in routine clinical practice. To the best of our knowledges, there are no major papers that assess the influence of Fast 3D wheel to cerebral MR angiography in patients with cerebrovascular diseases. We hypothesize that “Fast 3D wheel (Fast 3Dw)” has a potential to reduce examination time without degradation of image quality and aneurysm or vascular evaluations, when compared with PI. The purpose of this study was to directly compare the efficacy of Fast 3Dw for cerebral MR angiography with conventional PI in patients with cerebral aneurysm.Materials and Methods
50 consecutive candidates with unruptured cerebral aneurysm underwent conventional MRA by PI and Fast 3Dw methods at a 3T scanner (Vantage Centurian: Canon Medical Systems Corporation). For quantitative vascular clarity assessment, signal-to-noise ratios (SNRs) of internal carotid artery (ICA), middle cerebral artery (MCA) and white matter (WM) and contrast noise ratios (CNRs) between white matter and ICA or MCA were assessed by ROI measurements as following formula.- SNR = SIICA/SDWM; SIMCA/SDWM [1]
- CNR = (SIICA-SIWM) / {(SDICA + SDWM) / 2} or (SIMCA-SIWM) / {(SDMCA + SDWM) / 2} [2]
Results
Representative cases are shown in Figure 1. Comparison of mean examination times, SNRs and CNRs between PI and Fast 3Dw are shown in Figure 2. Mean examination time of Fast 3Dw was significantly shorter than that of PI (p<0.05). SNR of Fast 3Dw was significantly higher than that of PI (p<0.05). Compared results of size of aneurysms and diameters of ICA and MCA between PI and Fast 3Dw are shown in Figure 3. There were no significant differences of between PI and Fast 3Dw (p>0.05). Figure 4 shows interobserver agreements of vascular clarity, artifacts and diagnostic confidence level of PI and Fast 3Dw and compared results of each qualitative index between PI and Fast 3Dw. Interobserver agreement of each qualitative index on Fast 3Dw was significant and substantial or excellent (0.78≤κ≤0.81, p<0.001), although that on PI was significant and substantial (0.66≤κ≤0.79, p<0.001). When compared each qualitative index between PI and Fast 3Dw, there were no significant differences (p>0.05).Conclusion
Fast 3Dw has a superior potential to conventional PI for examination time reduction with keeping image quality and accuracies for aneurysm size and vascular diameter measurements in patients with cerebral aneurysm.Acknowledgements
This work was technically and financially supported by Canon Medical Sytstems Corporation.References
- Deshmane A, Gulani V, Griswold MA, Seiberlich N. Parallel MR imaging. J Magn Reson Imaging. 2012 Jul;36(1):55-72
- Hamilton J, Franson D, Seiberlich N.Prog. Recent advances in parallel imaging for MRI. Nucl Magn Reson Spectrosc. 2017 Aug;101:71-95.
- Jaspan ON, Fleysher R, Lipton ML.Br. Compressed sensing MRI: a review of the clinical literature. J Radiol. 2015;88(1056):20150487.
- Feng L, Benkert T, Block KT, Sodickson DK, Otazo R, Chandarana H. Compressed sensing for body MRI. J Magn Reson Imaging. 2017 Apr;45(4):966-987.
- Ikeda H, Ohno Y, Murayama K, Yamamoto K, Iwase A, Fukuba T, Toyama H. Compressed sensing and parallel imaging accelerated T2 FSE sequence for head and neck MR imaging: Comparison of its utility in routine clinical practice. Eur J Radiol. 2021 Feb;135:109501.
- Ueda T, Ohno Y, Yamamoto K, Iwase A, Fukuba T, Hanamatsu S, Obama Y, Ikeda H, Ikedo M, Yui M, Murayama K, Toyama H. Compressed sensing and deep learning reconstruction for women's pelvic MRI denoising: Utility for improving image quality and examination time in routine clinical practice. Eur J Radiol. 2021 Jan;134:109430.
Figures

Figure 1. 60-year-old female patient with A-com aneurysm.
Each of
the examination times was as follows: MRA with PI, 390s and MRA with Fast 3Dw,
174s. Diameter of aneurysm (arrow) and
diameters of bilateral ICAs and MCAs were measured as follows: MRA with PI, 1.90mm,
3.82mm, 3.24mm, 1.24mm and 1.17mm; MRA with Fast 3Dw-A, 1.86mm, 3.86mm, 3.48mm,
1.37 and 1.26mm. Vascular clarity,
artifact and aneurysm depiction level of Fast 3Dw were 5, 1 and 5, and those of
PI were 5, 1 and 5.
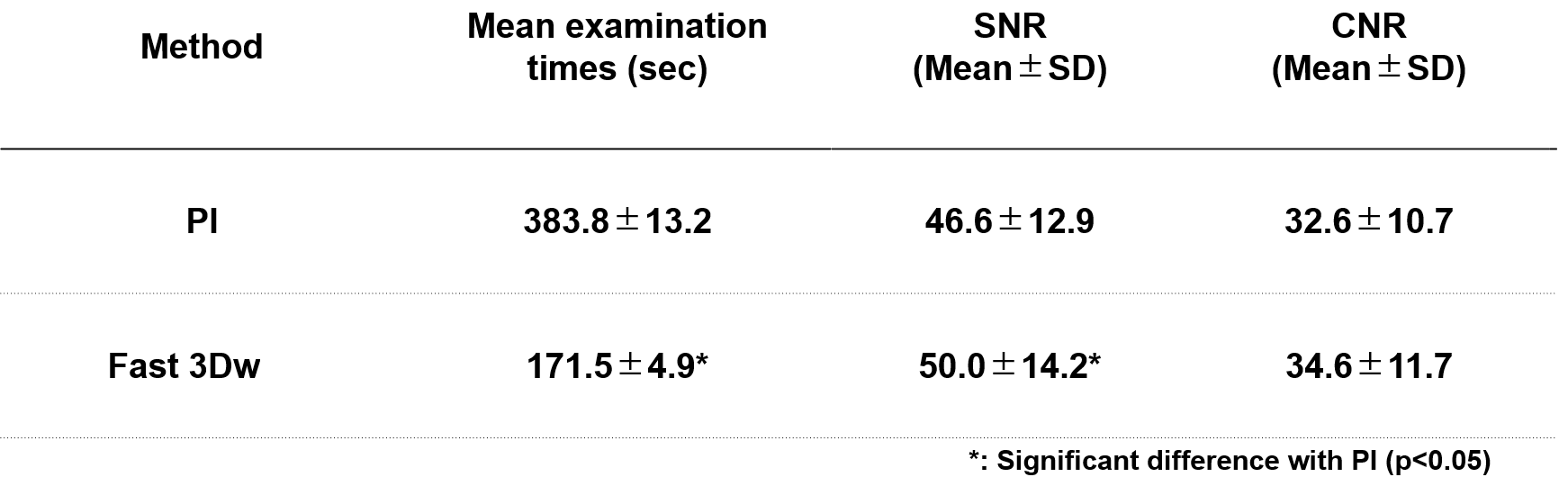
Figure 2. Compared results of mean
examination times, SNRs and CNRs between PI and Fast 3Dw. Mean examination time and SNR of
Fast 3Dw were significantly shorter or higher than those of PI (p<0.05).

Figure 3. Compared results of size of aneurysms and diameters
of ICA and MCA between PI and Fast 3Dw. There were no significant differences of
size of aneurysm and diameters of ICA and MCA between PI and Fast
3Dw (p>0.05).
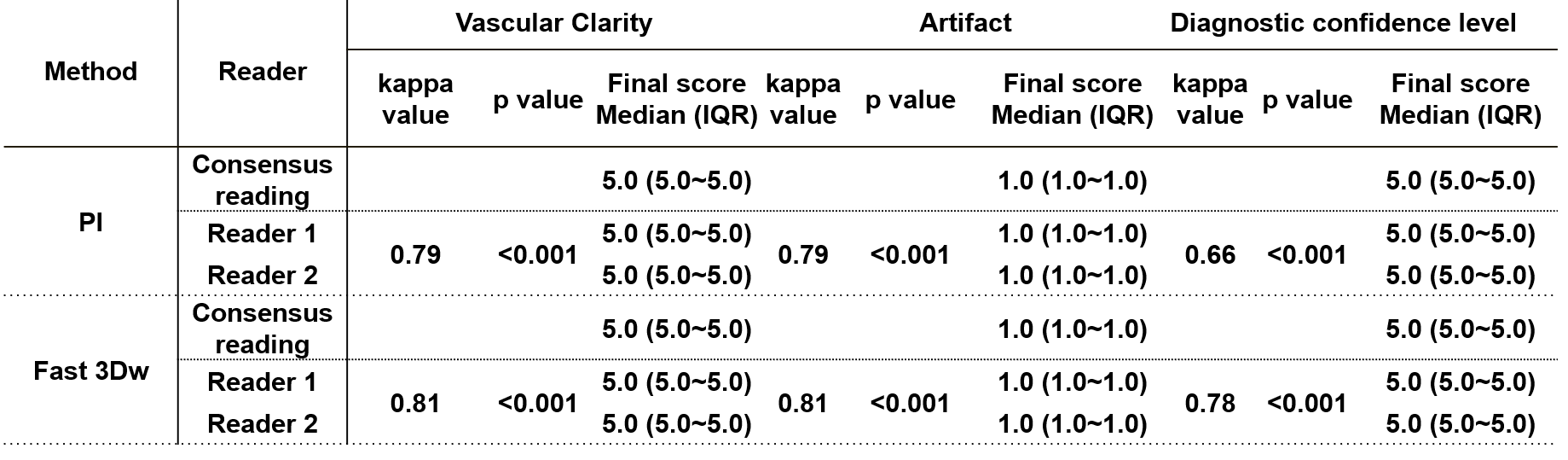
Figure 4. Interobserver agreements of vascular clarity,
artifacts and diagnostic confidence level of PI and Fast 3Dw and compared
results of each qualitative index between PI and Fast 3Dw. Inter-observer agreement of each index by two methods were
determined as substantial or excellent (0.66≤κ≤0.81, p<0.001). There were no significant differences of
vascular clarity, artifacts and diagnostic confidence level between PI and Fast
3Dw (p>0.05).
DOI: https://doi.org/10.58530/2022/4170