4168
Comparative study between the Slow Infusion MR angiography and CT angiography in detection of the Adamkiewicz artery1Radiology, Nippon Medical School Chiba Hokusoh Hospital, Inzai, Chiba, Japan, 2Radiology, Nippon Medical School Hospital, Tokyo, Japan, 3Cardiovascular surgery, Nippon Medical School Chiba Hokusoh Hospital, Inzai, Chiba, Japan, 4Radiology, Nippon Medical School Musashikosugi Hospital, Kawasaki, Kanagawa, Japan
Synopsis
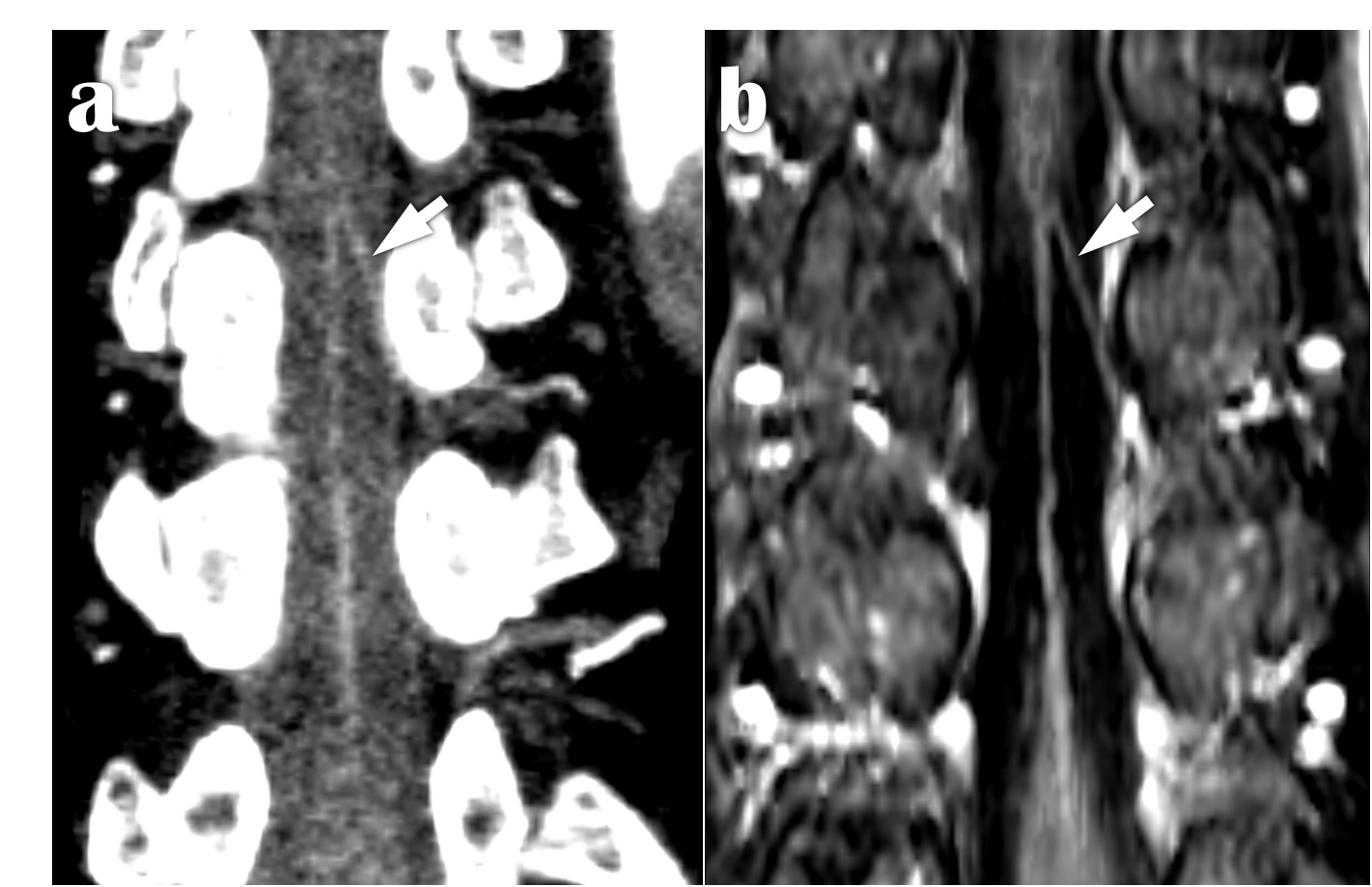
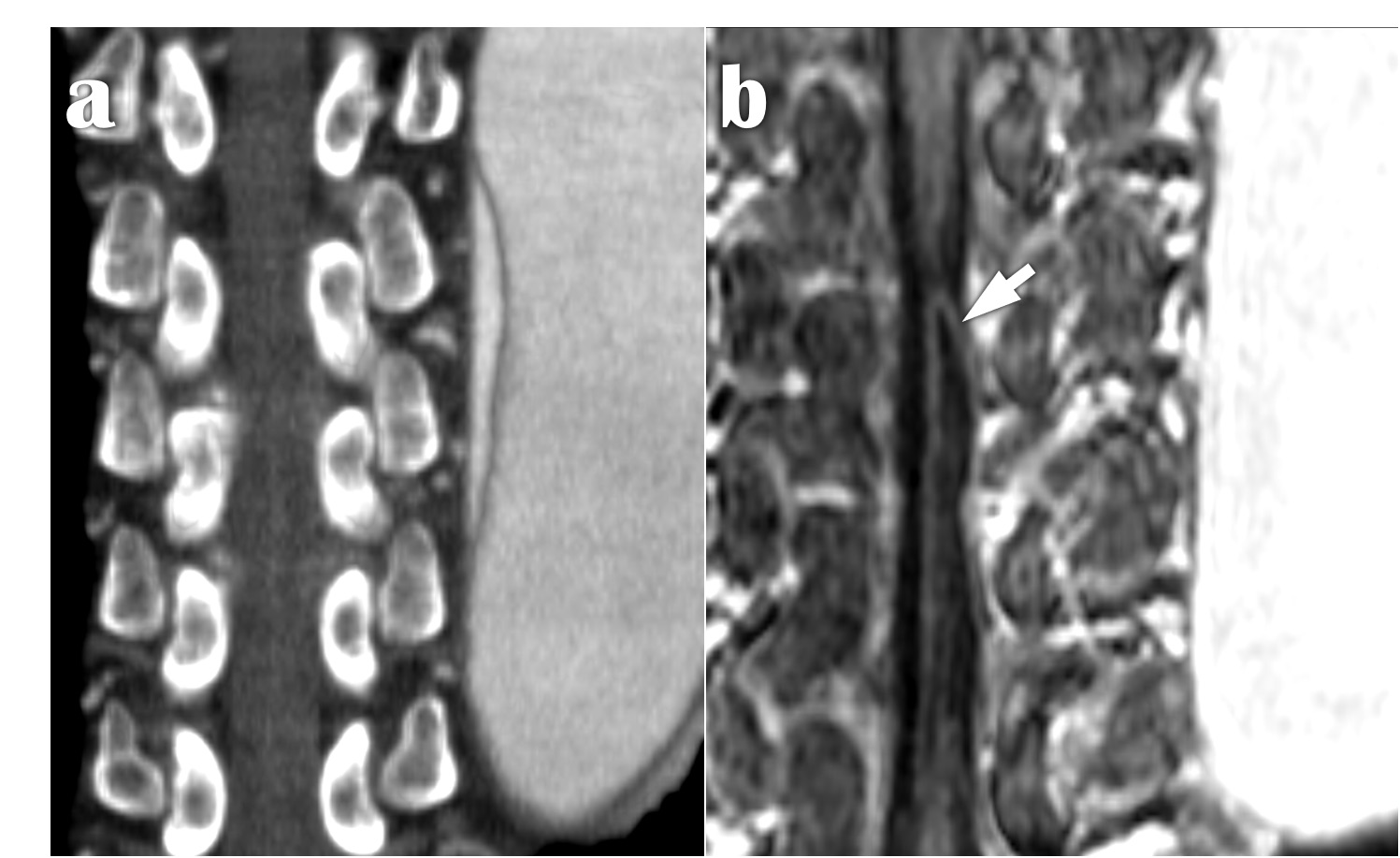
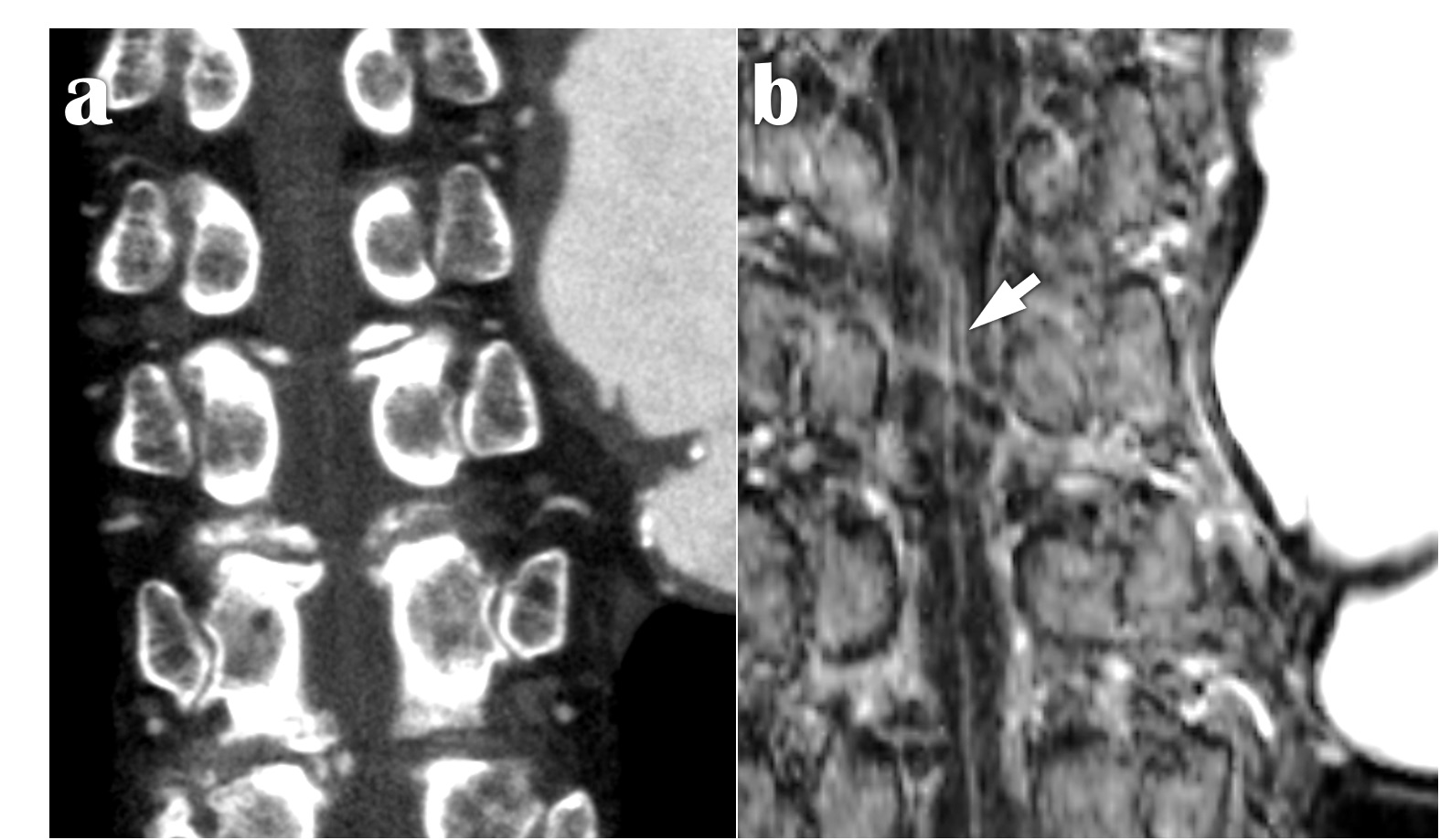
The Slow-Infusion MRA with SPGR provided the higher detectability of the AKA with whole patients, all AD patients, and with the AD patients whose AKA originating from false lumen in comparison with CTA.
Materials and Methods: Fifty-six patients with thoracic or thoracoabdominal aortic disease (43 males and 13 females, mean age; 69 [range 40–92] years old, 25 patients of aortic dissection (AD) and 31 patients of aortic aneurysm) were examined with both CTA and Slow Infusion-MRA to detect AKA between April 2018 and September 2021 and were enrolled in this study. CTA imaging: The level from the fifth thoracic to the third lumber vertebra was scanned using a 64-row CT scanner. Iodine contrast medium (370 mg/ml) with the amount of 2 ml per kg of body weight was injected at the speed of 3–5ml/sec and followed by 50 mlsaline flush. Scan was triggered by a bolus tracking system with the region of interest (ROI) at the diaphragm level of the descending aorta.MRA imaging: MRA was performed using a 3T whole-body scanner and 3-dimensional fast SPGR sequence with a chemical shift-selective fat-suppression technique was used. The following specific imaging parameters were used for the Slow Infusion-MRA: repetition time/echo time; 7.1/2.3 ms, flip angle; 14 degrees, field of view (FOV); 320 x 320 mm2; image matrix; 388 x 388, the resulting pixel size; 1 x 1 mm, slice thickness; 0.8 mm. Gadoteridol contrast medium with the amount of 0.1 mmol per kg of body weight was injected at the speed of 0.1-0.2 ml/sec, the peak contrast timing was set to one-thirds middle of the scan time, and images were acquired during 1–5 minutes.Image analysis: Data of CTA and MRA was analyzed using a 3-dimensional workstation. The degree of detectability of AKA was stratified into previously reported 4 classifications1 as follows: Grade I; AKA is not depicted, Grade II; intradural vessel is partially depicted but the continuity to extradural segment is unclear, Grade III; AKA is depicted but its origin is unclear, Grade IV; AKA and the continuity from the extradural segment is clearly depicted. Grades III and IV were considered as sufficient for AKA diagnosis. Among total patients and the sub-groups based on anatomical features, the detection rates with MRA and CTA were statistically compared.
Results: The significantly higher detection rates with MRA vs. CTA were demonstrated among total 56 patients (92.9 % vs. 73.2 %, [p = 0.006]). The average of grade of MRA was also significantly higher compared to CTA (3.71 vs. 3.09). In the 25 aortic dissection patients, the detection rates with MRA vs. CTA were 92.0 % vs. 68.0 %, [p = 0.034], among 8 AD patients whose AKAs originate from the false lumen (87.5 % vs. 12.5 %, [p = 0.003]). In the 27 patients with aneurysm at thoracic descending aorta, the detection rates with MRA vs. CTA were 92.6 % vs. 74.1 %, [p = 0.068]. The detection rates of 10 cases whose AKA originate from the aneurysmal parts were 80.0 % vs. 70.0 %, [p = 0.61], on the other hand, the detection rates of 17 cases whose AKA originate from the non-aneurysmal parts were 100 % vs. 76.5 %, [p = 0.033].
Discussion: While CTA has been regarded as more standard mainly due to the convenience in the imaging, the various attempts in Gd-enhanced MRA at 3-T improved the detectability of AKA2,3. As the scanning method of Gd-enhanced MRA, the Time-Resolved method based on the spin-echo has been more frequently used to detect AKA so far4,5,6. In contrast, we applied the Slow-Infusion MRA to gain better detection of small arteries as AKA with the advantage of the spatial resolution. Then we modified the parameters as TR/TE and flip angle from the previous report of Slow-Infusion MRA to detect AKA7 to keep high signal/noise ratio with high matrix, thin slice, and wide FOV. Further, we softly compressed the patient’s abdomen using cushion to keep uniform respiration and used spine radio frequency coil in the cases who did not require the detailed evaluation of ascending aorta. These maneuvers could greatly reduce the influences of respiration and heart beating. Notably, the feasibility of the Slow-Infusion MRA in the AD patients whose AKA originating from false lumen was demonstrated from our results, despite it has been supposed as difficult to detect the AKA using CTA or the Time-Resolved MRA due to the large difference in blood flow velocity between the true and false lumen8,9.
Conclusion: The high spatial resolution of Slow Infusion-MRA could be preferable to detect AKA prior to various thoracic or thoracoabdominal aortic surgery.
Acknowledgements
No acknowledgement found.References
1. Thorsten A. Bley, et al. Presurgical Localization of the Artery of Adamkiewicz with Time-resolved 3.0-T MR Angiography. Radiology, 2010
2. Kunihiro Yoshioka, et al. MR angiography and CT angiography of the artery of Adamkiewicz: noninvasive preoperative assessment of thoracoabdominal aortic aneurysm. Radiographics. 2003;23(5):1215-25.
3. Dominik Taterra, et al. Artery of Adamkiewicz: a meta-analysis of anatomical characteristics. Neuroradiology, 2019 61:869-88
4. Yamada N, et al. MRA of the Adamkiewicz artery: a preoperative study for thoracic aortic aneurysm.J Computer Assist Tomography 2000; 24: 362-368.
5. Hideki Hyodoh, et al. Usefulness of Preoperative Detection of Artery of Adamkiewicz with Dynamic Contrast-enhanced MR Angiography. Radiology, 2005, 236:1004-1009.
6. Hidenobu Takagi, et al. Identifying the Adamkiewicz artery using 3-T time-resolved magnetic resonance angiography: its role in addition to multidetector computed tomography angiography. Jpn J Radiology. 2015, 33: 749-56.
7. Kunihiro Yoshioka, et al. MR angiography and CT angiography of the artery of Adamkiewicz: state of the art. Radiographics 2006; 26: S63-S73
8. Kunihiro Yoshioka, et al. CT Angiography and MR Angiography of the Artery of Adamkiewicz. J Jpn Coll Angiol, 2009, 49: 517–521
9. Kenichiro Takahashi, et al. Utility of 4D Flow MRI in Thoracic Aortic Diseases: A Literature Review of Clinical Applications and Current Evidence. Magnetic Resonance in Medical Sciences, 2021
Figures