4148
The application of whole-heart coronary MRA with compressed sensing in patients with atrial fibrillation1Wuhan Asia General Hospital, WuHan, China, 2Philips Healthcare, Beijing, China
Synopsis
The whole-heart coronary MRA with compressed sensing (CS) technique is a novelly noninvasive, contrast agent-free, and radiation-free technique for evaluating coronary artery disease[2] [3].Patients with atrial fibrillation have irregular heartbeat, which brings uncertainty to the coronary MRA image quality. Results of this study indicated that there was no statistical difference in coronary artery image quality with CS acceleration factors of 2, 4, 6 between sinus rhythm and atrial fibrillation patients, which suggested that whole-heart coronary MRA with CS technique could also be applied inpatients with atrial fibrillation.
Introduction
The whole-heart coronary MRA technique has advantages ofnoninvasive, contrast agent-free, and radiation-free to evaluatecoronary artery disease.Compressed Sensing (CS) is a novel technique to accelerate scanning with flexible acceleration factors(AFs) settings.Atrial fibrillation has been widely concerned as a common complication ofdiaphragm navigator-based free-breathingcoronary MRA,which might increase scanning difficulty and harm image quality.The purpose of this study is to explore if the whole-heart coronary MRA with different compressed sensing AFscould be applied in patients withatrial fibrillation.Methods
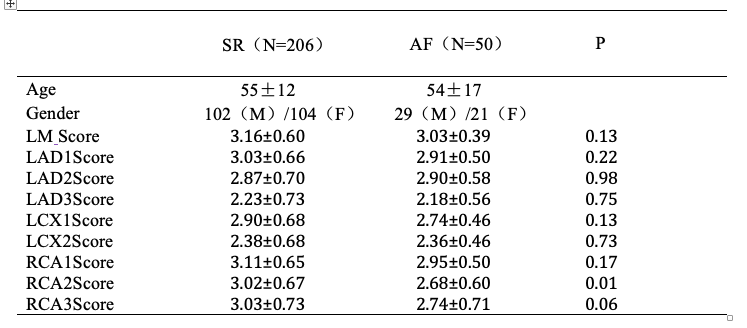
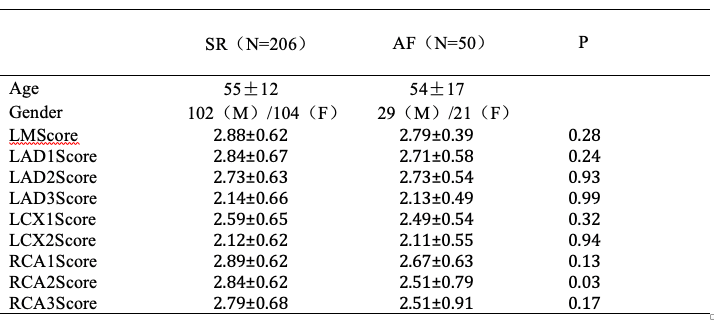
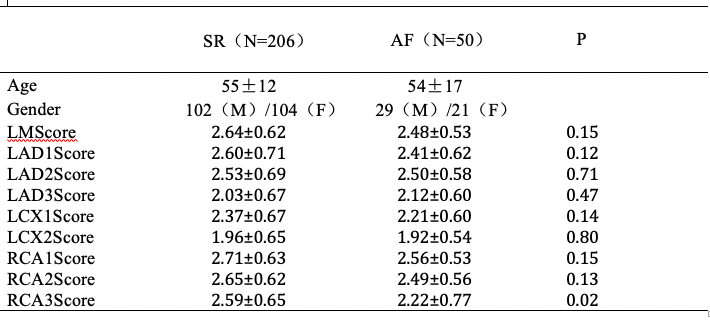
This study was approved by the institutional IRB. 206 patients with sinus rhythm(SR)and 50 patients with atrial fibrillation(AF)were enrolled and under went whole-heart coronary MRA on a 1.5T MR scanner (Ambition, Philips Healthcare, the Netherlands) with a 32-channel body coil. The whole-heart coronary MRA was based on a free-breathing electrocardiogram-triggered navigator-gated steady-state free precession sequence, which was accelerated by CS[1]. The MRA protocols with different CS AFs were implemented in random orders for each subject. The electrocardiogram trigger delay was identified by visualizing the quiescent period of the right coronary artery (RCA) using a 100 phases breath-hold cine image in the two-chamber view (temporal resolution 7.5ms). Three radiologists independently assessed the image quality on nine branches of the coronary artery through a four-point scale (1=poor, 2=medium, 3=good, 4=excellent) subjective score system. The scored coronary artery included left main coronary artery (LM),left anterior descending coronary (LAD), left circumflex artery (LCX),posterior descending artery (RCA) at proximal (index 1), middle/distal (index 2), distal (index 3) positions.After the consistency test, the mean values of image quality scores were compared between two groups using anMann-Whitney UtestResults
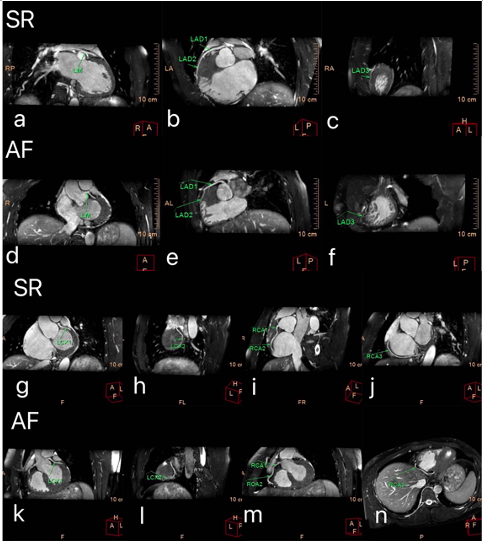
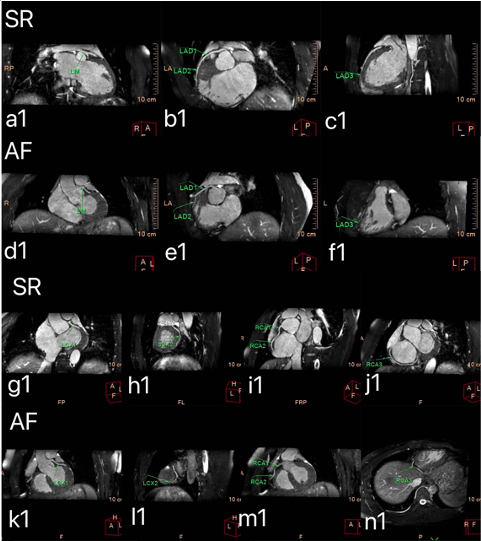
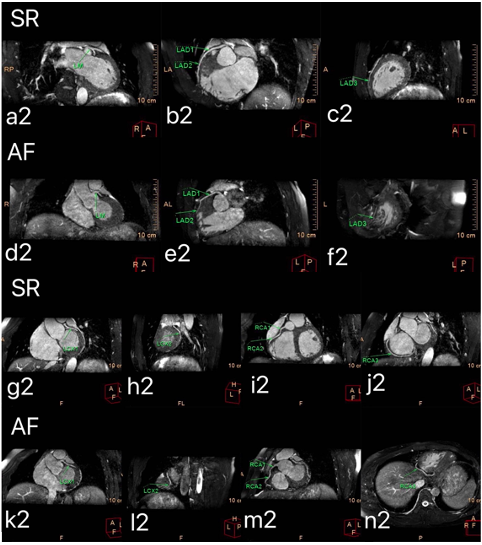
The representative images of the right coronary artery and left coronary artery with different acceleration schemes were shown in figure 1, figure 2, and figure 3. The quality scores of images with CS AFs of 2,4were in table1and table2.There was no statistical difference in image quality inLM, LAD1, LAD2, LAD3,LCX1,LCX2,RCA1,RCA3(p >0.05) except RCA2(p<0.05). The image quality scores with CS AFs of 6 were in table3, There were no statistical differences in image quality in LM, LAD1, LAD2, LAD3,LCX1,LCX2,RCA1,RCA2(p>0.05), and slight differences in image quality in RCA3(p <0.05).When the CS AFs increased, the image quality was reduced(table1,2,3).Discussion
Despite the arrhythmia in patients with atrial fibrillation, there was little difference in image quality compared with sinus rhythm except for a few vessels.This suggested that whole-heart coronary MRA with CS technique was also suitable for atrial fibrillation patients. Further studies are necessary to evaluate its diagnostic accuracy compared with the gold standard digital subtraction angiography (DSA).Conclusion
This study showed that whole-heart coronary MRA with different CS AFs in sinus rhythm and atrial fibrillation patients could get approximately the same image quality, which suggested CS accelerated coronary MRA was a promising and valuable non-invasive clinical method for the diagnosis of coronary artery disease.Acknowledgements
On this occasion, there is no one we wish to acknowledge.References
1. Saeed M,Van TA,Krug R,et al.Cardiac MR imaging:current status and future direction[J].Cardiovase Diagn Ther,2015,5(4):290-310.
2. Kim KW,Lee JM,Jeon YS,et al.Free-breathing dynamic contrast-enhancedMRI of the abdomen and chest using a radial gradient echo sequence with K-space weighted image contrast (KWIC)[J].EurRadial,2013,23:1352-1360.
3.Weber OM,Martin AJ,Higgins CB,et al.Whole-heart steady-state free precession coronary artery magnetic resonance angiography.Magn Reson Med,2003,50:1223-1228.
Figures