4146
Single-breath-hold whole heart coronary MRA using 3D turbo-field-echo-planar-imaging (TFEPI) with Compressed SENSE framework
Kazuo Kodaira1, Michinobu Nagao2, Masami Yoneyama3, Mana Kato1, Takumi Ogawa1, Yutaka Hamatani1, Isao Shiina1, Yasuhiro Goto1, and Shuji Sakai2
1Department of Radiological Services, Tokyo Woman's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Woman's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
1Department of Radiological Services, Tokyo Woman's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Woman's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
Conventional whole-heart-coronary-magnetic-resonance-angiography (WHC-MRA) using NAV has a limitation of long scan time. Single-breath-hold-multi-shot-gradient-EPI can significantly reduce scan time of WHC-MRA, but it may be difficult depending on the gradient-spec of MRI-system. 3D-turbo-field-echo-planar-imaging (TFEPI) with Compressed-SENSE (C-SENSE) has the possibility to solve these problems. However, it is yet not applied for WHC-MRA. C-SENSE is suitable for subjects with a high sparse such as vessels, and can accelerate scan time of WHC-MRA while ensuring image quality. We propose a new combination of TFEPI with C-SENSE for single-breath-hold WHC-MRA, and examine image quality and scan time in comparison to the conventional methods.
Introduction
Various sequences have been proposed for whole heart coronary magnetic resonance angiography (WHC-MRA)1-4. In conventional WHC-MRA, it is typically performed during free-breathing, and respiratory motion is prospectively compensated by using a 1D-right-diaphragmatic-navigator (NAV)5. However, an important limitation of the NAV method is its relatively long acquisition time6. Single-breath-hold technique using Turbo-field-echo-planar-imaging (TFEPI) could significantly reduce the acquisition time of WHC-MRA while providing image quality similar to that of conventional free-breathing gradient echo sequence7. TFEPI sequence is a hybrid technique that combines TFE and EPI scan7 (Fig.1). It enables high-speed imaging with EPI readout, resulting in shorter scan time by allowing more echoes to be acquired during one heartbeat. However, there is a problem that scan time is extended depending on the gradient-spec of MRI-system. On the other hand, even if SENSE-factor is increased to shorten scan time, image quality is expected to degrade due to increased noise. 3D TFEPI with Compressed SENSE (C-SENSE) has the possibility to solve these problems. C-SENSE has recently been introduced as acceleration technique. By combining TFEPI with C-SENSE (CS-TFEPI), we hypothesized that scan time of single-breath-hold WHC-MRA can be further accelerated without degrading the image quality by denoising. In this study, we investigated the feasibility of single-breath-hold CS-TFEPI for WHC-MRA by comparing with single-breath-hold TFEPI with SENSE and conventional free-breathing TFE.Methods
A total of six volunteers (5 males and 1 female; age range: 23~44) were examined on a 3.0T-MRI (Ingenia, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. We compared image quality and scan time among WHC-MRA using CS-TFEPI or SENSE, and TFE. Four sequences were acquired with cardiac triggering. For respiratory compensation, TFEPI was acquired with single-breath-hold and TFE was acquired with NAV. Imaging-parameters; TFEPI: FOV=300×282mm2, voxel-size=1.56×1.93×3.6mm3, TR/TE/FA=9.3/4.3/20, TFE-factor=17, EPI-factor=7, shot-duration=158.7ms, SENSE/C-SENSE factor=SENSE:2.5×1.5 (TFEPI-S2.5×1.5) /SENSE:3.6×2.0 (TFEPI-S3.6×2.0) /C-SENSE:3.6×2.0 (TFEPI-CS3.6×2.0); TFE: FOV=300×288mm2, voxel-size=1.6×1.6×1.8mm3, TR/TE/FA=3.2/1.39/12, TFE-factor=31, shot-duration=100ms, SENSE-factor=2.0×1.2 (T1TFE-S2.0×1.2). Each actual scan time was recorded. Curved Planer Reconstructions (CPRs) were performed using Ziostation2 (Ziosoft Co, Tokyo) and image quality was evaluated by visual score at the 10-points (RCA: #1/2/3/4 LAD: #5/6/7/8 CX: #11/13) based on American-Heart-Association classification. For overall image quality, sharpness and noise and artifacts, we evaluated them as 4-point grades (grade “4” was excellent, “1” was severe) by two blinded readers. Visual evaluation was assessed by Steel-Dwass test. For quantitative comparison, signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were measured. The SNR was assessed in the blood and myocardium. To allow quantitative SNR measurements, we used a noise-measurement-method proposed by Zwanenburg et al8. The standard-deviation of a region of interest of the corresponding area in the noise image was used as metric for the noise. SNRblood and SNRmyocardium were then calculated as follows: SNRA = SI(A) / SDnoise(A) Where SI are the mean average signal intensity of the blood and myocardium respectively, and the corresponding SDnoise is the standard-deviation at the same location on the noise images. Subsequently, we measured the CNR for comparing image contrast quantitatively. The CNR was estimated for blood and myocardium (CNRblood-myocardium). The CNRblood-myocardium was calculated by the following equations: CNRA-B = [SI(A) - SI(B)] / 0.5 [SDnoise(A) + SDnoise(B)] The SNR and CNR were assessed by one-way repeated measures analysis of variance (ANOVA) and the post-hoc Tukey-Kramer test.Results
Figure 2, 3 shows the results of visual evaluation. Regarding proximal coronary arteries, for overall image quality and noise and artifacts, TFEPI-CS3.6×2.0 and T1TFE-S2.0×1.2 were showed significantly higher than TFEPI-S3.6×2.0 and TFEPI-S2.5×1.5 (p<0.0001). In addition, there was no significant difference between TFEPI-CS3.6×2.0 and T1TFE-S2.0×1.2. For the sharpness, TFEPI-CS3.6×2.0 was showed significantly lower than T1TFE-S2.0×1.2 (p<0.0001), but significantly higher than TFEPI-S3.6×2.0 and TFEPI-S2.5×1.5 (p<0.0001). Regarding distal coronary arteries, for overall image quality, sharpness and noise and artifacts, TFEPI-CS3.6×2.0 was showed significantly lower than T1TFE-S2.0×1.2 (p<0.0001), but significantly higher than TFEPI-S3.6×2.0 and TFEPI-S2.5×1.5 (p<0.001). Figure 4 shows SNR and CNR comparison among four sequences. For the SNRblood, SNRmyocardium and CNRblood-myocardium, TFEPI-CS3.6×2.0 was showed significantly higher than T1TFE-S2.0×1.2 and TFEPI-S3.6×2.0 (p<0.0001), except for the comparison with TFEPI-S2.5×1.5. Figure 5 shows the representative images and average scan time using TFEPI-S2.5×1.5, TFEPI-S3.6×2.0, TFEPI-CS3.6×2.0 and T1TFE-S2.0×1.2.Discussion & Conclusion
TFEPI-S2.5×1.5 had a low visual score due to artifacts caused by relatively long breath holding time, and TFEPI-S3.6×2.0 had a low visual score due to increased noise with high SENSE factor. On the other hand, TFEPI-CS3.6×2.0 had high visual score regarding proximal coronary arteries as a result of high SNR and CNR due to the effect of denoising. Regarding distal coronary arteries, TFEPI-CS3.6×2.0 had low visual score due to its low spatial resolution and relatively long shot-duration time. Nevertheless, coronary MRA is often acquired after contrast-enhancement. By using contrast agent, the diagnostic ability of the distal coronary arteries can be improved by increasing the blood SNR. Thus, CS-TFEPI has clinically usefulness because it provides useful information with short breath holding time of about 20 seconds and also reduces the burden on the patient. Furthermore, 4D-coronary-MRA using 3D TFEPI has been introduced9, but it takes a long scan time for whole heart acquisition. This study suggests that CS-TFEPI can be extended to whole-heart 4D-coronary-MRA.Acknowledgements
No acknowledgements found.References
(1) Kazuo Kodaira, et al. Whole heart coronary MRA using image-based 2D navigator (iNav) and conventional Nav system: comparison of image quality and scan time. Proceedings of the Annual Meeting & Exhibition of ISMRM (2021). (2) Oliver M. Weber, PhD et al. Free-Breathing, Three-Dimensional Coronary Artery Magnetic Resonance Angiography: Comparison of Sequences. Journal of Magenetic Resonance Imaging. 2004; 20: 395-402. (3) Teresa Correia et al. Technical note: Accelerated nonrigid motion-compensated isotropic 3D coronary MR angiography. Med Phys. 2018 Jan; 45(1): 214-222. (4) Yuji Iyama et al. Single-breath-hold whole-heart coronary MRA in healthy volunteers at 3.0-T MRI. Springerplus. 2014; 3: 667. (5) Markus Henningsson et al. Prospaective Respiratory Motion Correction for Coronary MR Angiography Using a 2D Image Navigator. Magn Reson Med. 2013; 69: 486-494. (6) Mehdi H. Monghari et al. Three-dimensional Heart Locator and Compressed Sensing for Whole-heart Magnetic Resonance Angiography. Magn Reson Med. 2016 May; 75(5): 2086–2093. (7) Yuji Iyama et al. Single-Breath-Hold Whole-heart Unenhanced Coronary MRA Using Multi-shot Gradient Echo EPI at 3T: Comparison with Free-breathing Turbo-field-echo Coronary MRA on Healthy Volunteers. Magn Reson Med Sci. 2018; 17: 161-167. (8) Zwanenburg et al. MR Angiography of the cerebral perforating arteries with magnetization prepared anatomical reference at 7T: comparison with time-of-flight. J Magn Reson Imaging. 2008; 28: 1519–1526. (9) Yasuhiro Goto, et al. Feasibility of Non-contrast dynamic TFEPI 4D-coronary MRA with PPU. Proceedings of the Annual Meeting & Exhibition of ISMRM (2021).Figures
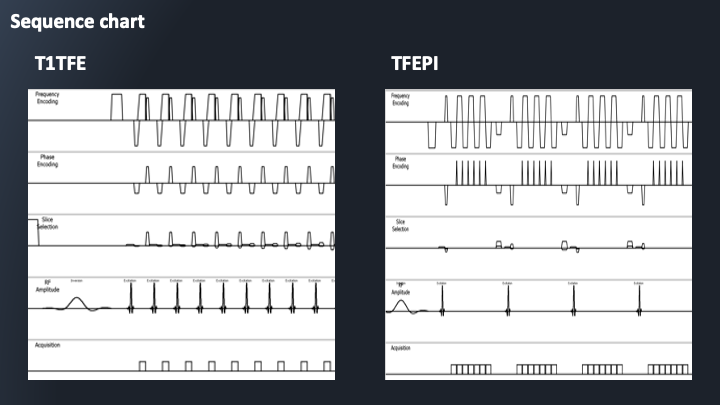
Figure 1: Sequence chart of T1TFE
and TFEPI. TFEPI sequence is a hybrid
technique that combines TFE and EPI scan. EPI readout reduce scan time by
allowing more echoes to be acquired during one heartbeat.

Figure 2: The results of visual evaluation regarding
proximal coronary arteries. For overall image quality and noise and
artifacts, TFEPI-CS3.6×2.0 and T1TFE-S2.0×1.2
were showed significantly
higher than TFEPI-S3.6×2.0 and TFEPI-S2.5×1.5 (p<0.0001). In addition, there was no significant
difference between TFEPI-CS3.6×2.0 and T1TFE-S2.0×1.2.
For
the sharpness, TFEPI-CS3.6×2.0 was showed significantly lower
than T1TFE-S2.0×1.2 (p<0.0001),
but significantly higher
than TFEPI-S3.6×2.0 and TFEPI-S2.5×1.5 (p<0.0001).
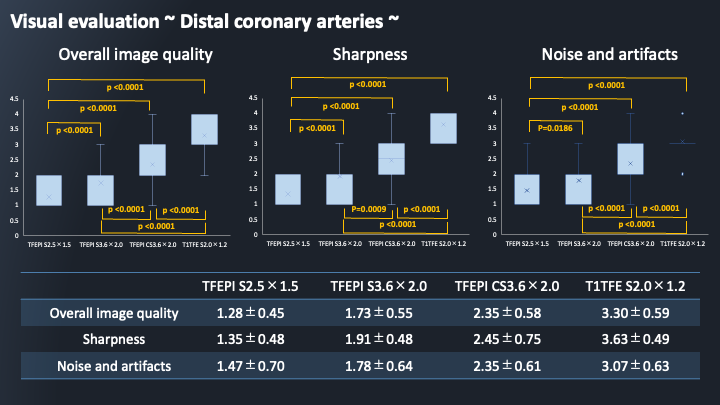
Figure 3: The results of visual evaluation regarding distal coronary arteries. For
overall image quality, sharpness and noise and artifacts, TFEPI-CS3.6×2.0 was showed significantly lower
than T1TFE-S2.0×1.2 (p<0.0001),
but significantly higher
than TFEPI-S3.6×2.0 and TFEPI-S2.5×1.5 (p<0.001).
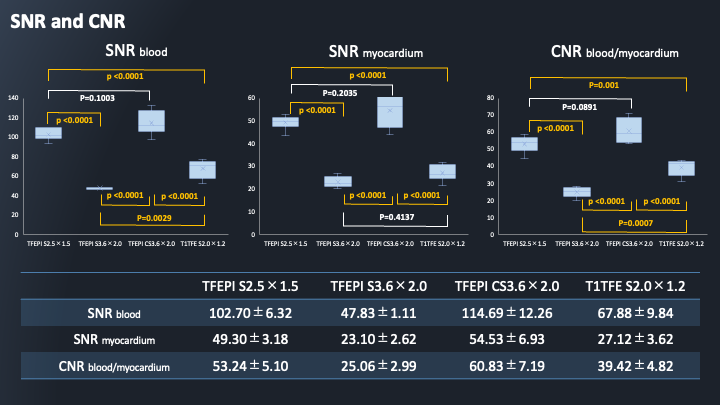
Figure 4: The results of
SNR and CNR. For the SNRblood, SNRmyocardium and CNRblood-myocardium, TFEPI-CS3.6×2.0 was showed significantly higher
than T1TFE-S2.0×1.2 and TFEPI-S3.6×2.0 (p<0.0001), except for the comparison
with TFEPI-S2.5×1.5.

Figure 5: CPR images of coronary artery of volunteer A
and average scan time in single-breath-hold TFEPI and free-breathing T1TFE. Compared
to TFEPI with SENSE, TFEPI with C-SENSE has
high SNR of blood and can visualize coronary arteries relatively distally.
DOI: https://doi.org/10.58530/2022/4146