4142
0.2 mm Isotropic Intracranial Perforating Arteries Imaging using Compressed Sensing TOF-MRA at 7T1Tiantan Neuroimaging Center of Excellence, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2China National Clinical Research Center for Neurological Diseases, Beijing, China, 3MR Collaboration, Siemens Healthineers Ltd., Beijing, China, 4Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
Synopsis
The impairment of microvessels can lead to neurologic diseases such as stroke and vascular dementia. The imaging of perforating arteries requires an extremely high resolution due to their small caliber size. In this study, we optimized the parameters of compressed sensing (CS) TOF-MRA to achieve isotropic 0.2 mm lenticulostriate artery (LSA) images within 10 minutes at 7T. More LSA stems and branches were delineated in CS TOF images compared with conventional TOF images. CS TOF-MRA can be a state-of-the-art method for detecting microvasculopathies of cerebral vascular diseases.
Introduction
The evaluation of perforating arteries (particularly the lenticulostriate artery, LSA) is important for the diagnosis of small vessel disease [1]. However, it is challenging to image perforating arteries because of their small caliber size (usually 50 – 400 um), which is smaller than conventional MRA resolution at 3T (usually 600 um). 7T TOF-MRA was initially demonstrated for successful visualization of LSA [2] due to the increased signal-to-noise ratio (SNR) and contrast improvement. However, high-resolution TOF-MRA usually requires a long acquisition duration [3], and it is difficult for conventional TOF-MRA to achieve extremely high resolution within a clinically acceptable time. It has already been demonstrated recently that novel compressed sensing (CS) high-acceleration technique can be implemented in TOF-MRA at 7T without deteriorating the image quality [4,5]. In these works, the imaging protocols may not be optimal for perforating arteries imaging since they focus on artery imaging at larger coverage, and there is room for optimizing the sequence parameters. This work achieved 0.2 mm isotropic LSA imaging within 10 minutes using CS TOF-MRA. The LSA images from CS TOF-MRA are also compared with conventional accelerated 0.3 mm isotropic TOF-MRA at 7T.Methods
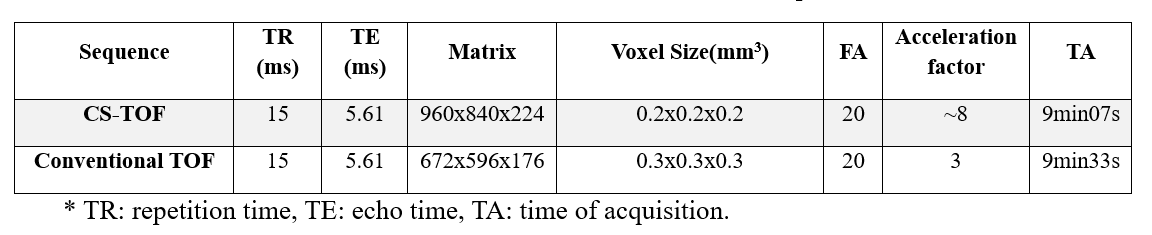
All measurements were performed on a 7 T MR system (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany) using a 32- channel Rx/8Tx head-coil (Nova Medical, Wilmington, Massachusetts, USA). Five healthy volunteers were included in this initial study. All measurements were carried out in accordance with the institutional guidelines and with the approval of the local Ethics Committee. CS TOF with 0.2 mm isotropic resolution and conventional TOF with 0.3 mm isotropic resolution were collected. Key parameters are listed in Table 1. The coronal maximum intensity projections (MIP) with a slab thickness of 20 mm were generated for both scans. The numbers of stems and branches of LSAs were counted based on these MIP images. Wilcoxon signed-rank test was used to compare the numbers of stems and branches between the two imaging methods. A p-value of less than 0.05 indicated statistical significance. All statistical analyses were performed by using commercial software (SPSS 22.0, IBM).Results
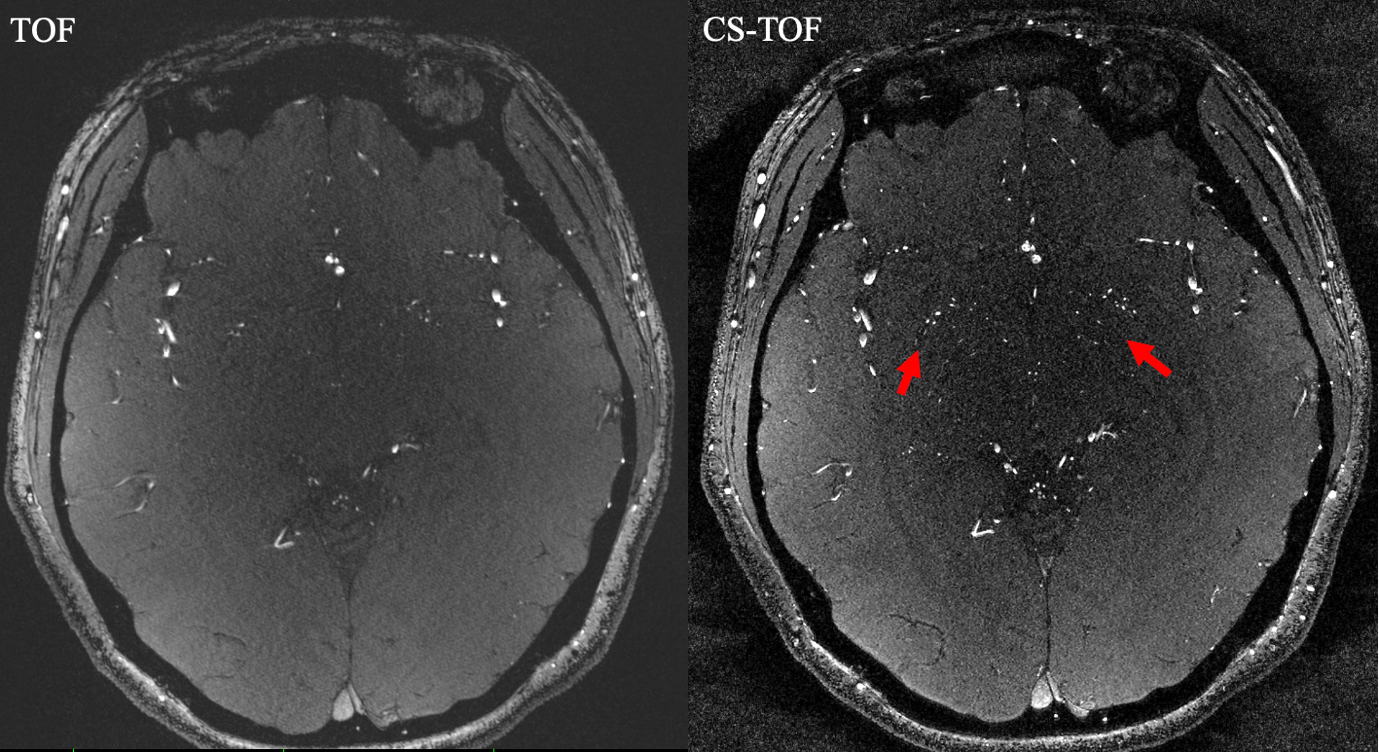
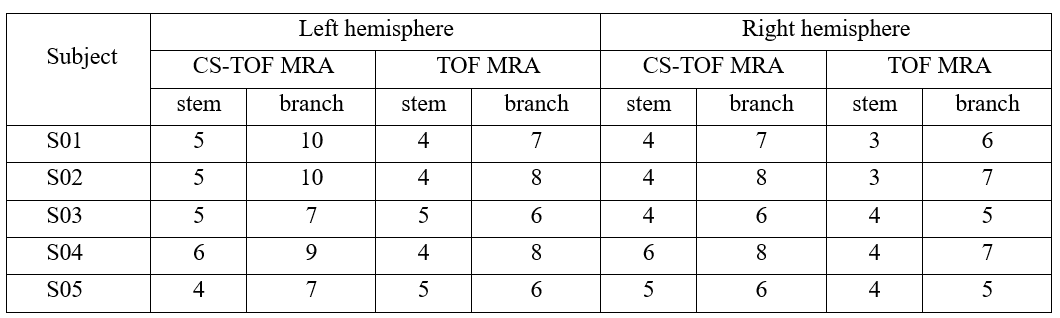
The axial images from CS TOF-MRA and conventional TOF in a volunteer are shown in Figure 1. More small arteries can be observed in CS images (red arrows). The representative MIP images from another volunteer are shown in Figure 2. CS TOF images also delineate much more LSAs, especially for branches (red arrows). The numbers of stems and branches of LSAs are listed in Table 2. The numbers of stems visualized on conventional TOF-MRA was slightly smaller than that by CS TOF-MRA (Left: 4.4±0.5 vs. 5±0.7, p = 0.257; Right: 3.6±0.5 vs. 4.6±0.9, p = 0.059). The number of branches visualized by conventional TOF-MRA was smaller than that by CS TOF-MRA, which is statistically significant in both hemispheres (Left: 7±1 vs. 8.6±1.5, p = 0.039; Right: 6±1 vs. 7±1, p = 0.025).Discussion
This might be the first time that intracranial perforating arteries imaging with isotropic 0.2 mm resolution within 10 mins has been demonstrated. A higher spatial resolution reduces the partial volume effect, so the LSA delineation is significantly improved in the CS TOF images in Figures 1 and 2. Our study demonstrates that more stems and branches were delineated in CS TOF compared with conventional TOF.In fact, the anatomy suggests that the number of LSAs is huge, but it is difficult to observe in clinics due to the limitation of SNR, resolution and subject motion. Benefitting from the improved SNR and increased T1 relaxation time, 7T TOF-MRA has been demonstrated to visualize LSAs. Still, 7T TOF-MRA may only describe the larger LSAs. The compressed sensing technique shortens the acquisition time while preserving the imaging quality due to its novel acquisition trajectory and reconstruction, thus making it possible to achieve higher resolution under the clinically acceptable acquisition time. Our results also demonstrate that more LSAs are visualized with the spatial resolution increasing from 0.3 mm to 0.2 mm. The results suggest that CS TOF can be a state-of-the-art technique for imaging LSAs. In future research, more subjects would be enrolled to verify the performance of CS TOF. Also, many quantitative metrics for LSAs, such as the length, curvature, tortuosity and stenosis, should be adopted to compare the characteristics of LSAs for the two methods. Furthermore, applications on patients with cerebral vascular diseases should also be evaluated.
Conclusion
The CS TOF-MRA was optimized to achieve isotropic 0.2 mm LSAs images within 10 mins. A higher resolution produces a detailed delineation of the intracranial perforating arteries. The technique can be state-of-the-art for the evaluation of cerebral small vessel diseases.Acknowledgements
This work was supported in part by the Capital Medical University (PYZ20092). The authors thank Patrick Liebig from Siemens Healthcare for providing the research sequence.References
1. Greenberg SM. Small Vessels, Big Problems. N. Engl. J. Med. 2006;354:1451–1453 doi: 10.1056/NEJMp068043.
2. Kang CK, Park CW, Han JY, et al. Imaging and analysis of lenticulostriate arteries using 7.0-Tesla magnetic resonance angiography. Magn. Reson. Med. 2009;61:136–144 doi: 10.1002/mrm.21786.
3. Mattern H, Sciarra A, Godenschweger F, et al. Prospective motion correction enables highest resolution time-of-flight angiography at 7T. Magn. Reson. Med. 2018;80:248–258 doi: 10.1002/mrm.27033.
4. Park C-A, Kang D, Son Y-D, Kim H-K, Kang C-K. Microvascular Imaging Using Compressed Sensing at 7T MRI: A Preliminary Study. Appl. Magn. Reson. 2015;46:1189–1197 doi: 10.1007/s00723-015-0713-0.
5. Meixner CR, Liebig P, Speier P, et al. High resolution time-of-flight MR-angiography at 7 T exploiting VERSE saturation, compressed sensing and segmentation. Magn. Reson. Imaging 2019;63:193–204 doi: https://doi.org/10.1016/j.mri.2019.08.014.
Figures