4139
Sub-aortic Complex is a Simple and Accurate Parameter to Predict Obstruction in Hypertrophic Cardiomyopathy: A CMR and Doppler Study1Department of Radiology, The First Hospital of Lanzhou University, Intelligent Imaging Medical Engineering Research Center of Gansu Province, Accurate Image Collaborative Innovation International Science and Technology Cooperation Base of Gansu Province, Radiological Clinical Medicine Research Center of Gansu Province, Lanzhou, China, 2Radiology, The First Hospital of Lanzhou University, Intelligent Imaging Medical Engineering Research Center of Gansu Province, Accurate Image Collaborative Innovation International Science and Technology Cooperation Base of Gansu Province, Radiological Clinical Medicine Research Center of Gansu Province, Lanzhou, China, 3Department of Cardiology, The first Hospital of Lanzhou University, Lanzhou, China, 4Department of Magnetic Resonance Imaging, Cardiovascular Imaging and Intervention Center, State Key Laboratory of Cardiovascular Disease,Fuwai Hospital, National Center for Cardiovascular Diseases,Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Synopsis
To investigate the “sub-aortic complex (SAC)”, a new cardiac magnetic resonance (CMR) derived parameter, for the detection and grading of left ventricular outflow tract (LVOT) obstruction in hypertrophic cardiomyopathy (HCM) patients, compared with echocardiography and CMR 2D flow.
Methods
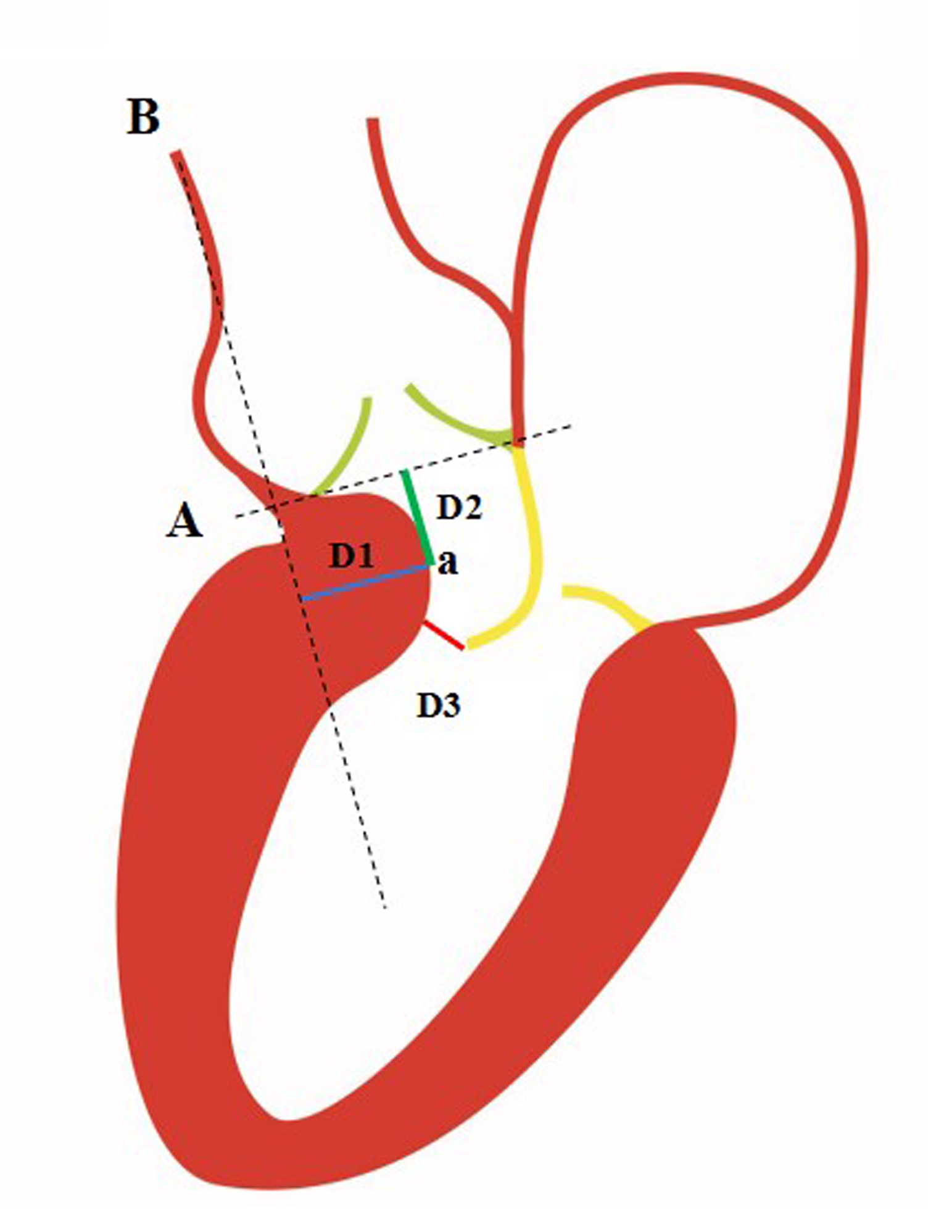
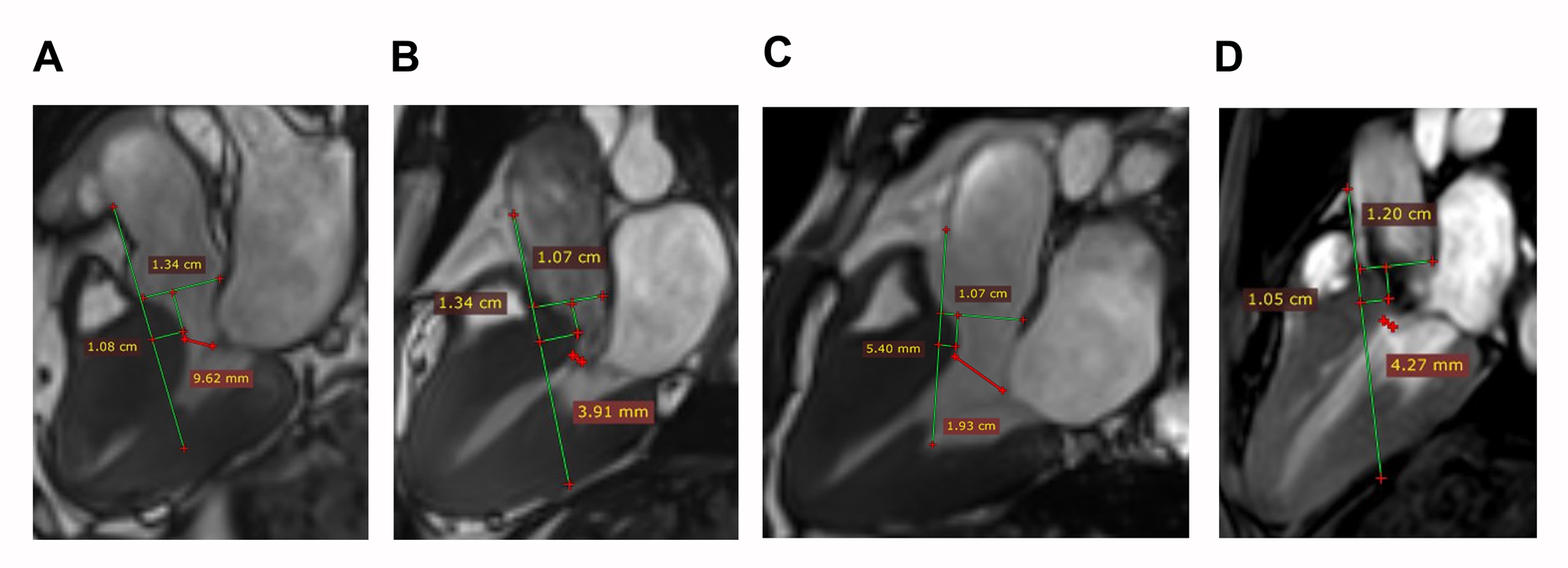
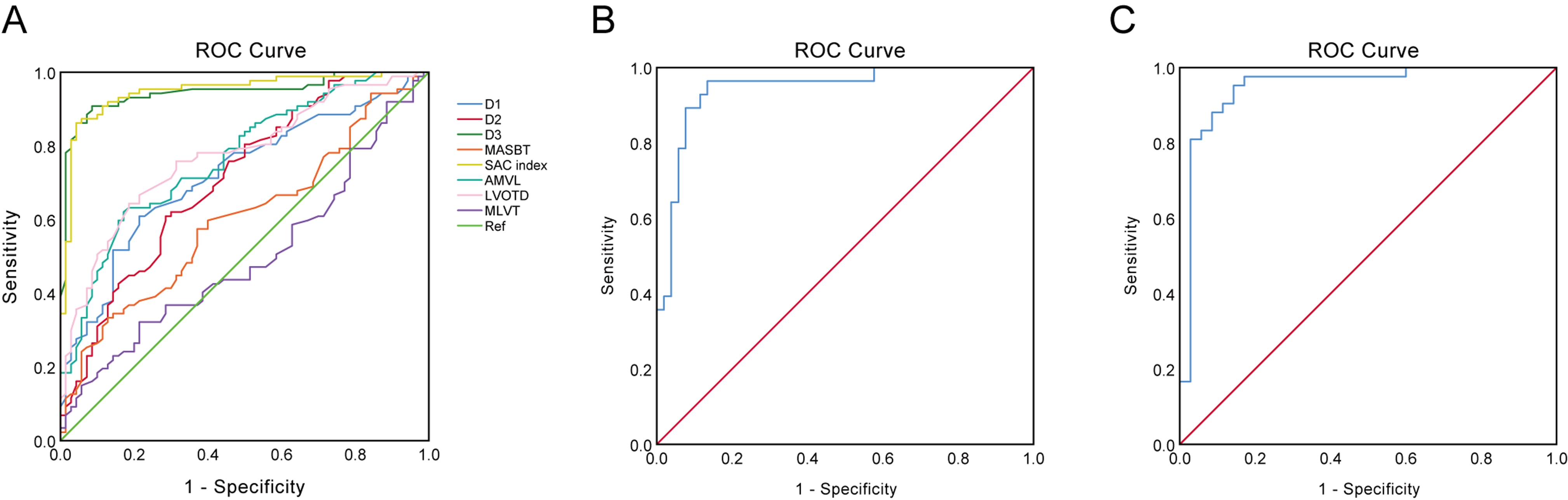
157 consecutive patients with HCM were retrospectively enrolled. The SAC parameters(D1, D2 and D3)were measured on the LV 3-chamber steady-state free precession (SSFP) cine imaging at the end-systolic phase. The relations between the existence and severity of hemodynamic obstruction and SAC index (SACi) were evaluated by Pearson correlation coefficient, receiver operating characteristic (ROC) curves and logistic regressions.Results
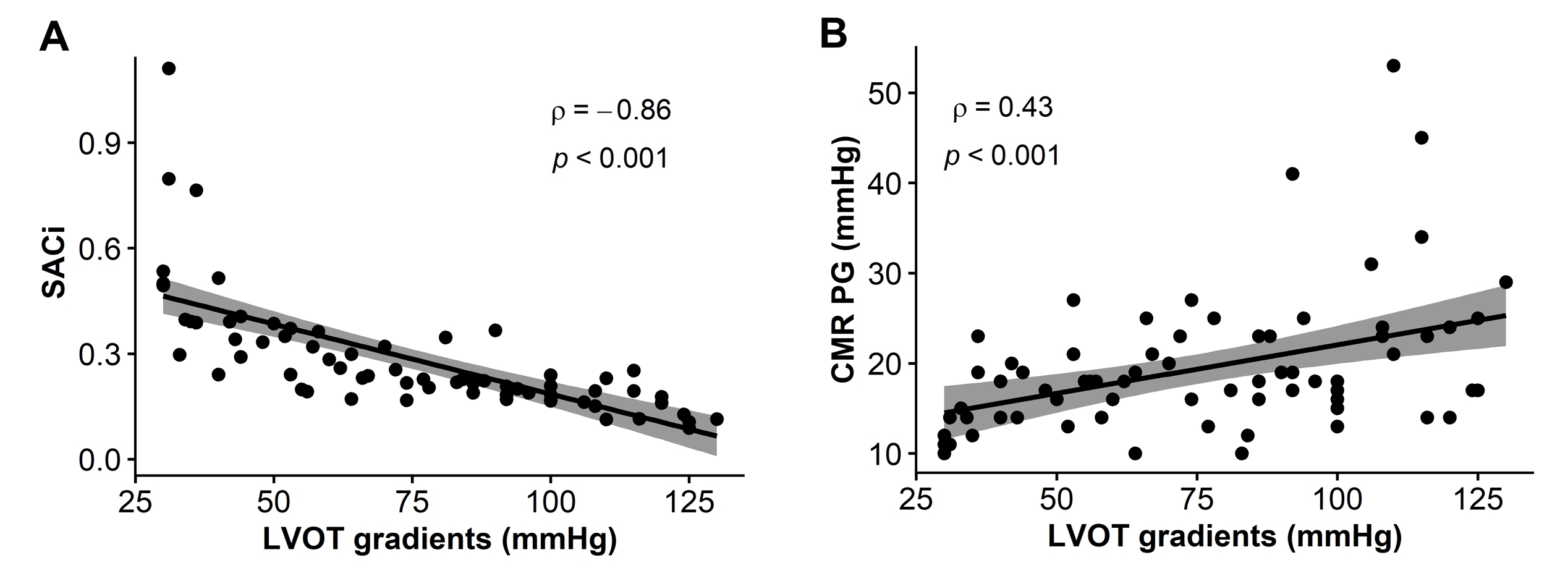
The SAC were well correlated with anterior mitral valve leaflet (AMVL) length (R=0.33, p<0.001)and LVOT diameter(R=0.48, p<0.001). The ROC curves indicated that SACi was able to discriminate the obstructive and non-obstructive patients with the best predictive accuracy (AUC=0.949, p<0.001). The cutoff value of 0.424 yielding a sensitivity and specificity of 94.3% and 87.4%, respectively. Further Spearman correlation analysis demonstrated significant inverse relationship between SACi (R=0.86 p<0.001), CMR PG (R=0.43, p<0.001 ) and the resting LVOT pressure gradient.Conclusion
The SACi is a simple and accurate parameter, which can detect LVOT obstruction. It was also better than the relatively low temporal resolution CMR 2D to detect and grade the severity of obstruction in patients with HCM.Acknowledgements
This work was also partially supported by the Division of Intramural Research, National Heart, Lung and Blood Institute, National Institutes of Health, USA.References
1.Maron BJ, Maron MS. Hypertrophic cardiomyopathy. Lancet. 2013. 381(9862): 242-55.
2.Bagnall RD, Weintraub RG, Ingles J, et al. A Prospective Study of Sudden Cardiac Death among Children and Young Adults. N Engl J Med. 2016. 374(25): 2441-52.
3.Veselka J, Anavekar NS, Charron P. Hypertrophic obstructive cardiomyopathy. Lancet. 2017. 389(10075): 1253-1267.
4.Maron MS, Olivotto I, Zenovich AG, et al. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006. 114(21): 2232-9.
5.Authors/Task Force members, Elliott PM, Anastasakis A, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014. 35(39): 2733-79.
6.To AC, Dhillon A, Desai MY. Cardiac magnetic resonance in hypertrophic cardiomyopathy. JACC Cardiovasc Imaging. 2011. 4(10): 1123-37.
7. Maron BJ, Maron MS. The Remarkable 50 Years of Imaging in HCM and How it Has Changed Diagnosis and Management: From M-Mode Echocardiography to CMR. JACC Cardiovasc Imaging. 2016. 9(7): 858-872.
8. Maron MS, Olivotto I, Harrigan C, et al. Mitral valve abnormalities identified by cardiovascular magnetic resonance represent a primary phenotypic expression of hypertrophic cardiomyopathy. Circulation. 2011. 124(1): 40-7.
9. Patel P, Dhillon A, Popovic ZB, et al. Left Ventricular Outflow Tract Obstruction in Hypertrophic Cardiomyopathy Patients Without Severe Septal Hypertrophy: Implications of Mitral Valve and Papillary Muscle Abnormalities Assessed Using Cardiac Magnetic Resonance and Echocardiography. Circ Cardiovasc Imaging. 2015. 8(7): e003132.
10.Hindieh W, Weissler-Snir A, Hammer H, Adler A, Rakowski H, Chan RH. Discrepant Measurements of Maximal Left Ventricular Wall Thickness Between Cardiac Magnetic Resonance Imaging and Echocardiography in Patients With Hypertrophic Cardiomyopathy. Circ Cardiovasc Imaging. 2017. 10(8).
11. Tan C, Rubenson D, Srivastava A, et al. Left ventricular outflow tract velocity time integral outperforms ejection fraction and Doppler-derived cardiac output for predicting outcomes in a select advanced heart failure cohort. Cardiovasc Ultrasound. 2017. 15(1): 18.
12. Schulz-Menger J, Abdel-Aty H, Busjahn A, et al. Left ventricular outflow tract planimetry by cardiovascular magnetic resonance differentiates obstructive from non-obstructive hypertrophic cardiomyopathy. J Cardiovasc Magn Reson. 2006. 8(5): 741-6.
13. Vogel-Claussen J, Santaularia Tomas M, Newatia A, et al. Cardiac MRI evaluation of hypertrophic cardiomyopathy: left ventricular outflow tract/aortic valve diameter ratio predicts severity of LVOT obstruction. J Magn Reson Imaging. 2012. 36(3): 598-603.
14. Morant K, Mikami Y, Nevis I, et al. Contribution of mitral valve leaflet length and septal wall thickness to outflow tract obstruction in patients with hypertrophic cardiomyopathy. Int J Cardiovasc Imaging. 2017. 33(8): 1201-1211.
15. Maron MS, Olivotto I, Betocchi S, et al. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med. 2003. 348(4): 295-303.
16. Desai MY, Bhonsale A, Patel P, et al. Exercise echocardiography in asymptomatic HCM: exercise capacity, and not LV outflow tract gradient predicts long-term outcomes. JACC Cardiovasc Imaging. 2014. 7(1): 26-36.
17. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986. 1(8476): 307-10.
18. Rowin EJ, Maron MS. Evidence for Left Ventricular Outflow Tract Obstruction With Minimal Septal Hypertrophy: The Case Grows Stronger for a Multimodality Imaging Strategy for Hypertrophic Cardiomyopathy. Circ Cardiovasc Imaging. 2015. 8(7): e003588.
19. Maron MS. Clinical utility of cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J Cardiovasc Magn Reson. 2012. 14: 13.
20. Gruner C, Chan RH, Crean A, et al. Significance of left ventricular apical-basal muscle bundle identified by cardiovascular magnetic resonance imaging in patients with hypertrophic cardiomyopathy. Eur Heart J. 2014. 35(39): 2706-13.
21.Henein M, Arvidsson S, Pilebro B, Backman C, Mörner S, Lindqvist P. Long mitral valve leaflets determine left ventricular outflow tract obstruction during exercise in hypertrophic cardiomyopathy. Int J Cardiol. 2016. 212: 47-53.
22.Teo EP, Teoh JG, Hung J. Mitral valve and papillary muscle abnormalities in hypertrophic obstructive cardiomyopathy. Curr Opin Cardiol. 2015. 30(5): 475-82.
Figures