4133
High resolution retinal blood flow MRI using a new acquisition strategy for MRI of curved objects
Eric R. Muir1
1Radiology, Stony Brook University, Stony Brook, NY, United States
1Radiology, Stony Brook University, Stony Brook, NY, United States
Synopsis
The retina has highly structured laminar organization, with two separate blood supplies, the retinal and the choroidal blood flow layers. Retinal MRI has generally used a single thick 2D slice. Extension to 3D retinal MRI is difficult due to the curvature of the eye and limited SNR at the needed high resolution. A new acquisition strategy for MRI of curved objects was developed, in which high-resolution is acquired perpendicular to the retina but with low-resolution tangent to the retina. This approach gave significant gains in SNR and provided laminar resolution of the retinal and choroidal blood flow in 3D.
Introduction
The retina has a highly-structured laminar neuronal and vascular organization, with two separate blood supplies with substantial differences, the retinal and the choroidal vessels. Choroidal blood flow (ChBF) is many times greater than retinal BF (RBF). Different retinal diseases likely affect the retinal and choroidal circulations differently.MRI application to the thin retina is difficult due to the high resolution needed. Retinal MRI has generally used a single thick 2D slice through the central retina, with the ability to distinguish retinal BF and choroidal BF having been demonstrated (1). The thick slice provides relatively high SNR. However, extension to 3D MRI of the retina has remained difficult. Additional thick slices could be acquired, but there will be substantial through-plane blurring due to the retina curving through non-central slices, blurring the retina too much to be useful. Thus, high resolution is also needed in the 3rd dimension (~70-80µm in all 3 dimensions for rodents), but adequately increasing the slice resolution will dramatically reduce SNR, which is already limited for 2D retinal MRI. The goal of this study was to overcome this limitation with a new acquisition strategy for MRI of curved objects with high resolution perpendicular to the surface of the object.
Methods
A curved object imaging (COI) acquisition approach was developed, in which high-resolution is acquired in radial orientations perpendicular to the curved retina, while low resolution (thus improving SNR) is acquired in orientations tangent to the retina. To do this, k-space is acquired in a wedge shape of ~90-110o, providing high laminar resolution over the majority of the retina. Several potential trajectories could be used for COI acquisition. We used a modified 3D PROPELLER readout, where the number of blades are reduced to sample a bowtie-like region of k-space (Fig 1A).MRI was performed on a 7T scanner (Bruker) with 1000mT/m gradient. COI MRI was acquired using 3D RARE to encode each blade for PROPELLER. Studies were performed on C57BL/6 mice (n=2, male) anesthetized with isoflurane. A small surface eye coil (diameter=6 mm) was used for imaging. BF MRI used continuous arterial spin labeling with a label coil placed at the heart with label duration=2.55s and post label delay=350ms (1,2). COI MRI acquired 13 blades spanning 95o of the retina, with TR=3s, effective TE=4ms, FOV=7x7x7mm, matrix for each blade=96x16x16, 8 segments per blade, and 52min scan, providing perpendicular resolution of 73µm and a minimal resolution of 345µm. For comparison, conventional Cartesian acquisition was acquired using 3D EPI with TR=3s, TE=7.1ms, FOV=6x6x3.2 mm, matrix=112x112x16, 2 in-plane segments, and 48min scan. BF was calculated in ml/g/min, and the retina was flattened to analyze the retinal and choroidal BF (1).
Results
Fig 1 shows COI of a curved sample; COI and standard Cartesian acquisitions (3D RARE with comparable parameters and istropic 3D resolution of 0.34mm) were acquired with both linear and centric phase encoding, with relative SNR’s (normalized by square root of the volume repetition time) of: linear-Cartesian=1, linear-COI=3.8, centric-Cartesian=2.0, and centric-COI=8.4. COI had about 4x gain of SNR COI relative to Cartesian while maintaining high perpendicular resolution over the 95o wedges. Fig 2 shows similar SNR studies from simulations of COI and Cartesian isotropic acquisitions, giving similar SNR gains of 3-4x for COI.Fig 3 shows 3D COI images of a mouse eye, demonstrating 3D layer-specific BF of the entire retina. For comparison, Fig 4 shows similar BF images of a mouse eye using conventional 3D Cartesian acquisition. COI showed good resolution of both the RBF and ChBF across the majority of the retina in all dimensions, while Cartesian had good laminar resolution only in the in-plane dimension and only for about two central slices. For Cartesian, in the slice direction, RBF could only be distinguished over a small central region due to the lower resolution. The retinal surface was flattened from COI data, to give en-face views of BF taken from depths corresponding to the RBF and the ChBF layers (Fig 5). Blood flow as a radial distance from the optic nerve was plotted for each retinal quadrant, showing a large drop in ChBF in the periphery, but a slow decline of RBF towards the periphery.
Discussion and Conclusion
This study demonstrates a novel approach to quantitatively image the retinal and choroidal blood flow in 3D with laminar resolution using MRI. The COI MRI method developed herein provided 3D retinal MRI with improved SNR and laminar resolution compared to conventional 3D Cartesian acquisitions. ChBF was many times larger than RBF, consistent with previous reports by 2D MRI (1) or by terminal methods (autoradiography and microspheres) in large animals (3,4). Methods to quantitatively measure retinal and choroidal BF with depth resolution and across the entire retina are lacking. Our MRI approach can provide important blood flow data that is not depth limited and is non-invasive. This method could be useful to study models of retinal disease.Acknowledgements
No acknowledgement found.References
1. Muir ER, Duong TQ. MRI of retinal and choroidal blood flow with laminar resolution. NMR Biomed 2011;24:216-223. 2. Muir ER, Shen Q, Duong TQ. Cerebral blood flow MRI in mice using the cardiac spin-labeling technique. Magn Reson Med 2008;60:744-748. 3. Sperber GO, Bill A. Blood flow and glucose consumption in the optic nerve, retina and brain: effects of high intraocular pressure. Exp Eye Res 1985;41:639-653. 4. Geijer C, Bill A. Effects of raised intraocular pressure on retinal, prelaminar, laminar, and retrolaminar optic nerve blood flow in monkeys. Invest Ophthalmol Vis Sci 1979;18:1030-1042.Figures
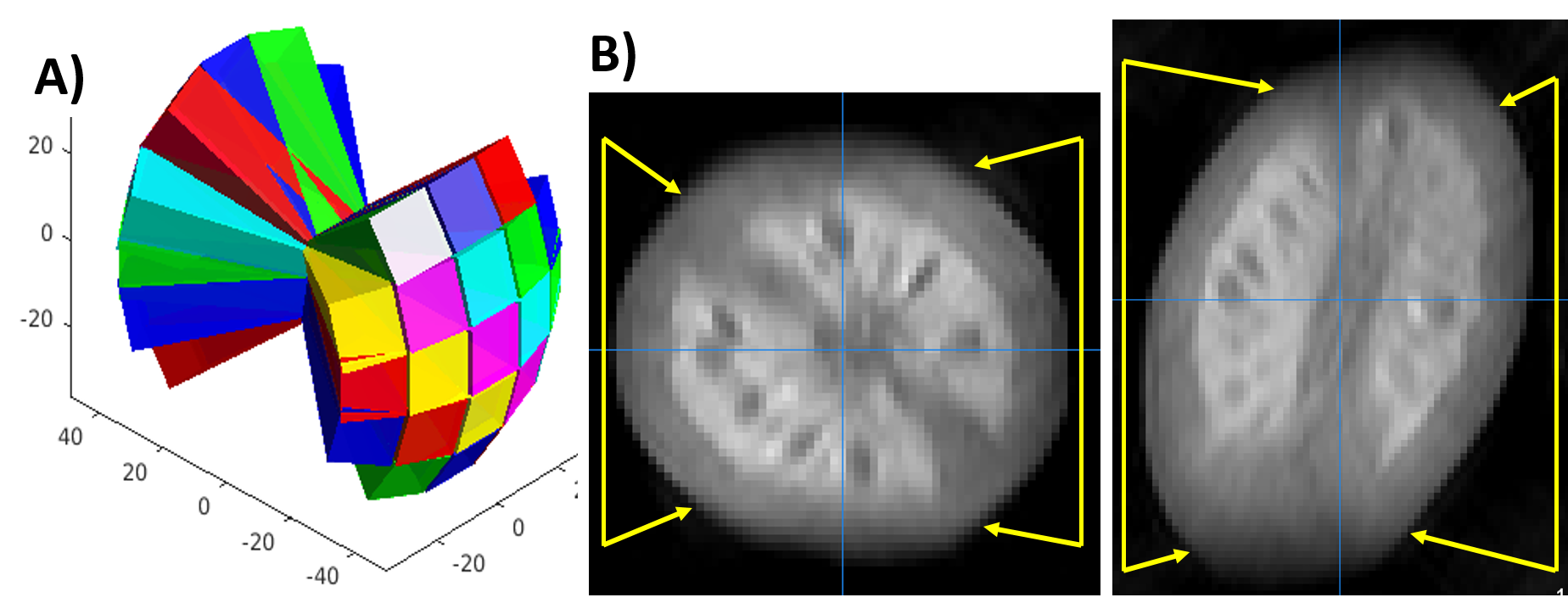
A) COI
k-space trajectory using 3D Propeller, where each rectangular slab is a 3D
phase-encoded blade. B) COI MRI of a curved sample (grape tomato), showing two
planes, with perpendicular resolution of 0.34mm, and minimal resolution of 1.63mm.
Edges are sharp in orientations in which high perpendicular resolution was
acquired (between yellow arrows), but blurred in the other orientations in which low
resolution was acquired, as expected.
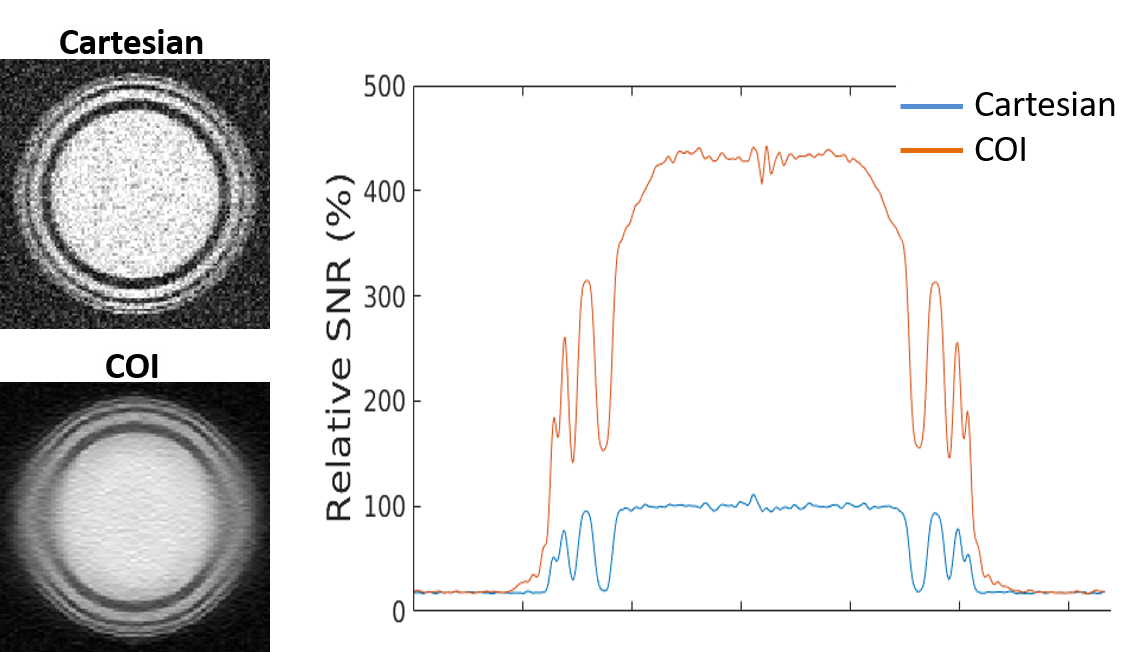
SNR
simulations of a 3D object of spherical shells. A single slice of conventional
Cartesian and COI images are shown. SNR profiles across the object are also
shown (profile taken across the “high-resolution” direction). COI had 3-4x
higher SNR, consistent with real MRI data. MRI parameters (matrix, TR, TE,
etc.) and object parameters (T2, T1, size) were set similar to those expected
for rodent retina with the COI perpendicular resolution equal to the Cartesian
isotropic resolution.
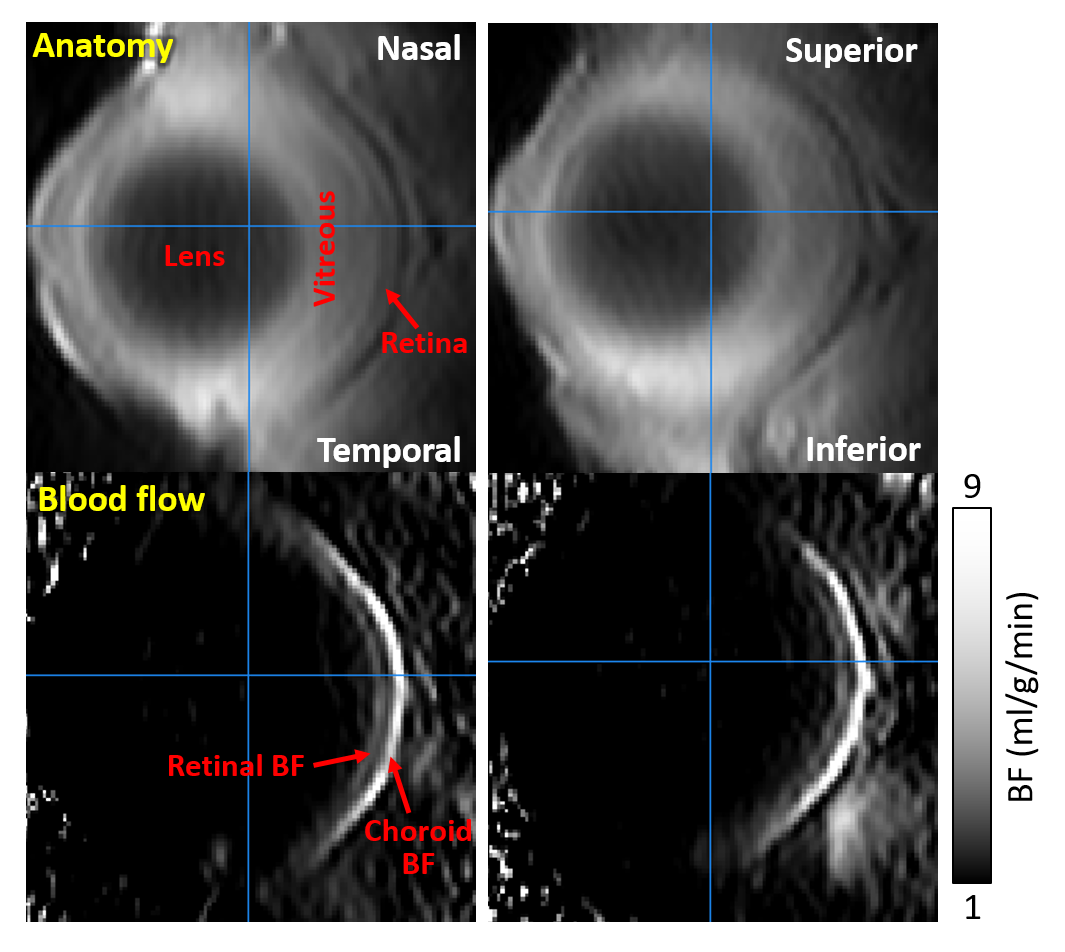
COI 3D retinal MRI of
a mouse eye showing two orthogonal planes, horizontal (left column) and vertical
(right column). The anatomical image and corresponding BF map (in ml/g/min) are
shown. Both the retinal and choroidal BF layers were clearly distinguished in
both orientations. Anatomical orientations are indicated on the anatomical
images.
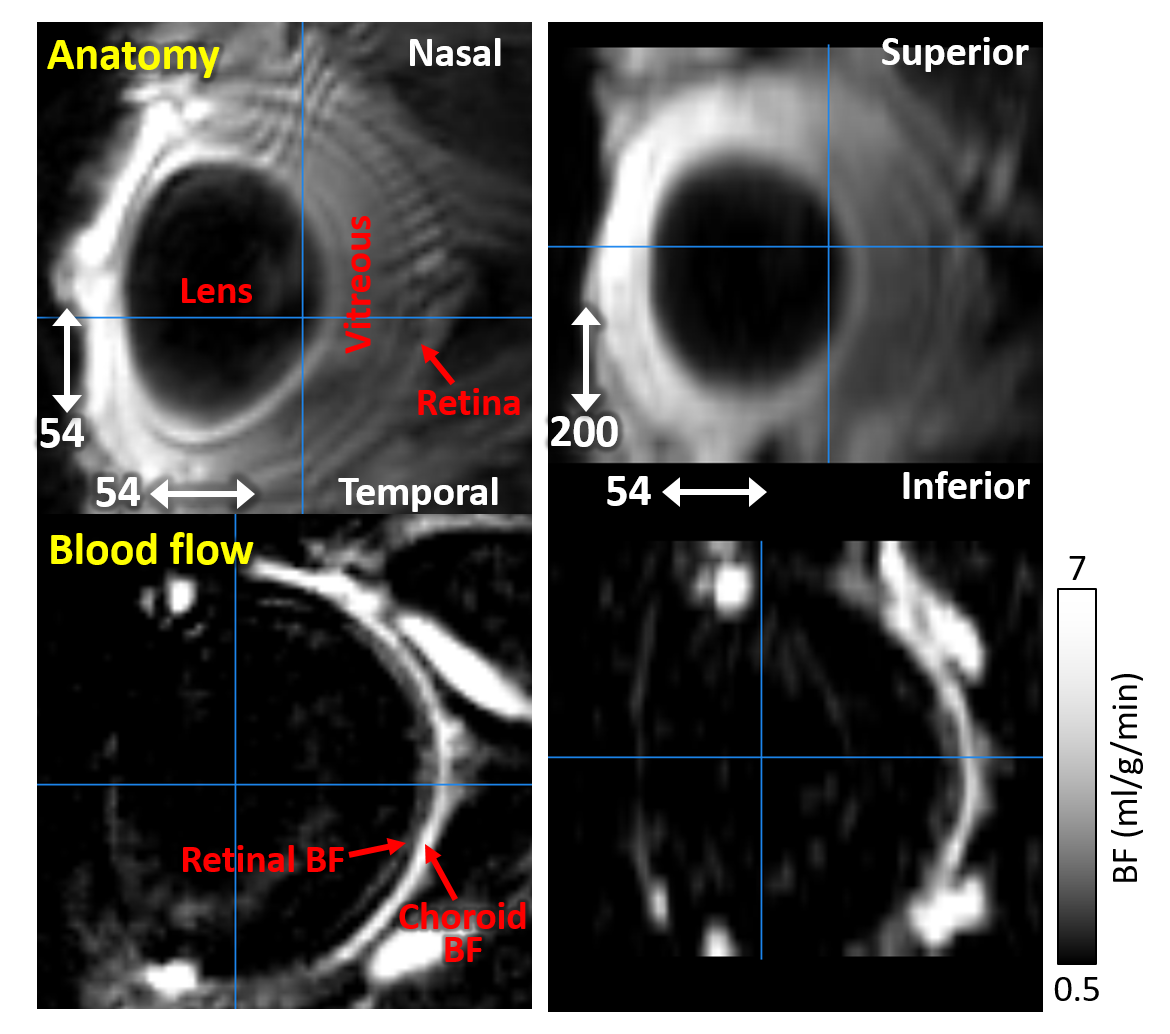
Conventional Cartesian
3D retinal MRI of a mouse eye showing two orthogonal planes, horizontal (left
column) and vertical (right column). A relatively low resolution in the slice
direction was needed to maintain adequate SNR for Cartesian acquisition, while
maintaining sufficient in-plane resolution. There was poor definition of the
retinal BF layer in the lower resolution direction. Resolutions of each direction
are indicated in the lower corner of anatomical images (in µm).
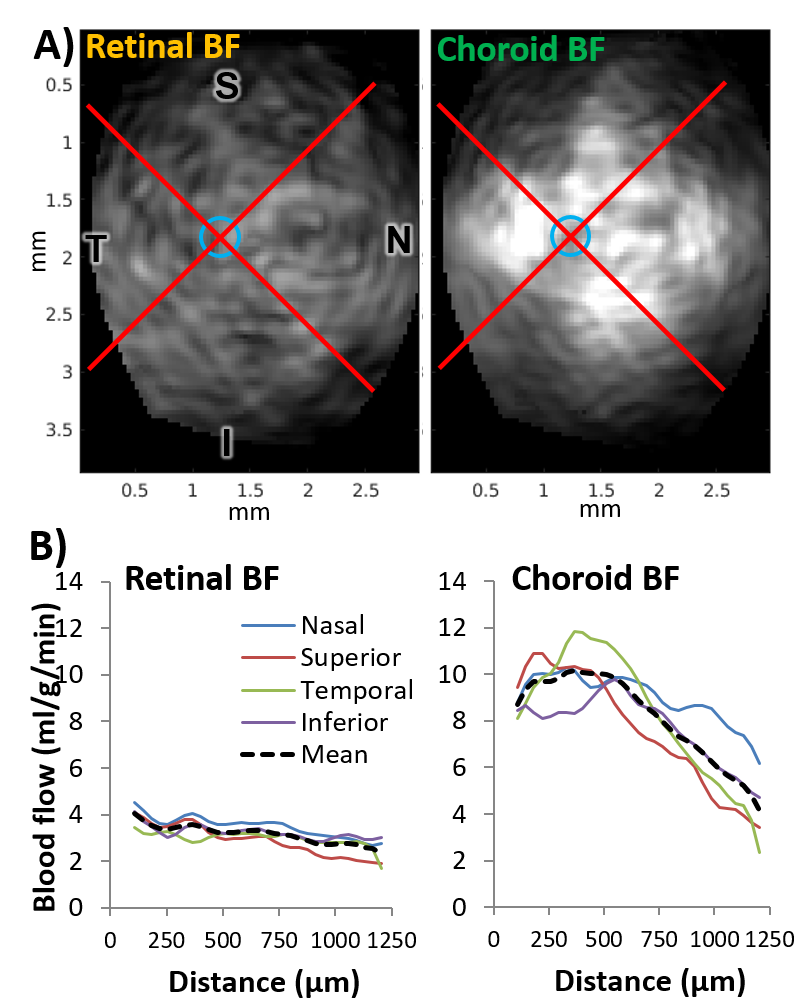
From the 3D COI BF
image in Fig 3, the retinal surface was found and virtually flattened. A) En-face
views were taken at depths corresponding to the retinal and choroidal BF layers.
Blue circle indicates optic nerve, red lines divide into quadrants (S-superior,
I-inferior, T-temporal, N-nasal). B) BF data were averaged in each quadrant and
plotted as distance from optic nerve for retinal and choroidal BF layers.
DOI: https://doi.org/10.58530/2022/4133