4131
Evaluation of Coronary Artery Damage in Kawasaki Disease with Non-Contrast Whole-Heart Coronary Magnetic Resonance Angiography1Department of Magnetic Resonance, Lanzhou University Second Hospital, Lanzhou, China, 2Philips healthcare, Xi'an, China
Synopsis
In this study, the non-contrast whole-heart coronary magnetic resonance angiography (NCE-CMRA) is used to evaluate the coronary artery damage in Kawasaki Disease (KD). The NCE-CMRA and ultrasound images of children with Kawasaki disease (KD) are retrospectively analyzed. Compared with echocardiography, the NCE-CMRA has its unique advantages in displaying coronary artery, such as high image resolution, good soft tissue contrast and strong signal to noise ratio. Furthermore, NCE-CMRA can clearly and directly show the damaged coronary artery. Therefore, it is a potential alternative to ultrasound for imaging of the coronary artery in children with KD.
Introduction
Kawasaki Disease (KD) is an acute non-specific arterial vasculitis in infants and children, which can specifically damage the coronary arteries, manifesting as coronary aneurysm, thrombosis, and stenosis, which eventually leads to myocardial infarction and even sudden death1. The accurate evaluation of coronary artery damage in children with KD has always been a major clinical problem to be solved urgently. Echocardiography has become a common examination method for the diagnosis and follow-up of coronary artery lesions in children with KD due to its economical and convenient characteristics. However, it has insufficient display for mid-to-distal and small branch coronary artery lesions, and its diagnostic value is limited2. The non-contrast whole-heart coronary magnetic resonance angiography (NCE-CMRA) is a non-invasive, contrast-free method, which is sensitive and reliable in display coronary artery dilation, coronary aneurysm formation and distal branches3. This study mainly explores the advantages of NCE-CMRA in displaying coronary arteries, and evaluates the clinical value of the diagnosis of coronary artery disease in children with KD compared with ultrasonography.Materials and Methods
The NCE-CMRA and ultrasound images of forty-one children who were clinically diagnosed with KD in Lanzhou University Second hospital from June 2017 to June 2019 were analyzed retrospectively. There were 22 males and 19 females, aged from 20 months to 10 years, with an average of 6.78 years old. The NCE-CMRA examination were collected using Philips Ingenia 3.0T scanner with 16-channel phased array body coil. 3D-TFE-NAV sequence combined with ECG gating and respiratory navigation technology were used for 3D coronary angiography. The FOV was 300x250mm2. The number of slices was 100-120, the acquisition voxel was 1.25x1.25x1.6mm3, the reconstructed voxel was 0.62x0.62x0.8 mm3, and the flip angle was 15°. Ultrasound used Philips iE33's S8-3 probe to obtain coronary artery images. Two senior cardiologists independently observed the extent, course, and distal branches of the coronary arteries displayed by the two techniques. Then the consistency test (ICC: The intraclass correlation coefficient) was performed to evaluate the inter-observer reproducibility. Finally, the chi-square test was used to analyze the significance level.Results
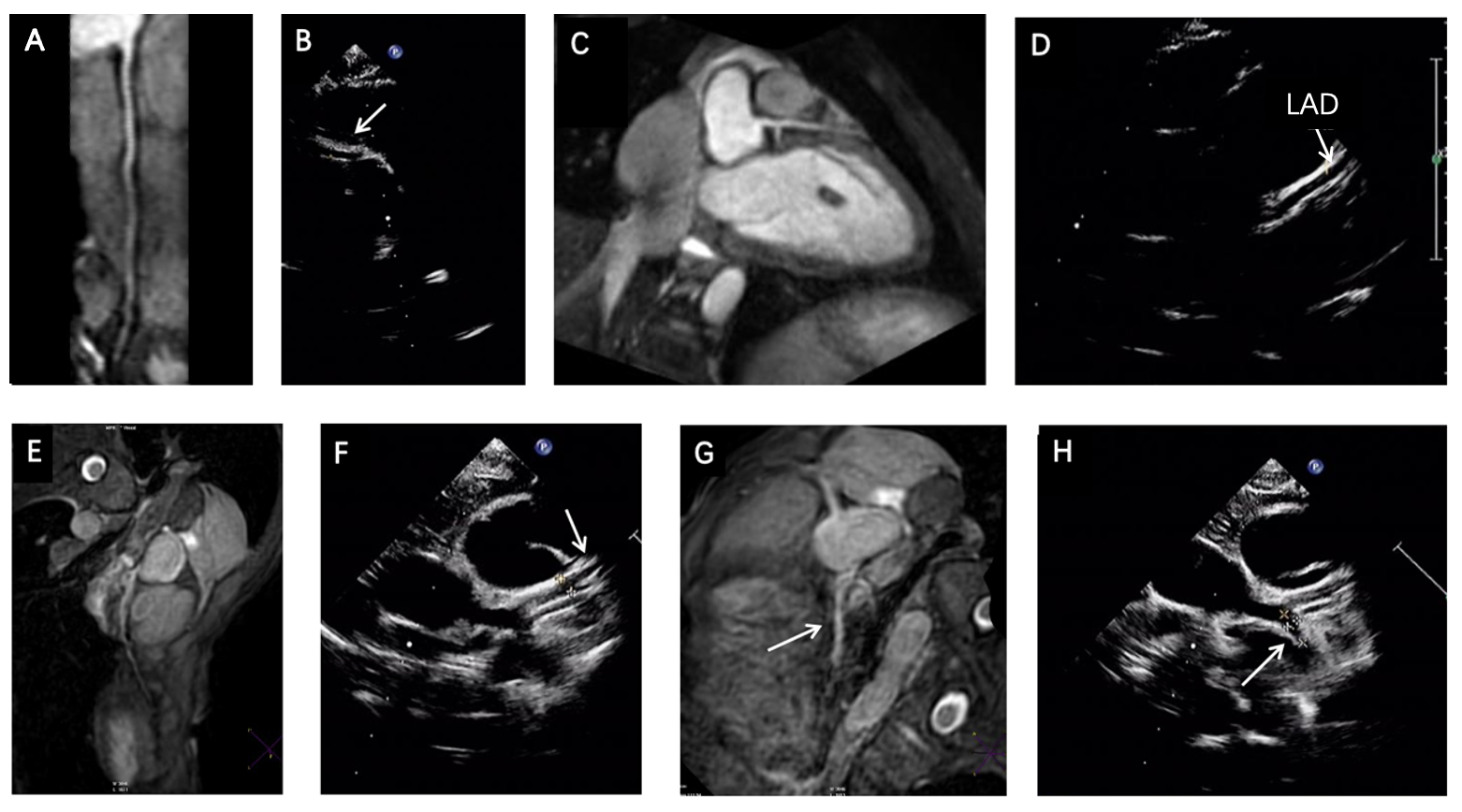
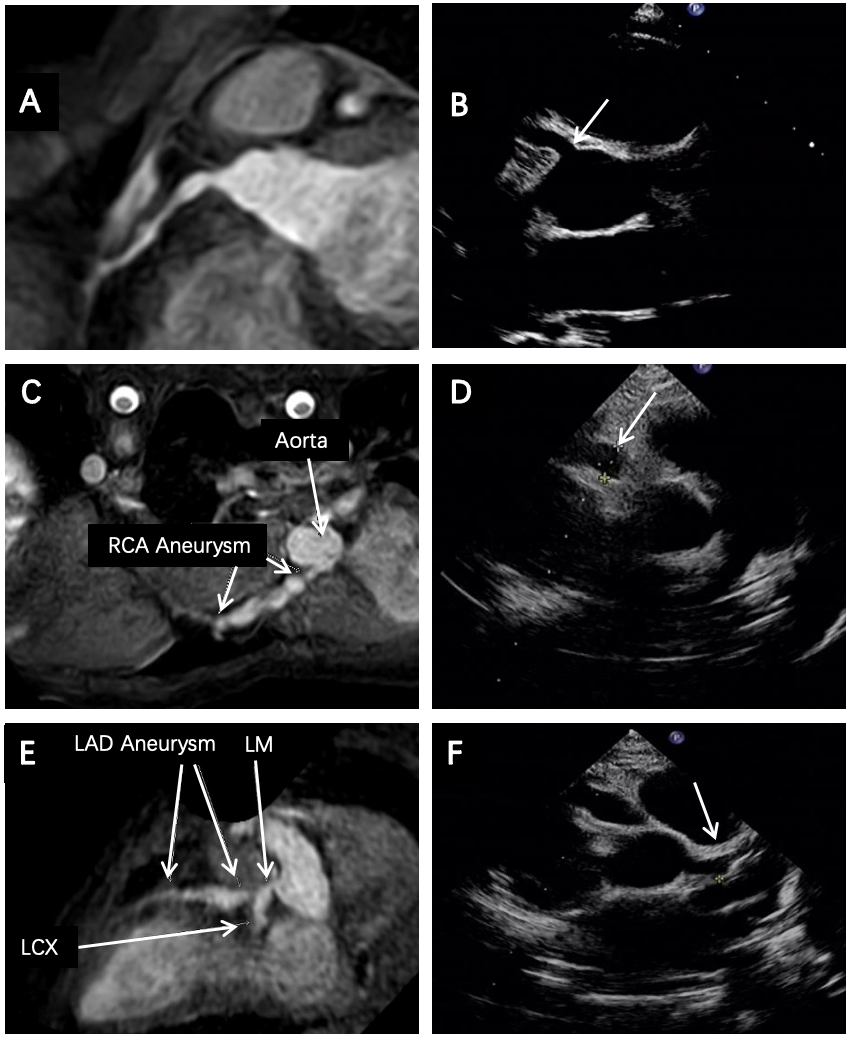
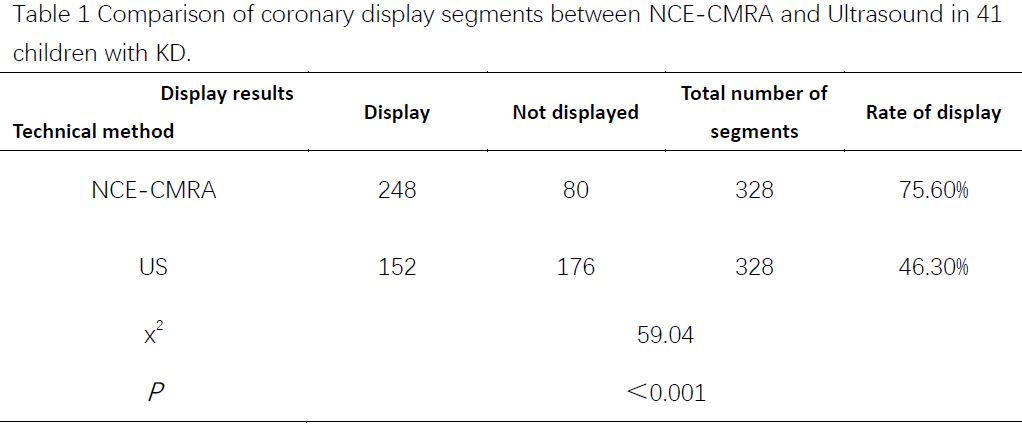
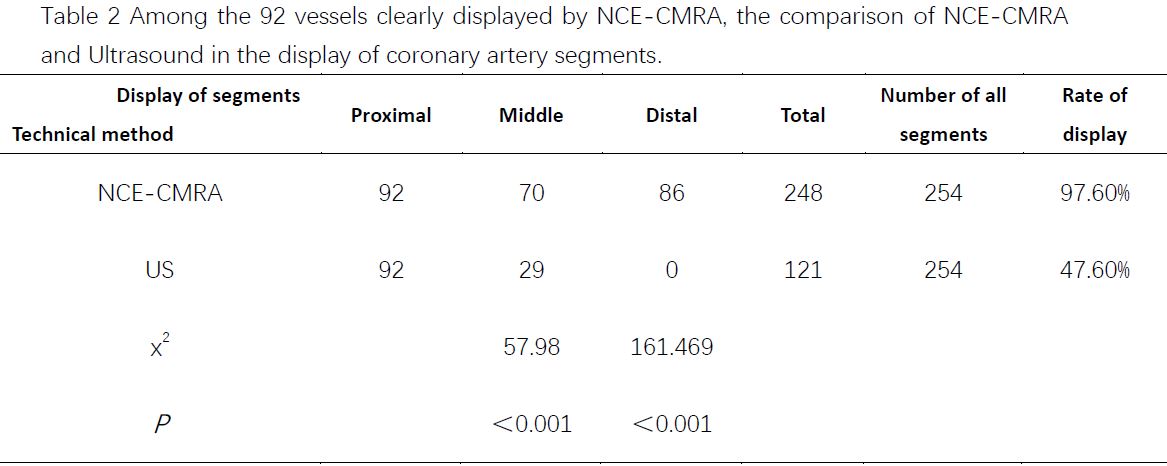
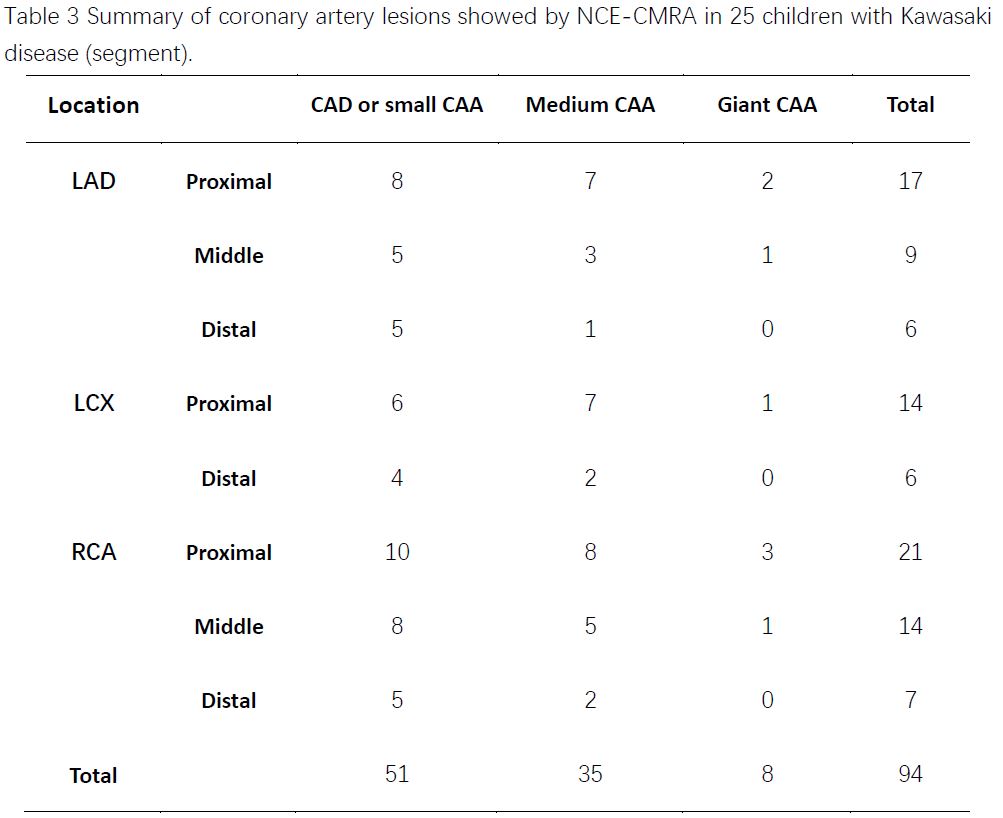
The 123 coronary branches were found in 41 children with KD. According to the American Heart Association standard3, the coronary arteries were divided into 15 segments. However, due to the individual growth differences of children, we only selected 8 segments as the classification (328 segments), which were the proximal, middle, and distal segments of the right coronary artery (RCA), the proximal, middle, and distal segments of the left anterior descending artery (LAD), and the proximal and distal segments of the left circumflex (LCX). According to NCE-CMRA image quality classification, it was divided into five levels. Level 0 and 1 cannot be diagnosed, a total of 31 vessels (74 segments) were unclearly displayed. A total of 92 vessels (254 segments) were clearly displayed. Among the 254 segments, 6 distal segments were unclearly displayed (segment display rate: 75.6%). Ultrasound showed 152 segments, and the segment display rate was 46.3%. There was significant difference between two techniques, χ2=59.04, P<0.001 (Table 1, Figure 1). For the 92 vessels (254 segments) displayed by NCE-CMRA, all the proximal and middle segments were displayed, and 86 distal vessels were displayed; while in Ultrasound images, only 29 segments in the middle and none in the distal were displayed. There was significant difference between middle and distal display (P<0.001, Table 2, Figure 1). Considered the children with KD who had coronary artery lesions, the lesions in the proximal segment of RCA, LAD, and LCX were displayed consistently (52 segments). For the middle-segment lesions, NCE-CMRA suggested 23 cases, while Ultrasound was 9 cases. NCE-CMRA displayed 19 cases of distal lesions, but Ultrasound could not (Table 3, Figure 2).Discussion
Coronary artery disease is one of the most serious complications of KD, and its severity is closely related to the prognosis of children with KD4. Compared with ultrasound, NCE-CMRA is sensitive and reliable in displaying the coronary artery range, course and distal branches. The results showed that there was no significant difference between the two techniques in the display of proximal coronary artery. However, in displaying the middle and distal branches, NCE-CMRA could intuitively and comprehensively display the course and distribution of blood vessels. Meanwhile, among 25 children with coronary artery lesions, NCE-CMRA sensitively showed the damaged vessels in the middle and distal segments, while US could not clearly detect the middle and distal vessels due to the influence of heartbeat, location, body-shape, lung and other factors, resulting in missed diagnosis of the range of coronary artery lesion in children with KD. Therefore, it is impossible to accurately evaluate the coronary artery damage in KD with NCE-CMRA. Moreover, it can be seen that NCE-CMRA is better than echocardiography in displaying the morphological abnormalities of coronary arteries, such as the expansion of the coronary arteries, the size, shape, number and location of coronary aneurysms, especially the distal coronary artery lesions5.Conclusion
NCE-CMRA can objectively and accurately display the characteristics and extent of coronary artery lesions in children with KD. It has important clinical significance in the diagnosis and evaluation of coronary artery disease in children with KD, and it can provide an effective reference for disease treatment and observation of disease changes.Acknowledgements
No acknowledgement found.References
1. Duarte R, Cisneros S, Fernandez G et al, Kawasaki disease: a review with emphasis on cardiovascular complications[J]. Insights into Imaging, 2010, 1(4): 223-231.
2. Miltner B , Poncelet A , Moniotte S . Multiple-Modality Imaging of Giant Coronary Artery Aneurysms in Kawasaki Disease[J]. Annals of Thoracic Surgery, 2016, 101(3): 1201-1201.
3. Mccrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association[J]. Circulation, 2017, 135(17): e927.
4. Dietz SM, Tacke CE, Kuipers IM et al, Cardiovascular imaging in children and adults following Kawasaki disease[J]. Insights into Imaging, 2015, 6(6): 697-705.
5. Greil GF, Seefer A, Miller S, et al. Magnetic resonance angiography and vessel wall imaging in children with Kawasaki disease[J]. Pediatr Radiol, 2007, 37: 666-673.
Figures