4130
FLEXA 3DTOF: Fast 3D TOF MR Angiography using Thin-slab Two-Point Dixon Acquisition
Naoyuki Takei1, Shiori Amemiya2, Tsuyoshi Ueyama3, Keita Fujii3, Osamu Abe2, and Tetsuya Wakayama1
1GE Healthcare, Tokyo, Japan, 2Radiology, The University of Tokyo Graduate School of Medicine, Tokyo, Japan, 3Radiology, The University of Tokyo Hospital, Tokyo, Japan
1GE Healthcare, Tokyo, Japan, 2Radiology, The University of Tokyo Graduate School of Medicine, Tokyo, Japan, 3Radiology, The University of Tokyo Hospital, Tokyo, Japan
Synopsis
Conventional 3DTOF MOTSA MRA technique without contrast agent is an established technique for carotid artery examination. The scan time is relatively long to have opportunity to improve. We have explored 3DTOF with two-point Dixon acquisition to achieve faster scan time by optimizing scan parameters and dealing with Water-Fat swap issue where B0 inhomogeneity and strong susceptibility exist at off-center scan in multi-slab acquisitions. The proposed Dixon MRA offers an alternative approach to conventional 3DTOF with about 4.2 times faster acquisition and better image contrast between artery and muscle for carotid MRA.
Introduction
Vessel occlusion arising from supra-aortic arteries is a common source of cerebral stroke and infarction1. As for non-contrast MR Angiography (MRA), conventional 3D Time of Flight (c3DTOF) has been clinically used to visualize vessels of carotid artery. The scan time is relatively long with 6-7 min to cover the whole carotid arteries, which becomes sensitive to motion such as swallowing and respiratory motion for carotid arteries and the origin of aorta, respectively. A limited imaging coverage of carotid bifurcation is scanned to accommodate clinically available scan time. The TR of c3DTOF is 20-30ms long to obtain sufficient inflow effect to move arterial blood into axial imaging slab and to apply spatial saturation pulse (SAT) pulse to suppress vein signal, which causes extended scan time. In this work, we have developed an accelerated 3DTOF MRA of two-point Dixon based acquisition with thin slab, short TR, parallel imaging, and compressed sensing technique to provide the wide scan coverage and less motion sensitivity within 2-minute scan time. The strategy for off-resonance scan in multi-slab Axial Dixon MRA is proposed to make robustness to Water and Fat swap.Methods
Figure 1.a shows the scheme of the proposed acquisition called FLEXA (FLEX Angiography) 3DTOF that consists of two-point Dixon SPGR acquisitions (FLEX3) and intermittent SATs. The axial 3DTOF acquisition uses MOTSA and concatenated SAT as is shown on Figure 1.b. The Dixon acquisition includes out-of-phase TE for the first echo and in-phase TE for the second echo in TR of 5-6ms. To mitigate flow saturation effect in slow flow, MOTSA is slab thickness 36mm with overlap 27.8 %. Total 15 slabs cover the whole carotid artery from the origin of aorta and intracranial arteries. The flip angle of the Dixon acquisition was optimized for blood flow 100 mm/s. The ramped RF pulse was used. The Dixon reconstruction uses FLEX3 to separate water (W) and fat (F) images from in-phase (IP) and out-of-phase (OP) images. A composite image is calculated by to compensate for Water-Fat swap that is the incorrect assignment of water and fat components where blood flow is subject to B0 inhomogeneity and strong susceptibility in the region such as chest region. The imaging reconstruction uses HyperSense combining ARC4 + compressed sensing5. To investigate the performance of the proposed method compared with conventional 3DTOF, healthy volunteer and patient studies were performed under the IRB approval. A 3.0 T System (Signa Premier, GE Healthcare, Waukesha, WI, U.S.A.) with Head and Neck 21 channel coils (GE Healthcare) was used. The scan parameter of FLEXA and c3DTOF is listed in Table 1.Results
Figure 2 shows a healthy volunteer scan result of carotid artery with one minute of scan time. In the MIP of the water image on the left, Water and Fat swap occurred in the left subclavian artery as indicated by the yellow arrow. In the water and fat source image of the axial slice, the water and fat signal were assigned incorrectly. The MIP of the composite image on the right compensated for the Water and Fat swap to increase the bright blood signal. Figure 3 shows a comparison result with c3DTOF in the healthy volunteer. FLEXA gave 4.2 times faster scan and higher image contrast between artery and muscle than c3DTOF. The carotid arteries were clearly depicted in both c3DTOF and FLEXA. The origin of Aorta was better delineated in FLEXA approach. Figure 4 shows a comparison result between FLEXA and c3DTOF for carotid and intracranial artery in the patient (81yo) with no pathology. FLEXA gave comparable visualization in Neck MRA to c3DTOF. For Brain MRA, the large branches of the intracranial artery were well depicted in FLEXA. Small vessels were better delineated in c3DTOF because of the capability of higher spatial resolution setting.Discussions and conclusion
The proposed method has demonstrated more than four times faster scan with comparable carotid artery delineation in equivalent spatial resolution to established 3DTOF. Accelerating scan time is clinically important to enable diagnosing vessels in the entire neck in stroke protocol. Scan time 6 seconds per slab in total 90 seconds of 15 thin slabs probably contributes to motion robustness to swallowing and breathing. To reduce signal saturation in slowly flowing blood, a thin slab and low flip angle of FLEXA were used. It takes about 5 TRs to travel through one slab at a mean velocity of 100 mm/s, a slab thickness of 36 mm, 27% slab overlap, and TR=5.7ms. As shown in Fig. 4, intracranial arteries were well delineated in FLEXA, indicating that arterial blood signal is preserved even with repeated RF excitation pulses. The use of two-point Dixon is one of the key techniques in FLEXA to achieve high background suppression, while Water-Fat swap can result in false-negative with arterial signal loss. We provided one solution with a composite image summing the magnitude of water, out-of-phase and in-phase image obtained from two-point Dixon imaging to simplify scan workflow enabling single station acquisition instead of multi-station acquisition that requires calibration scan at each station. Further clinical studies are warranted to evaluate FLEXA 3DTOF in the assessment of occlusive disease, stenosis degree and motion.Acknowledgements
No acknowledgement found.References
- Phan T, Huston J III, Bernstein MA, Riederer SJ, Brown RD Jr. Contrast-enhanced magnetic resonance angiography of the cervi- cal vessels: experience with 422 patients. Stroke 2001;32: 2282–2286.
- Irie R, Amemiya S, Ueyama T, Suzuki Y, Kamiya K, Takao H, Mori H, Abe O (2020) Accelerated acquisition of carotid MR angiography using 3D gradient-echo imaging with two-point Dixon. Neuroradiology 62(10):1345–1349.
- Ma J. Breath-hold water and fat imaging using a dual-echo two- point Dixon technique with an efficient and robust phase-correction algorithm. Magn Reson Med 2004;52:415–419.
- Brau AC, Beatty PJ, Skare S, Bammer R. Comparison of reconstruction accuracy and efficiency among autocalibrating data‐driven parallel imaging methods. Magn Reson Med 2008; 59: 382– 395.
- King et al, Proc. Intl. Soc. Mag. Reson. Med. 18
(2010), 4881.
Figures
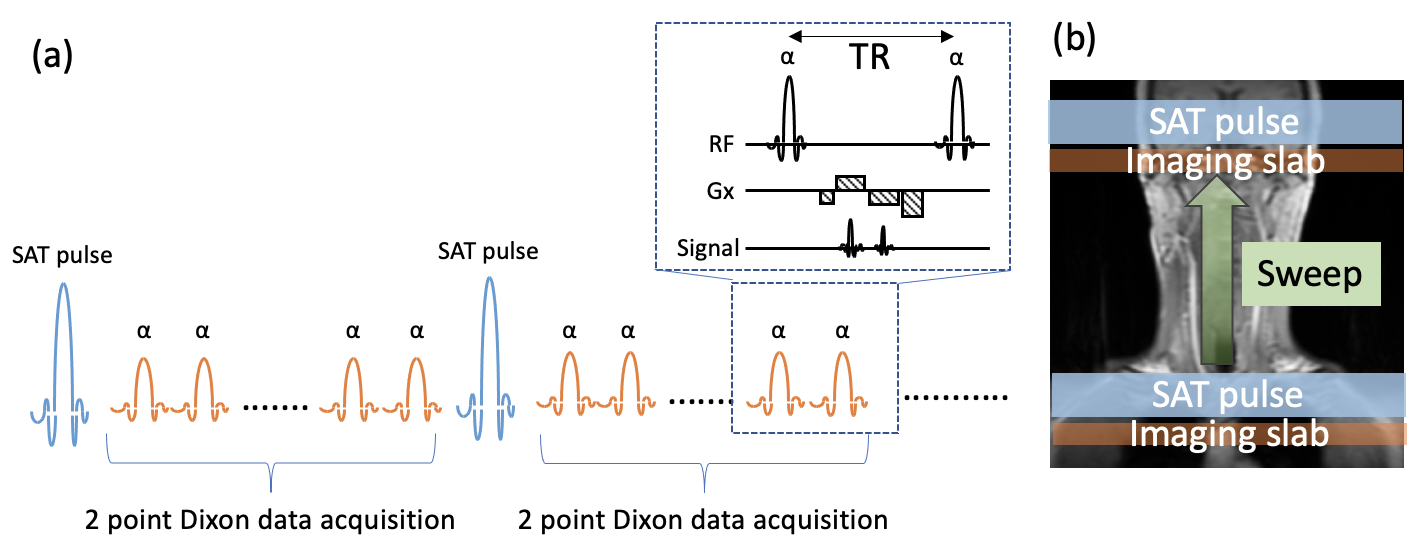
Figure.1. (a)
Proposed
non-gated two-point Dixon SPGR based MRA pulse sequence.
Intermittent SAT pulse placed on the FOV outside suppresses vein signal. (b)
Axial imaging slab with thin slab thickness sweeps through the whole cartoid
arteries.
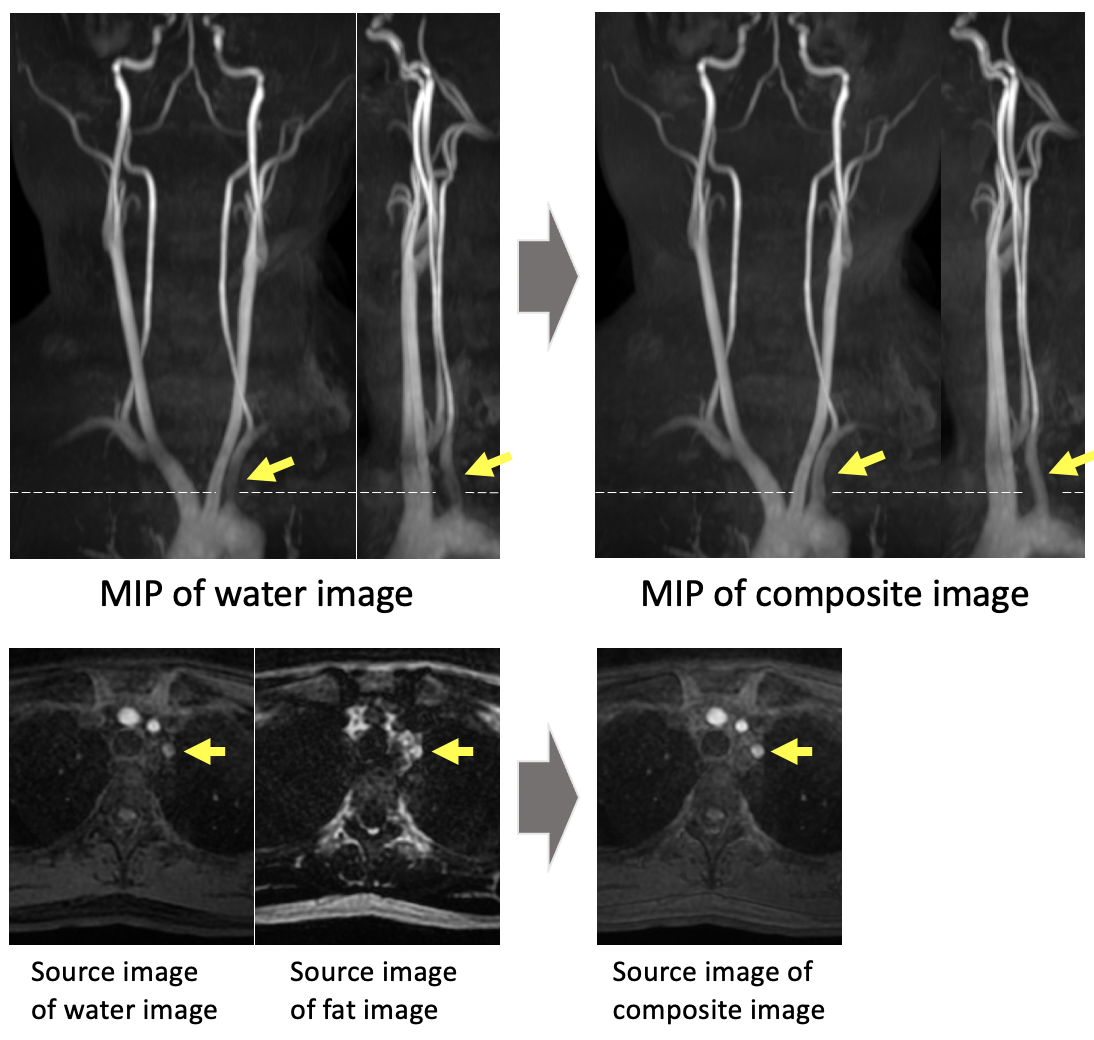
Figure.2. Water-Fat
swap compensation with composite image. MIP of water image calculated by Dixon
method has signal loss at the left subclavian artery (indicated by yellow
arrows). The source image of water and fat images identified the incorrect
assignment of water and fat signal. Composite image clearly compensates the
signal loss by adding In-Phase and Out-of-Phase images to water image. Scan
time was one minute.
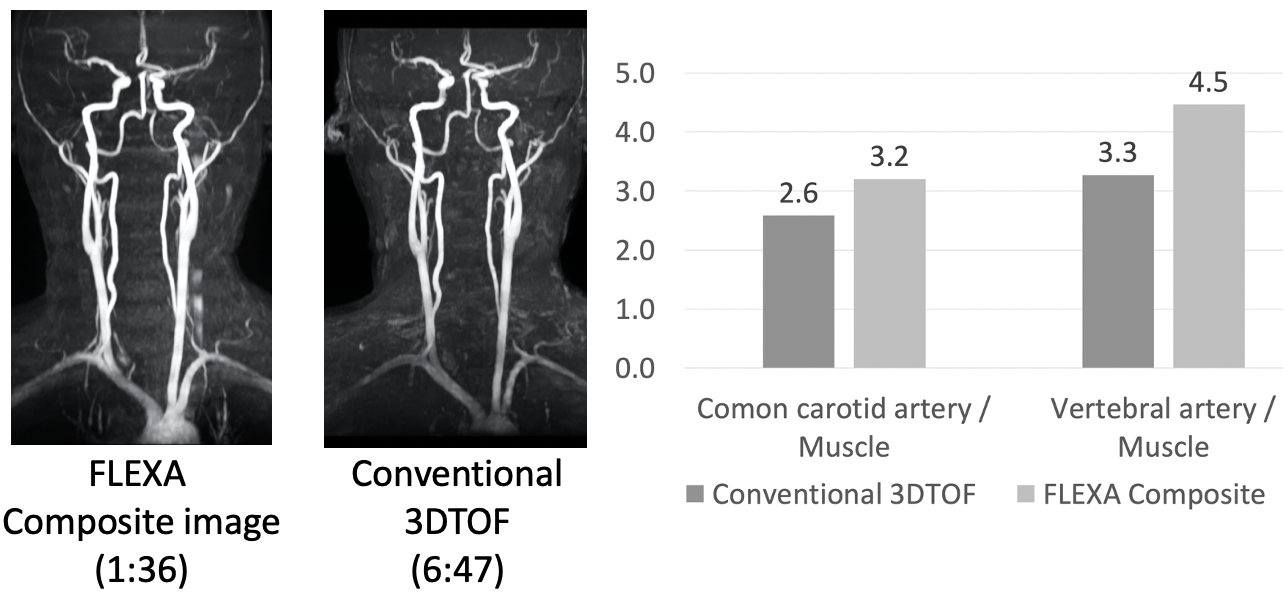
Figure.3. Comparison
results to conventional 3DTOF with a healthy volunteer. FLEXA 3DTOF showed higher
image contrast between artery and muscle at common carotid artery and vertebral
artery with a significant speedup of 3D acquisition in the equivalent voxel
size.
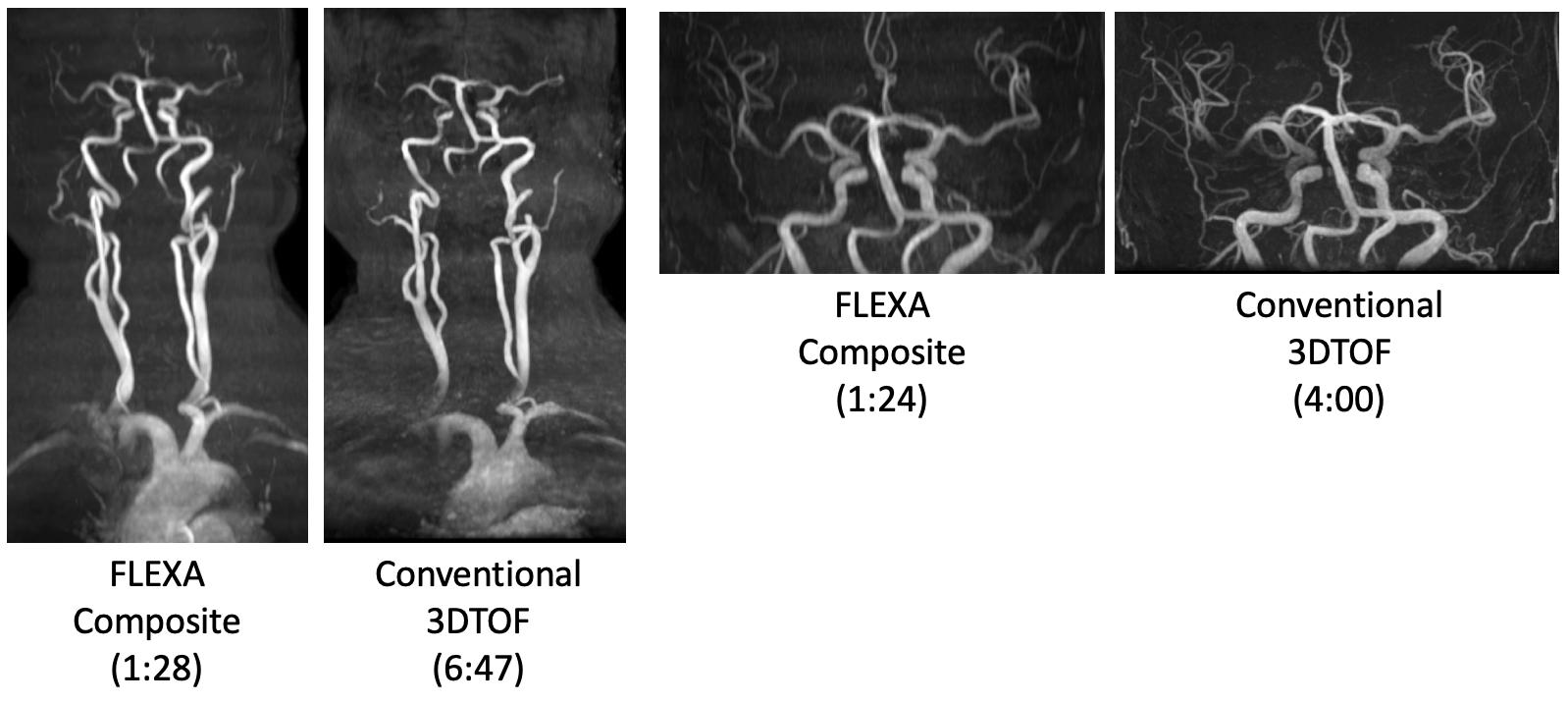
Figure.4.
Comparison results to conventional 3DTOF with a patient of 81 years that is
expected to have slowing flow of blood. FLEXA 3DTOF was able to depict both the
whole carotid artery and intracranial artery with the comparable MIP image to
conventional 3DTOF. For the brain MRA, spatial resolution of conventional 3DTOF
and FLEXA was 0.4x0.9x0.8 mm3 and 1.1x0.5x1.4mm3, respectively.

Table.1. Scan
parameter for carotid artery scan for conventional 3DTOF and FLEXA 3DTOF
DOI: https://doi.org/10.58530/2022/4130