4129
The Reliability of CMR Fast Late Gadolinium Enhancement Sequence in The Evaluation of Patients with Acute Myocardial Infarction1Beijing Friendship Hospital, bei jing, China
Synopsis
By comparing the three kinds of LGE images of 110 patients with AMI, and taking the current standard turbo FLASH imaging sequence as reference, this study verified the accuracy of using moco bSSFP and TrueFISP to evaluate the lesions in patients with AMI. The research covers image quality evaluation and qualitative diagnosis accuracy evaluation. The results show that moco bSSFP sequence and TrueFISP sequence have equivalent effect as turbo FLASH sequence in the qualitative diagnosis, but their image quality is better than that of turbo FLASH sequence.
Introduction and Purpose:
As a sophisticated method for detecting organic and structural heart disease, Cardiovascular Magnetic Resonance (CMR) Imaging features non-invasive examination and reliable lesion display. CMR Imaging evaluates the extent and nature of lesions, and decides clinical treatment and prognostic evaluation. In recent years, CMR has been widely applied at all-level hospitals. Patients raise ever-increasing demands for CMR, especially those with acute myocardial infarction (AMI)[1]. With regard to AMI, the number of infarctions and symptoms of microvascular obstruction (MVO) and intramyocardial hemorrhage (IMH) are evidences for evaluating the severity of patient conditions and prognosis[2]. Late Gadolinium Enhancement (LGE) sequence is an indispensable part of CMR acquisition. In this sequence, infarction/fibrosis is manifested as characteristic high signal, while MVO as low signal in the high signal area. In this way, it achieves the accurate evaluation of AMI patients’ lesions. Therefore, through LGE standard imaging sequence, with reference to Phase-Sensitive Inversion-Recovery (PSIR) Turbo FLASH pulse sequence (segmented PSIR-turboFLASH (turbo FLASH) under segmented, rapid and low-angle acquisition, the accuracy of AMI is evaluated by verifying PSIR Single Shot TrueFISP (TrueFISP) and motion-corrected, free-breathing single-shot PSIR balanced steady state free precession (moco bSSFP).Materials and Methods:
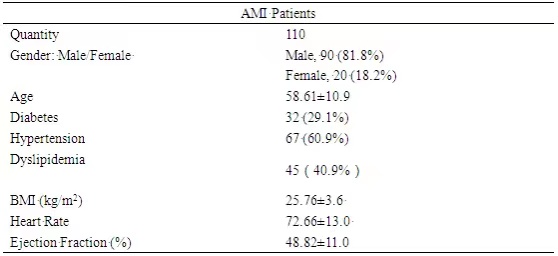
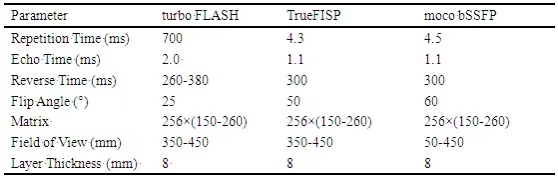
Retrospective collection is carried out for 110 AMI patients’ CMR sequence images, see details in Table 1. The difference between TrueFISP sequence and moco bSSFP sequence regarding image quality, visual qualitative and quantitative diagnosis and the current standard sequence turbo FLASH is evaluated. The 3T system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) is adopted for scanning, and specific parameters are shown in Table 2. Firstly, organoleptic scores are given for image quality of each layer of the three types of delayed enhancement sequences, and the average image score is calculated. The scoring criteria are described below: 4 Points: good image quality; 3 Points: mild artifacts, with no myocardial artifacts; 2 Points: moderate artifacts, myocardial artifacts, and acceptable display of lesion areas; 1 point: severe artifacts, and unable to conduct qualitative/quantitative diagnosis. Secondly, clutter-to-noise ratio (CNR) between LGE area/normal myocardium (NM) and LGE area/MVO are measured. Finally, two physicians qualitatively diagnose as per sequences. Diagnosis method is described below: Firstly, the number of image layers involved in LGE and MVO are recorded. To evaluate image layers more accurately involved in LGE and MVO, each layer of the scanned images is segmented according to 16 Segments Cardiac Segmentation Model published by the American Heart Association (AHA)[3] (six segments in basilar part and papillary muscle, four segments in apex) instead of a layer of segments selected in each part. Hence in this paper, “area” is defined as the minimum unit of heart boundary division, and the number of areas involved in LGE and MVO under the three types of sequences is separately recorded for the same patient.Results:
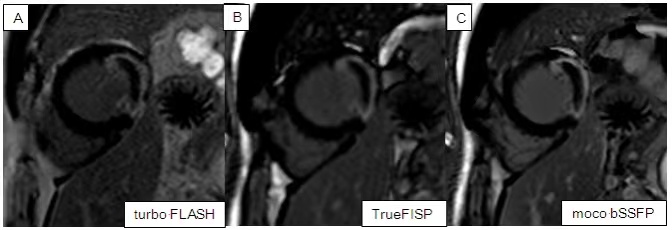
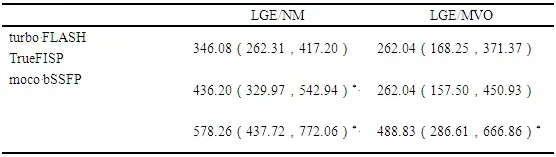
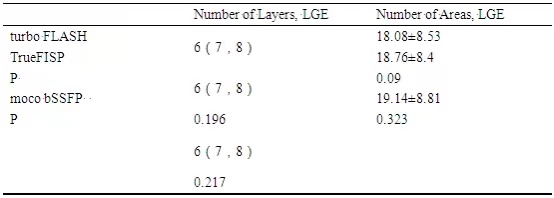
The average image quality scores of turbo FLASH sequence, TrueFISP sequence and moco bSSFP sequence are 3.45 (3.07, 3.64), 3.89 (3.8, 3.91), and 3.91 (3.82, 4), respectively. The average image quality score of moco bSSFP sequence and TrueFISP are significantly higher than that of turbo FLASH sequence, which is statistically significant (p<0.001). The average image quality score of moco bSSFP sequence is significantly higher than that of TrueFISP sequence (p<0.001). LGE sequence image of patients with typical lesions is shown in Figure 1. For CNR measurement, CNR LGE/NM and LGE/MVO of moco bSSFP sequence and CNR LGE/NM of TrueFISP sequence are higher than those of turbo FLASH sequence (P<0.05), and the difference is statistically significant. NR LGE/MVO of TrueFISP sequence shows no significant difference from that of turbo FLASH sequence. See the detailed measurement values in Table 3. After two physicians diagnose and evaluate the three types of LGE sequences of 110 AMI patients, it is found that moco bSSFP sequence and TrueFISP sequence demonstrate no difference with turboFLASH sequence regarding the number of image layers and areas involved in LGE and MVO. See Table 4 for details.Conclusions:
Compared with turbo FLASH sequence, moco bSSFP sequence and TrueFISP sequence are equivalent in qualitative diagnosis of AMI patients, and the image quality is significantly better than that of turboFLASH sequence. In previous studies[4,5,6], moco bSSFP sequence is proved with higher image quality and diagnostic reliability in children/patients with arrhythmia than turbo FLASH sequence. Coupled with the findings of Huber, et al.[7] on the accuracy of TrueFISP sequence in patients with chronic myocardial infarction, although its scanning time is shorter than turbo FLASH sequence, CNR LGE/NM of TrueFISP sequence and quantitative evaluation of lesions are lower than those of the former. Less evaluation is conducted for image quality and diagnostic accuracy in many AMI patients’ moco bSSFP sequence, TrueFISP sequence and turbo FLASH sequence. This paper fills the gap in this regard and is of reference significances for the clinical applications of moco bSSFP sequence, TrueFISP sequence and turbo FLASH sequence.Acknowledgements
Great gratitude is hereby expressed to all the staff who contribute to this paper.References
1. Kramer CM, Barkhausen J, Bucciarelli-Ducci C, et al. Standardized cardiovascular。magnetic resonance imaging (CMR) protocols: 2020 update. J Cardiovasc Magn Reson, 2020, 22(1): 17.
2. Betgem RP, Waard GA, Nijveldt R. Intramyocardial haemorrhage after acute myocardial infarction. NATURE REVIEWS | CARDIOLOGY.
3. Schulz-Menger J, Bluemke DA, Bremerich J. Standardized image interpretation and post processing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) Board of Trustees Task Force on Standardized Post Processing. Journal of Cardiovascular Magnetic Resonance 2013, 15:35.
4. Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, Finn JP, Judd RM. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001;218(1):215–23.
5. Piehler KM, Wong TC, Puntil KS, et al. Free-breathing, motioncorrected late gadolinium enhancement is robust and extends risk stratification to vulnerable patients. Circ Cardiovasc Imaging 2013;6(3):423e32.
6. Sievers B, Elliott MD, Hurwitz LM, et al. Rapid detection of myocardial infarction by subsecond, free-breathing delayed contrast-enhancement cardiovascular magnetic resonance. Circulation 2007;115(2):236e44.
7. Huber A,Hayes C, Spannagl B. Phase-Sensitive Inversion Recovery Single-Shot Balanced Steady-State Free Precession for Detection of Myocardial Infarction During a Single Breathhold. Academic Radiology, Vol 14, No 12, December 2007.
Figures