4128
Co-registration of cardiac PET and late gadolinium enhancement MRI for integrated PET/MR1Shanghai Jiao Tong University, Shanghai, China, 2United Imaging Healthcare Co. Ltd., Shanghai, China, 3Shanghai East Hospital, Shanghai, China, 4United Imaging Healthcare Co. Ltd., Houston, TX, United States
Synopsis
A two-stage cardiac PET/late gadolinium enhancement (LGE) co-registration method proposed here significantly improved the co-registration between PET and LGE in integrated PET/MR imaging. The two-stage method led to increased registration score (4.93±0.89) versus no-registration (3.49±0.84, p<0.001) and a single-stage method (4.23±0.81, p<0.001), an increased SUV value in the normal myocardium (3.87±2.56) compared with the no-registration (3.14±1.92, p<0.001) and the single-stage method (3.32±2.16, p<0.001). The technique may improve diagnostic accuracy of non-ischemic cardiomyopathies via better image co-registration.
PET and MR are two commonly used imaging modalities for clinical assessment of non-ischemic cardiomyopathies, including but not limited to Dilated Cardiomyopathy (DCM) and Hypertrophic Cardiomyopathy (HCM) 1. Integrated PET/MR combines the advantages of each modality, providing a more convenient, fast, and integrated imaging method for diagnosing and assessing non-ischemic cardiomyopathies 2. However, respiratory motion causes mismatches between PET images of the myocardium and the corresponding cardiac MR images in cardiac integrated PET/MR, even when both modalities are concurrently applied 3. The mismatch may affect the attenuation correction and the diagnosis of non-ischemic cardiomyopathies. In this study, we present a two-stage cardiac PET and MR Late Gadolinium Enhancement (LGE) co-registration method to mitigate this problem, with an ultimate aim to improve the diagnostic accuracy of integrated PET/MR for non-ischemic cardiomyopathies.
METHODS
Figure 1 shows the workflow for the proposed two-stage PET/LGE co-registration method, which employs the 3D MRAC FLASH image as an intermedia to fulfill the registration between 3D PET and 2D LGE. In the first stage, List-Mode PET data is sorted into eight respiratory bins based on the respiratory signal acquired by respiratory bellows and reconstructed separately for each respiratory phase. The respiratory-phase resolved PET image is then manually compared with the 3D MR FLASH image, which is acquired concurrently and reconstructed by using only end-expiration data, to find out the phase of the PET data best-matched to the FLASH. In the second stage of the registration, rigid registration is manually performed between 3D FLASH and 2D multi-slice LGE to obtain a 3D displacement field, which is then used to warp the PET image that is already matched to the 3D FLASH to the LGE image.
The performance of the proposed two-stage PET/LGE co-registration method was evaluated by comparison with no-registration and one-stage direct PET/LGE co-registration, as shown in Fig 2. When no registration was performed, PET was reconstructed with all data (Image 1), mimicking the typical clinical workflow. Image 2 was generated by a one-stage co-registration between the respiratory-phase resolved PET images and the multi-slice 2D LGE images. Finally, Image 3 was generated based on the proposed method.
A total of 33 patients referred to cardiac 18F-FDG PET/MR scans between May 2020 and September 2021 were retrospectively enrolled in the study. The final cohort consisted of 25 patients, including 12 HCM patients and 13 DCM patients, after excluding 1 for incomplete data acquisition, 3 for LGE with severe artifacts, and 4 for lack of myocardial FDG uptake which is required to facilitate the quantitative analysis shown below (cf. Table 1).
One hundred and sixty slices of LGE and forty lesions were studied. The co-registration quality was assessed qualitatively by two trained nuclear medicine physicians, and quantitatively by changes of mean SUV in the normal myocardium and the LGE-enhanced lesions. Wilcoxon signed-rank test was used for qualitative data and paired t-test for quantitative data. P=0.05 was considered statistically significant.
RESULTS
Figure 3 shows some representative examples before and after the application of the two-stage registration. Figure 4 shows the statistical analysis of the qualitative and quantitative comparison of the 3 co-registration methods. The two-stage method had an improved image registration score (4.93±0.89) compared with the no-registration method (3.49±0.84, p<0.001) and the single-stage method (4.23±0.81, p<0.001). Furthermore, the two-stage method led to an increased SUV value in the myocardium (3.87±2.56) compared with the no-registration method (3.14±1.92, p<0.001) and the single-stage method (3.32±2.16, p<0.001). The mean SUV in the LGE lesion significantly increased from 2.51±2.09 to 2.85±2.35 (p<0.001) after the two-stage co-registration, as shown in Figure 4. Histogram of the S-I direction displacement between LGE and PET showed that 34.4%, 50%, 63.7% of the patients had a displacement in the range of 0~2 mm, 0~4 mm, and 0~6 mm, respectively.
DISCUSSION
The proposed two-stage registration method significantly improves the registration quality of PET/LGE in myocardial PET/MR imaging. Accurate matching between PET/LGE is important for the diagnosis of non-ischemic cardiomyopathy, where both modalities are commonly used 4-6. Our study shows that misregistration between PET and LGE is common in integrated PET/MR imaging, with 50% of the studied population showing image mismatches along the S-I direction larger than 4 mm. The proposed method may greatly improve the co-registration quality in these patients, facilitating a more accurate analysis of the underlying pathology with integrated imaging.
Only patients with a significant myocardial FDG uptake were included in the study so that we can use the increase of SUV as a surrogate for accurate co-registration. The myocardium where FDG uptake is lower than that in the blood pool, usually from the fasting patient group, was not clearly visualized and thus excluded from further analysis .
In conclusion, we propose a two-stage cardiac PET/LGE co-registration method for integrated cardiac PET/MR imaging that is applicable for 2D short-axial LGE and 3D PET images. The technique may improve the diagnostic accuracy of non-ischemic cardiomyopathies via better image co-registration. The technique provides a convenient and easy-to-operate solution to make myocardial PET/MR quantitative analysis feasible.
Acknowledgements
No acknowledgement found.References
1. Jagsi R, Moran JM, Kessler ML, Marsh RB, Balter JM, Pierce LJ. Respiratory Motion of The Heart and Positional Reproducibility Under Active Breathing Control. International Journal of Radiation Oncology*Biology*Physics. 2007; 68:253-8. doi: 10.1016/j.ijrobp.2006.12.058.
2. Nazir MS, Ismail TF, Reyes E, Chiribiri A, Kaufmann PA, Plein S. Hybrid positron emission tomography-magnetic resonance of the heart: current state of the art and future applications. Eur Heart J Cardiovasc Imaging. 2018; 19:962-74. doi:10.1093/ehjci/jey090.
3. Nekolla SG, Martinez-Moeller A, Saraste A. PET and MRI in cardiac imaging: from validation studies to integrated applications. Eur J Nucl Med Mol Imaging. 2009;36 Suppl 1: S121-30. doi:10.1007/s00259-008-0980-1.
4. Kong EJ, Lee SH, Cho IH. Myocardial Fibrosis in Hypertrophic Cardiomyopathy Demonstrated by Integrated Cardiac F-18 FDG PET/MR. Nucl Med Mol Imaging. 2013;47:196-200. doi:10.1007/s13139-013-0201-0.
5. Yamaguchi H, Hasegawa S, Yoshioka J, Uehara T, Hashimoto K, Kusuoka H, et al. Characteristics of myocardial 18F-fluorodeoxyglucose positron emission computed tomography in dilated cardiomyopathy and ischemic cardiomyopathy. Ann Nucl Med. 2000;14:33-8. doi:10.1007/bf02990476.
6. Lassen ML, Rasul S, Beitzke D, Stelzmuller ME, Cal-Gonzalez J, Hacker M, et al. Assessment of attenuation correction for myocardial PET imaging using combined PET/MRI. J Nucl Cardiol. 2019;26:1107-18. doi:10.1007/s12350-017-1118-2.
Figures
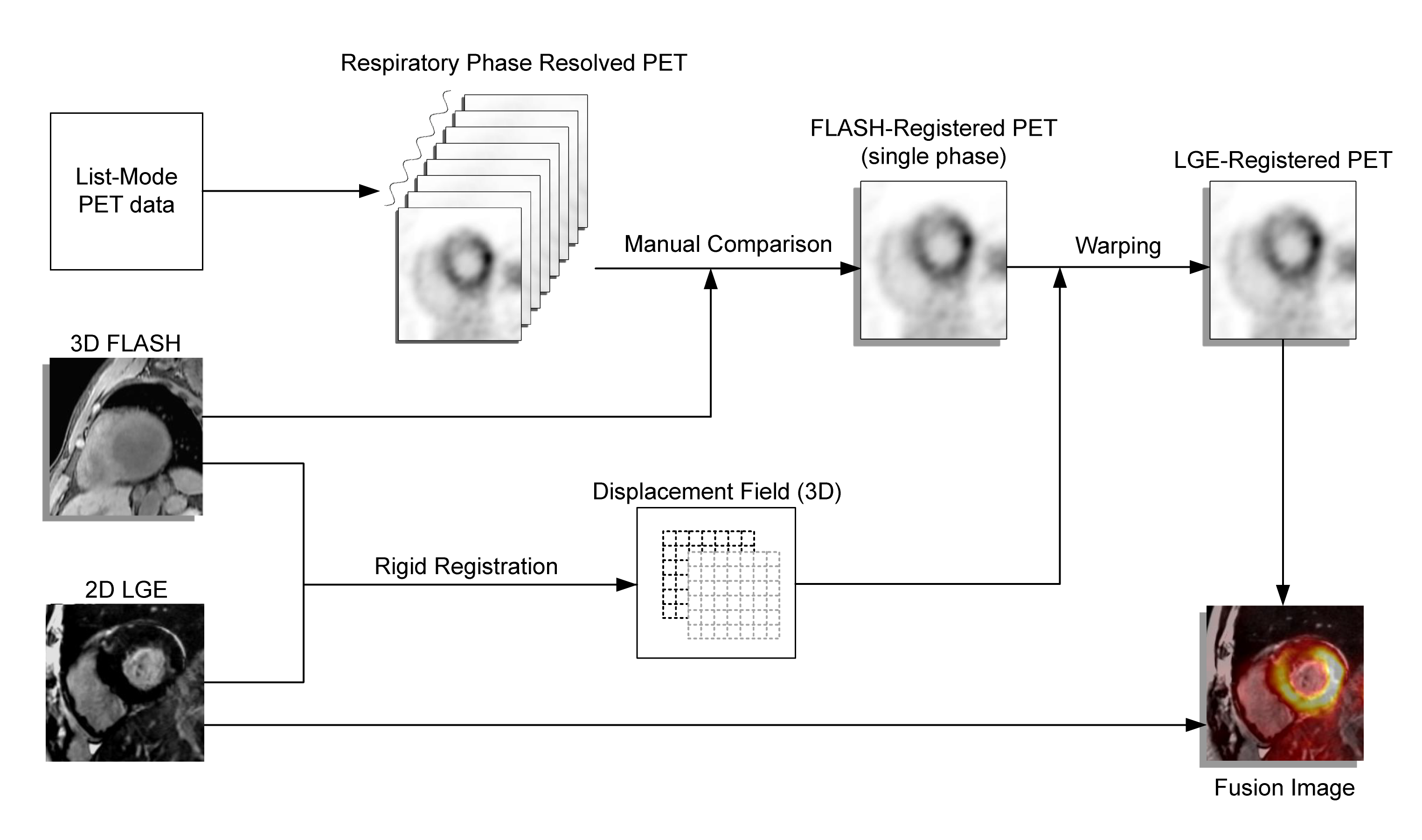
Fig. 1 Image co-registration of LGE and PET with a two-stage process. Firstly, List-Mode PET data was sorted into eight respiratory bins based on accompanying respiratory signals and separately reconstructed. The respiratory-phase resolved PET image is then manually compared with the 3D MR FLASH image. In the second stage of the registration, rigid registration is manually performed between 3D FLASH and 2D multi-slice LGE to obtain a 3D displacement field, which is then used to warp the PET image that is already matched to the 3D FLASH to the LGE image.
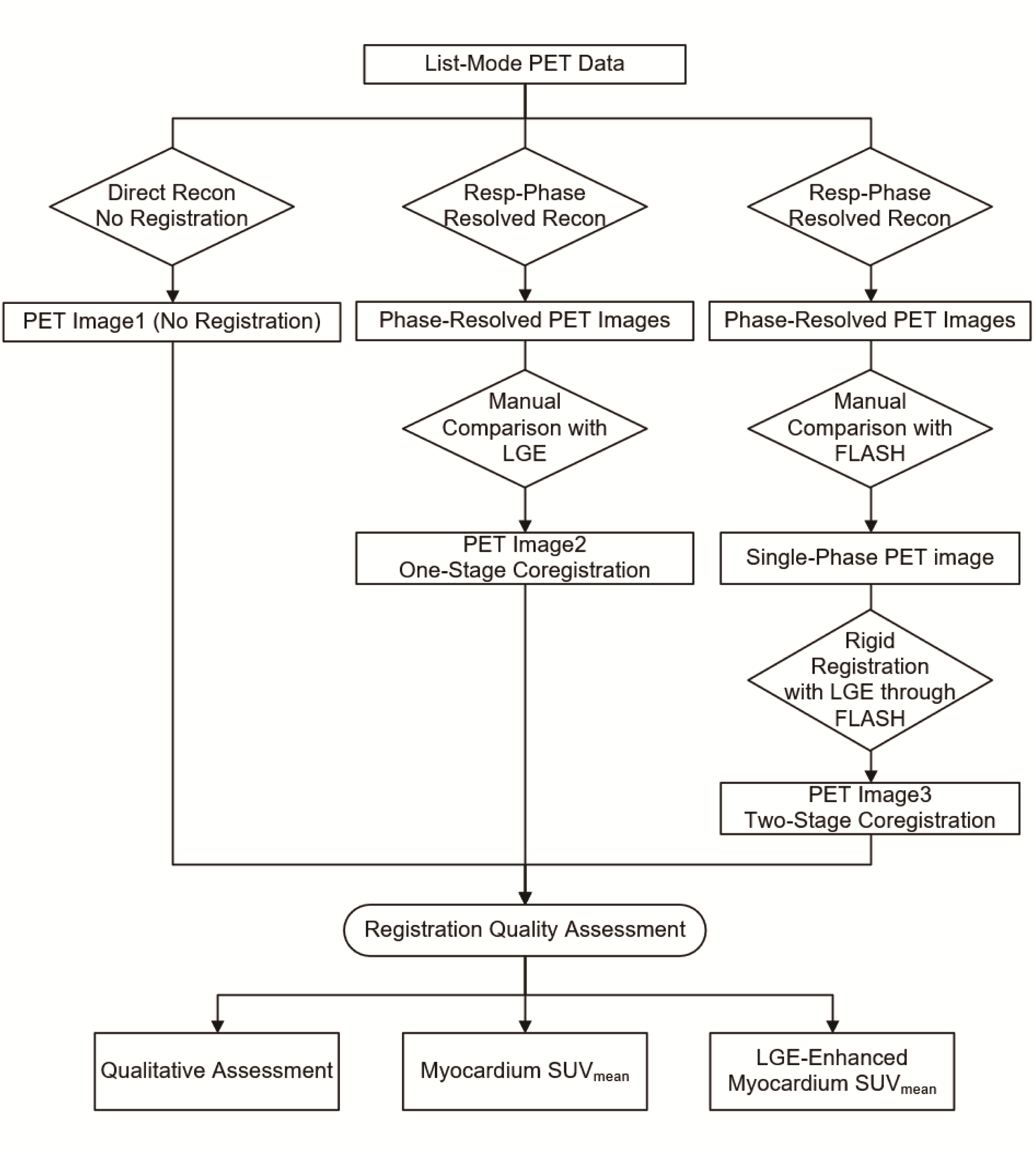
Fig. 2 Schematic layout of the study.
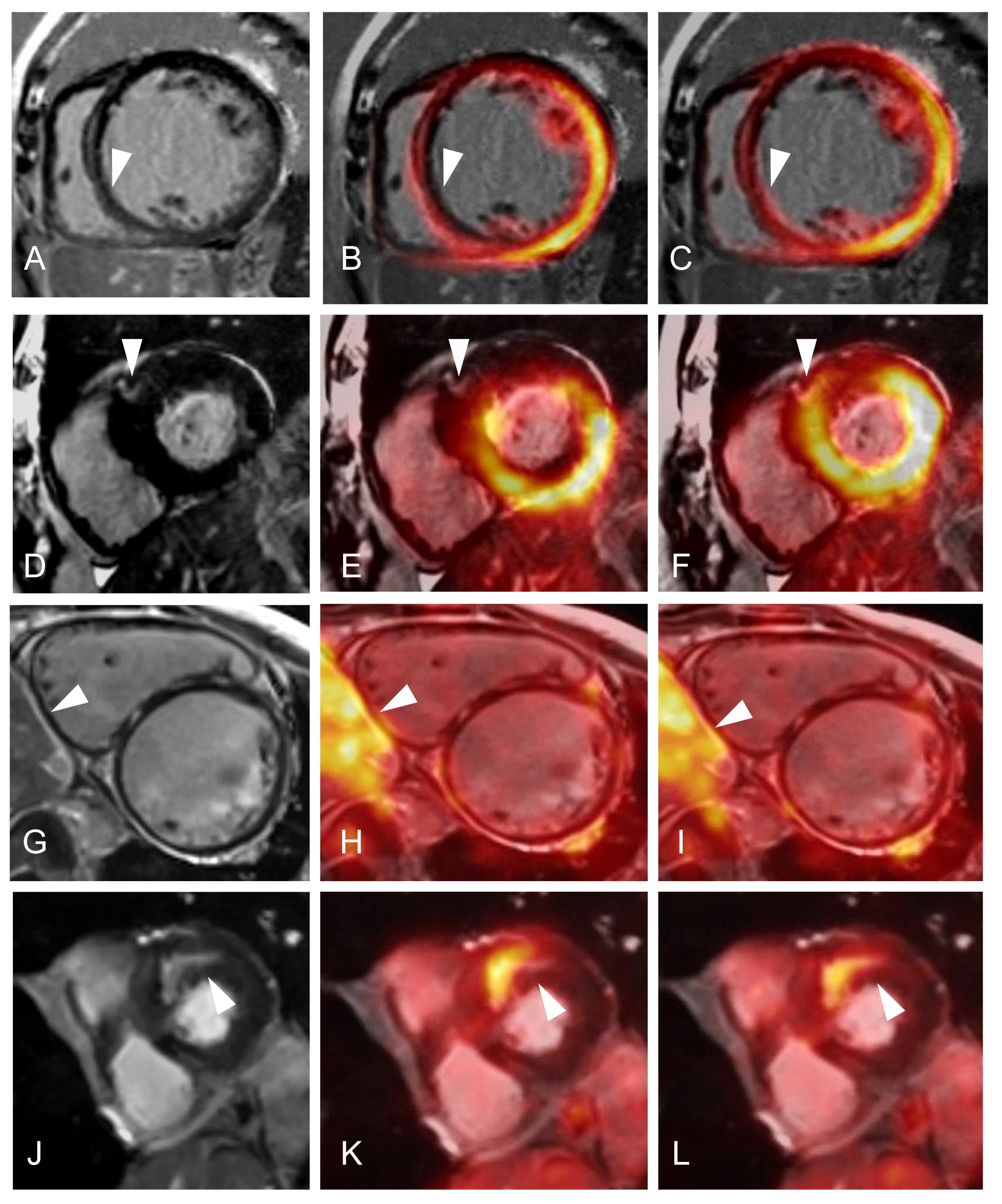
Fig. 3 Comparison of images before and after two-stage registration. (A-C) LGE and PET before registration had obvious mismatches (arrow). (D-F) SUV of one LGE-enhanced lesion changed after two-stage registration for a HCM patient receiving GL PET imaging (arrow). (G-I) A DCM patient receiving GL PET imaging with low myocardial FDG uptake, which is more clear after two-stage registration (arrow). (J-L) The enhancement pattern in LGE matched exactly with FDG uptake pattern after two-stage registration for a HCM patient undergoing fasting PET imaging (arrow).
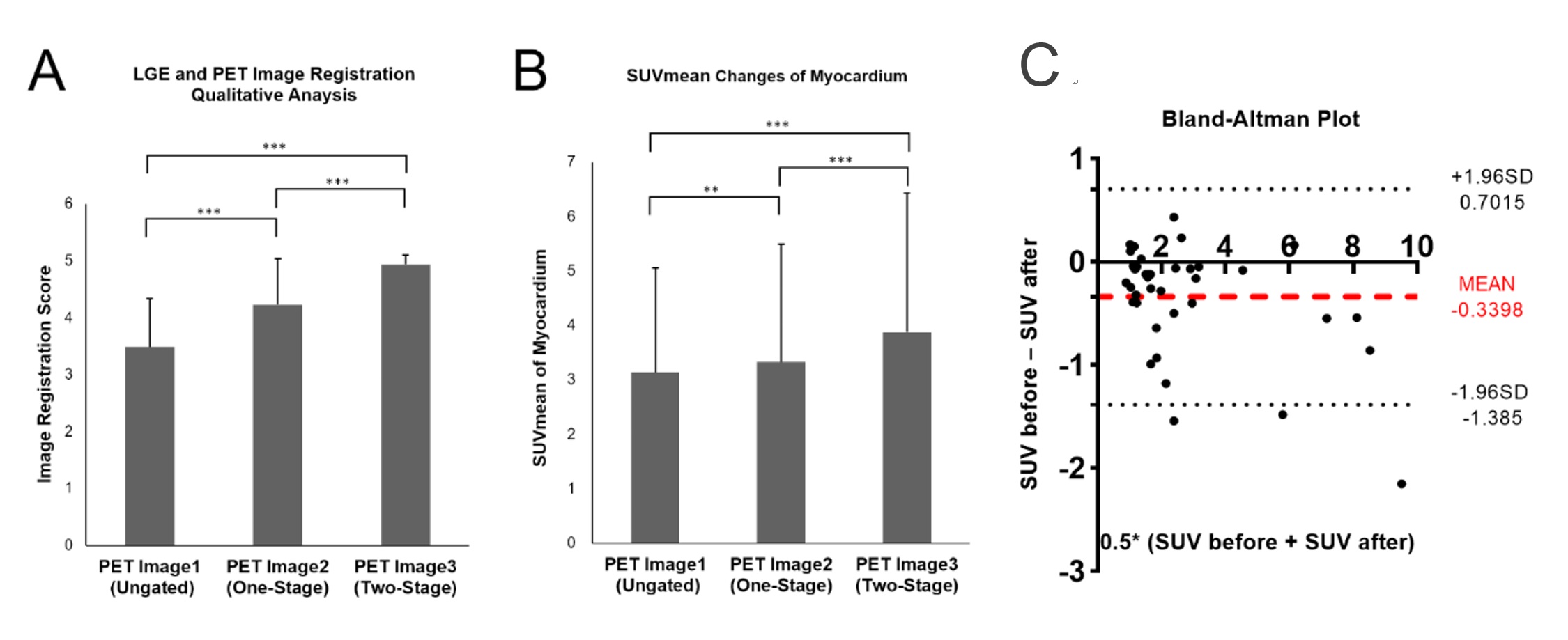
Fig. 4 Registration quality assessment of different registration methods. (A) Image registration score of PET image1/2/3. PET image3 had the highest registration accuracy and statistically significant improvements over other two methods. (B) SUVmean of myocardium was statistically increased with improved registration. Note that *, **, *** represent p value <0.05, 0.01 and 0.001 respectively. (C) Bland-Altman plot of changes of mean SUV in the 40 LGE-Enhanced lesions before and after two-stage registration.
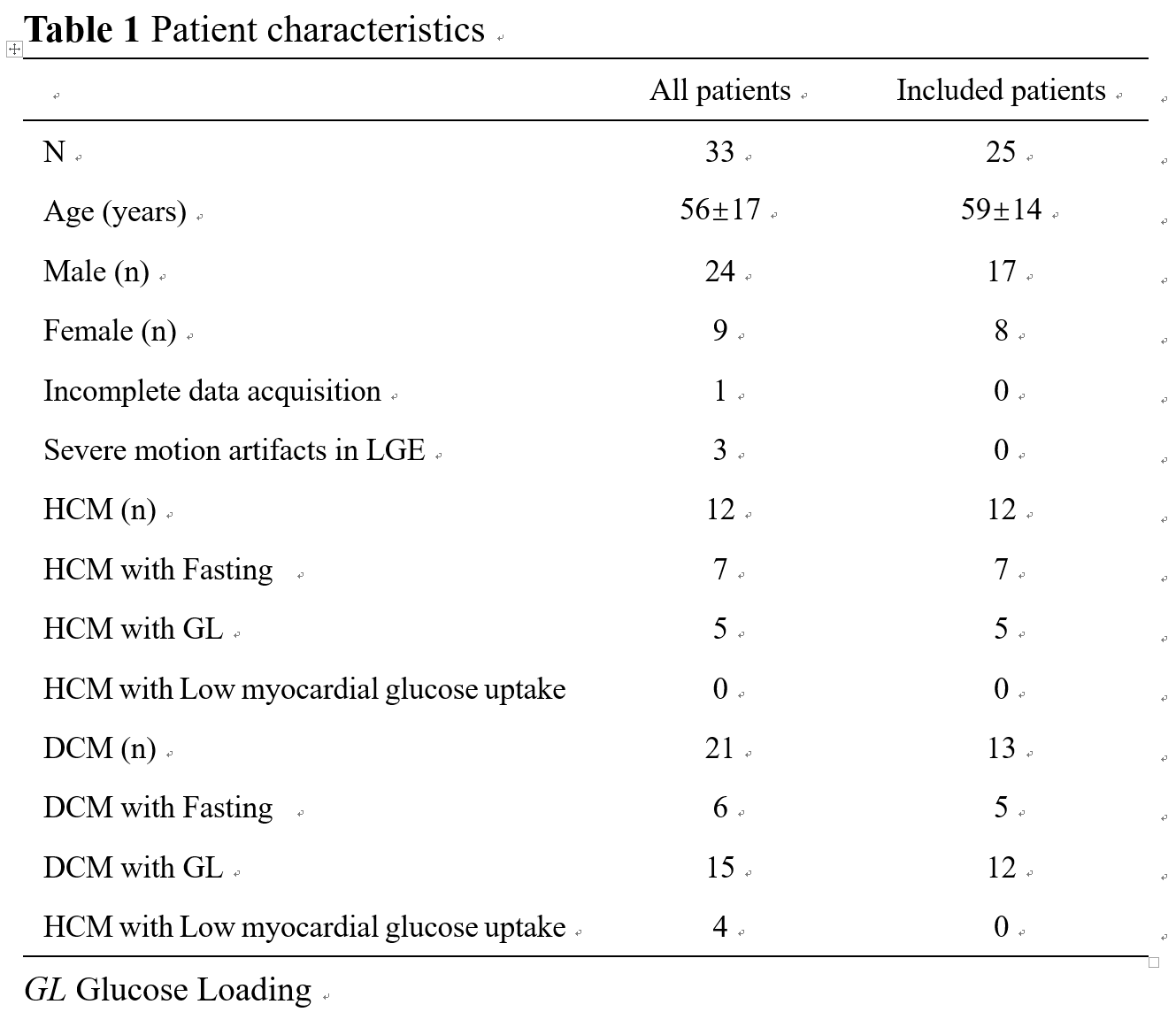
Table 1 Patient characteristics