4120
Left ventricular myocardial motion and fibrosis in patients with repaired tetralogy of Fallot1National Tsing Hua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 4Department of Pediatrics, National Yang-Ming University, Taipei, Taiwan, 5Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan
Synopsis
Repaired tetralogy of Fallot (rTOF) caused diffuse fibrosis due to adverse ventricular reconstruction. T1 mapping was employed to observe the diffuse fibrosis. In patients, the native T1 and peak diastolic longitudinal velocity (Vz) were found to be different from the normal group. We aimed to investigate the relationship between left ventricular myocardial motion and myocardial fibrosis in patients with rTOF.
Introduction
Tetralogy of Fallot (TOF) is a cyanotic congenital heart disease. There are four primary malformations : overriding aorta, pulmonary stenosis, ventricular septal defect(VSD) and right ventricular hypertrophy. TOF patients with repaired operation (rTOF) appear abnormally myocardial fibrosis burden in both ventricles1. The diastolic filling mechanism is impaired due to myocardial stiffness related to increasing regional or diffuse fibrosis2. Tissue Phase Mapping (TPM) cardiac magnetic resonance, which encodes myocardial velocity directly from phase images through phase contrast MRI, has been used in various heart diseases3. A previous study reported that regional myocardial motion provided early indicator of LV myocardial abnormalities in patients with rTOF4. In non-ischemic heart disease, diffuse fibrosis has been found to be associated with myocardial velocity5. However, it is currently uncertain whether diffuse fibrosis caused by adverse ventricular remodeling is associated with myocardial motion in patients with rTOF. Therefore, we aimed to investigate the relationship between left ventricular myocardial motion and myocardial fibrosis in patients with rTOF.Methods
The study cohort recruited 23 patients (23 ± 4 y/o, male/female=15/8) and 19 age-appropriate normal volunteers (21 ± 1 y/o, male/female=11/8). The tissue phase mapping(TPM) and Modified Look-Locker inversion recovery(MOLLI) was performed on a 3.0-Tesla MR scanner (Skyra, Siemens, Erlangen, Germany).TPM was performed with 12-channel-cardiac arrayed coil with prospective ECG trigging(sampling 90% of cardiac cycle) and navigator-guided free-breathing technique, and scanning parameters were TR/TE=27.2/4.5 ms, flip angle=7∘, voxel size=1.1×1.1×6 mm3, and Venc=15 cm/s in-plane and 25 cm/s through-plane. A single-breath-hold ECG gated MOLLI sequence with single-shoot bSSFP readout was acquire in diastole, and scanning parameters were TR/TE=2.57/1.2 ms, flip angle=35∘, voxel size=1.1×1.1×8 mm3 . The regions-of-interest (ROIs) of myocardial on basal, mid, and apical slices were manually determined on magnitude images and were applied to phase images for wall motion velocity and to T1 maps for native T1. The delineated myocardial ROIs on basal, mid, and apical slices in the LV were divided into 16 segments as recommend by America Heart Association (AHA). The peak diastolic and systolic velocity in radial (Vr) and longitudinal (Vz) directions were evaluated. Mann-Whitney U test and Pearson correlation were employed when appropriate. A p<0.05 was considered as statistical significance.Results
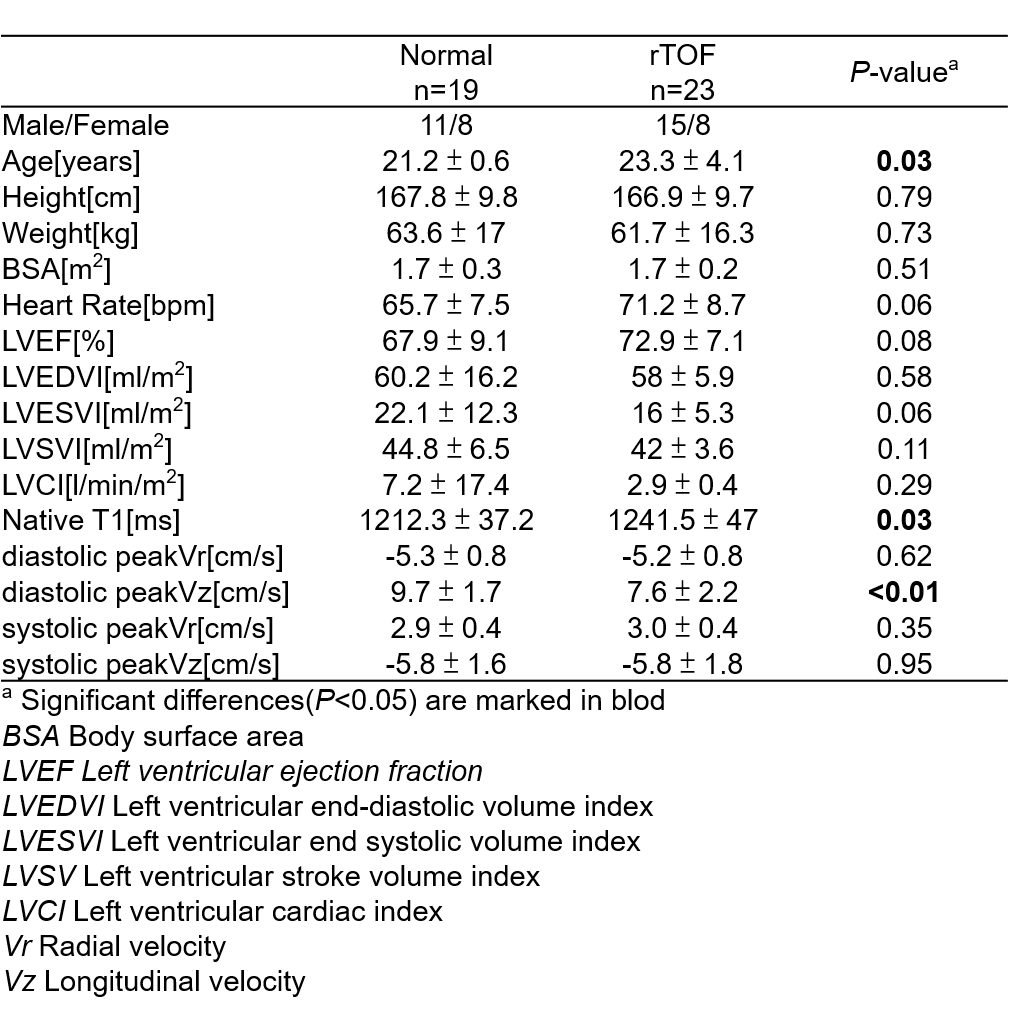
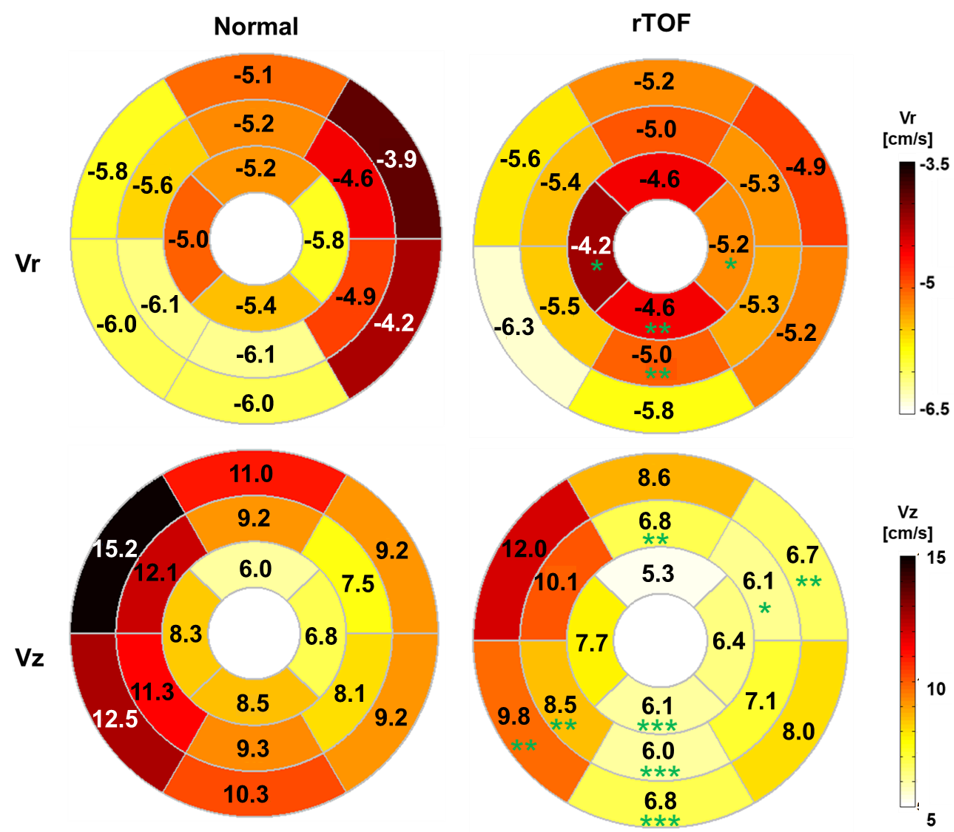
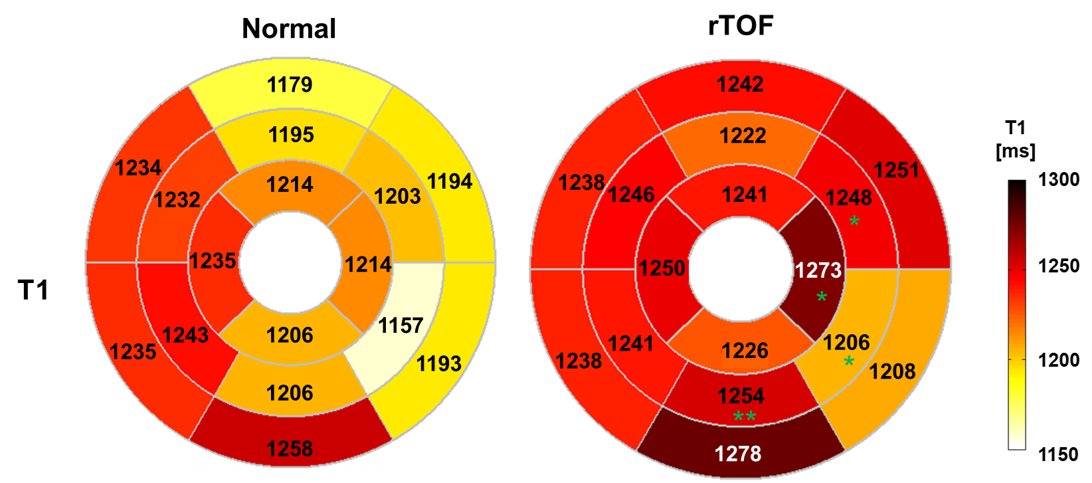
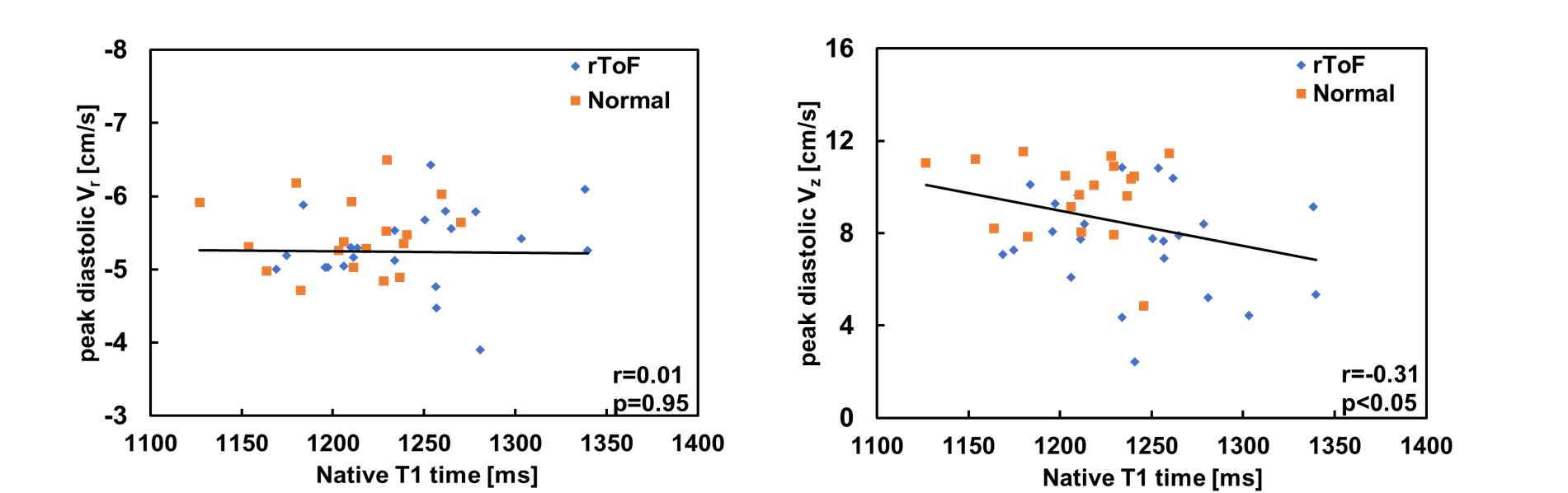
Table 1 lists demographics cardiac MRI volumetric parameters, native T1, and myocardial motion in normal and rTOF groups. In comparison with normal group, rTOF group exhibited increased native T1(1241.5 ± 47 vs 1212.3 ± 37.2, p=0.03). The rTOF group presented significantly decreased peak diastolic Vz than normal group (7.6 ± 2.2 vs 9.7 ± 1.7 cm/s, p=0.002). The mean native T1 of 16 segments are comparable in normal and rTOF groups. The bull’s eye plots shown in Figure 1 illustrates segmental peak diastolic Vr and Vz in normal and rTOF. In comparison with normal group, rTOF group presented lower diastolic Vr, mainly in apical and mid-inferior segments(p<0.05~0.01). The rTOF group exhibited significantly lower Vz, mainly in inferolateral and anterolateral segments(p<0.05~0.001). In Figure 2, the rTOF group possessed higher native T1 in four inferolateral segments (p<0.05~0.01). Figure 3 displays that global peak diastolic Vz presented weak negative correlation with global native T1(r=-0.31, p<0.05).Discussion and Conclusions
In this study, global peak diastolic Vz in rTOF was lower than normal group. More, we found significant reduced peak diastolic Vr and Vz in rTOF group, particularly in lateral segments. Although the global native T1 was comparable in rTOF and normal groups, the segmental T1 of specific inferolateral segments demonstrated significantly lower values in rTOF group. A previous study reported that changes in ventricular function can be detected before perceptible changes in ventricular geometry5, delineating the importance of functional myocardial motion in an early disease progress. In this study, we found decreased global Vz and decreased segmental Vr and Vz in rTOF group with preserved left ventricular volumes and LVEF, which underscored the sensitivity of myocardial motion in detecting altered myocardial function. In this study, the global myocardial motion only presented abnormality in Vz but not in Vr. However, in a segmental analysis of myocardial motion, both Vr and Vz demonstrated altered myocardial motion in rTOF group, underscoring the importance of detecting subtle regional changes of myocardial motion in early disease progress. Similarly, the comparable global native T1 and perceptible T1 changes in specific segments also supported the importance of segmental analysis from a viewpoint of myocardial fibrosis. A previous study reported that fibrosis was found to be associated with decreased systolic and diastolic longitudinal velocity in non-ischemic cardiomyopathy5. In our study, we also found a negative correlation between peak diastolic Vz and native T1. Although segmental analyses in myocardial motion and native T1 discovered subtle abnormalities before global changes, interestingly, we also found that two inferoseptal and two anterolateral segments abnormal Vr or Vz but comparable T1. This finding might delineate that the functional motion changes can be detectable earlier than diffusive microfibrosis.In conclusion, segmental analyses of peak diastolic Vr and Vz and native T1 could detect myocardial abnormality in rTOF patients with preserved LV volumes and LVEF. There was a negative correlation between peak diastolic Vz and native T1. Altered myocardial motion might present earlier than perceptible microfibrosis in specific inferoseptal and anterolateral segments.
Acknowledgements
No acknowledgement found.References
1. Kozak et al. "Diffuse myocardial fibrosis following tetralogy of Fallot repair: a T1 mapping cardiac magnetic resonance study." Pediatric radiology 44.4 (2014): 403-409.
2. Ellims et al. "Diffuse myocardial fibrosis in hypertrophic cardiomyopathy can be identified by cardiovascular magnetic resonance, and is associated with left ventricular diastolic dysfunction." Journal of Cardiovascular Magnetic Resonance 14.1 (2012): 1-9.
3. Foell "Hypertensive heart disease: MR tissue phase mapping reveals altered left ventricular rotation and regional myocardial long-axis velocities. " European Radiology. 2013;23(2):339-347.
4. Chang "Left ventricular regional myocardial motion and twist function in repaired tetralogy of Fallot evaluated by magnetic resonance tissue phase mapping." European radiology 28.1 (2018): 104-114.
5. Yamasaki et al. "Clinical impact of left ventricular eccentricity index using cardiac MRI in assessment of right ventricular hemodynamics and myocardial fibrosis in congenital heart disease." European radiology 26.10 (2016): 3617-3625.
Figures