4117
Left ventricular-aorta energy efficiency in patients with repaired tetralogy of Fallot1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
Synopsis
In this study, we defined a ratio of aortic KE and LV KE to represent LV-Ao efficiency. We aimed to evaluate LV-Ao energy efficiency in rTOF patients and evaluate the relationship between LV-Ao efficiency and RV hypertrophy. The aortic root KE, LV KE, and LV-Ao efficiency in rTOF group were comparable with normal group. The indexed LV-Ao efficiency was negatively correlated with age and RV volumetric parameters. The association between LV-Ao efficiency and age and RV hypertrophy suggested that the adverse interaction between RV and LV was expanded to the aorta in rTOF patients with preserved LV function.
Introduction
In patients with repaired tetralogy of Fallot (rTOF), left ventricular (LV) dysfunction may result in sudden death [1,2]. A previous study reported that aortic dilatation and regurgitation in rTOF patients may contribute to LV dysfunction [3]. Ventricular kinetic energy (KE) is able to assess cardiac performance and reduced ratio of aortic flow-to-LV KE precedes LV dysfunction [4]. However, the ratio of aortic flow-to-LV KE may underestimate the efficiency because of calculation of cross-sectional mean flow possessing regurgitation. In this study, we defined a ratio of aortic KE and LV KE, which was computed pixelwisely to avoid the underestimation of efficiency, to represent the LV-aorta energy efficiency. The purpose of this study was to evaluate LV-Ao efficiency in rTOF patients and evaluate the relationship between LV-Ao efficiency and RV hypertrophy.Methods
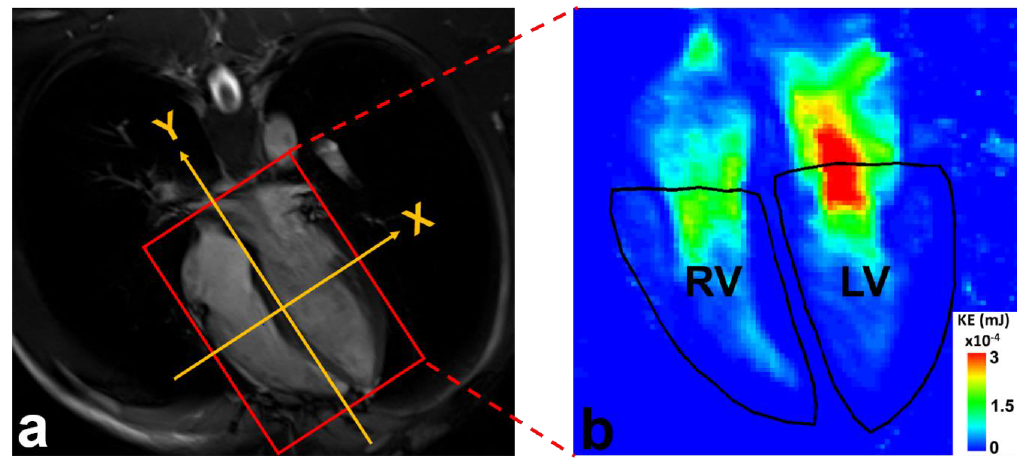
Sixteen patients with rTOF (age 22±4 years, 6 females) and 21 age-matched normal volunteers (age 22±1 years, 10 females) were recruited. All images were acquired in a 3-Tesla MR scanner (Tim Trio or Skyra, Siemens) with prospective ECG-triggering (acquire 90% of RR interval) and navigator to synchronize with cardiac and respiratory motion, respectively. The 4D flow was acquired with TR/TE=10.8/2.9 ms, voxel size=3.2x1.4x3.5 mm3, flip angle=7°, Venc=150 cm/s, and temporal resolution=41.6 ms. The regions-of-interest (ROI) of left ventricle was determined in a 4-chamber view (Figure 1). The plane of aortic root was localized at sinuses of Valsalva and perpendicularly to the long-axis of aorta in the 4D flow data-derived MR angiography. The ROI of the aortic lumen were manually determined in magnitude images and transferred to phase images for computation of aortic flow. The KE was calculated by: $$KE=\frac{1}{2}\rho Vv^{2}$$ where V is the volume of voxel, $$$v$$$ is velocity and $$$\rho$$$ is the blood density with a value of 1060 kg/m3 . The indexed aortic root KE is the sum of pixelwise KE within ROI normalized to BSA. The indexed LV KE is the intraventricular KE indexed to BSA. The peak and mean KE are the maximum and average KE during the cardiac cycle. LV-Ao efficiency and LV-Ao peak efficiency are calculated by: $$LV-Ao\ efficiency\ (a.u.)= \frac{aortic\ mean\ KE\ (mJ)}{LV\ mean\ systolic\ KE\ (mJ)}$$ $$LV-Ao\ peak\ efficiency\ (a.u.)= \frac{aortic\ peak\ KE\ (mJ)}{LV\ peak\ systolic\ KE\ (mJ)}$$ The indexed LV-Ao efficiency and LV-Ao peak efficiency are indexed to BSA. Student t test was performed when appropriate. A p<0.05 was considered statistically significant.Results
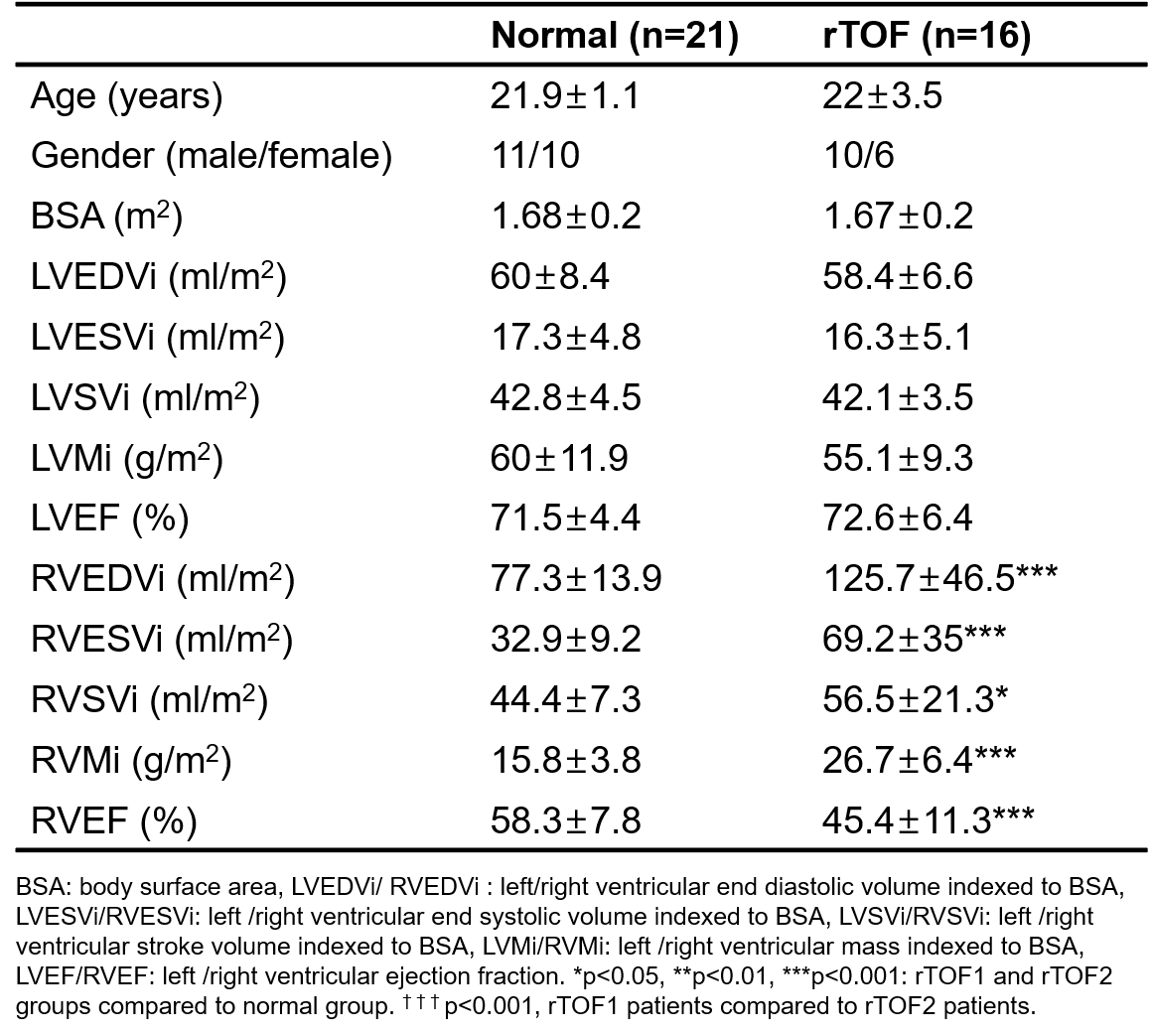
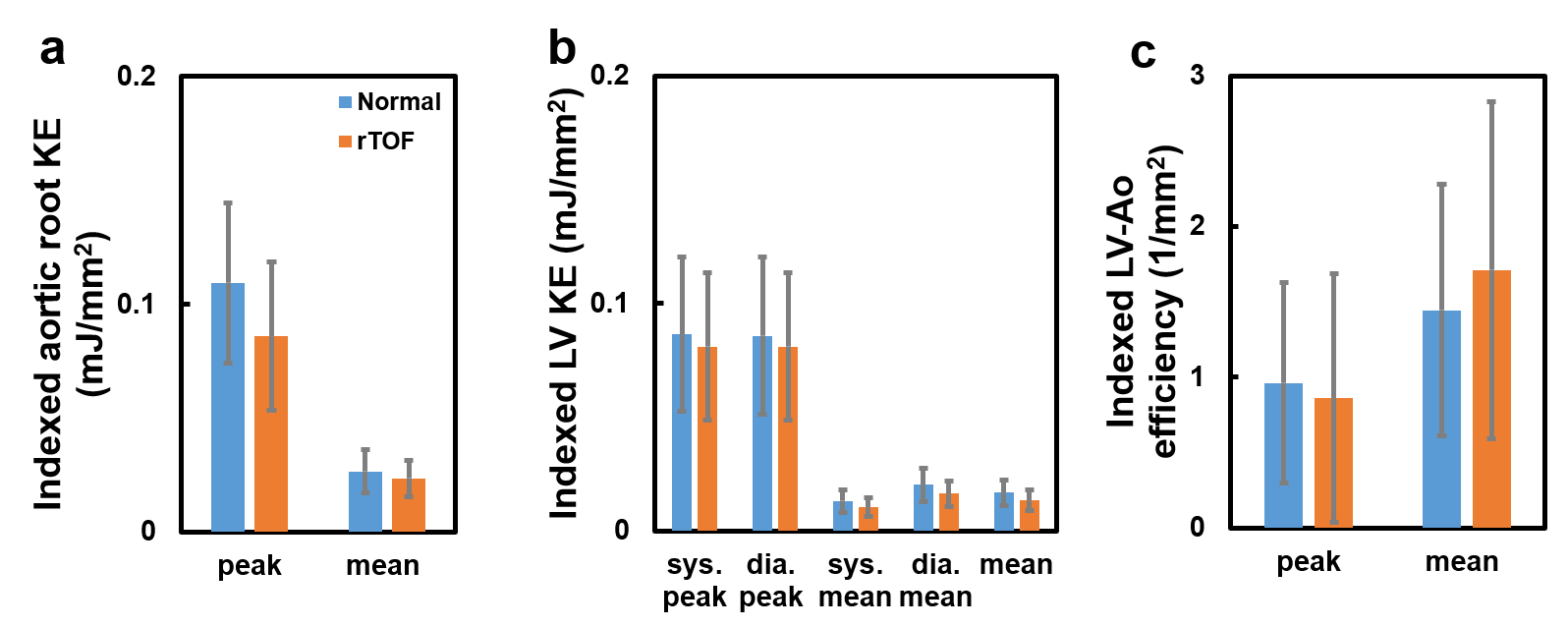
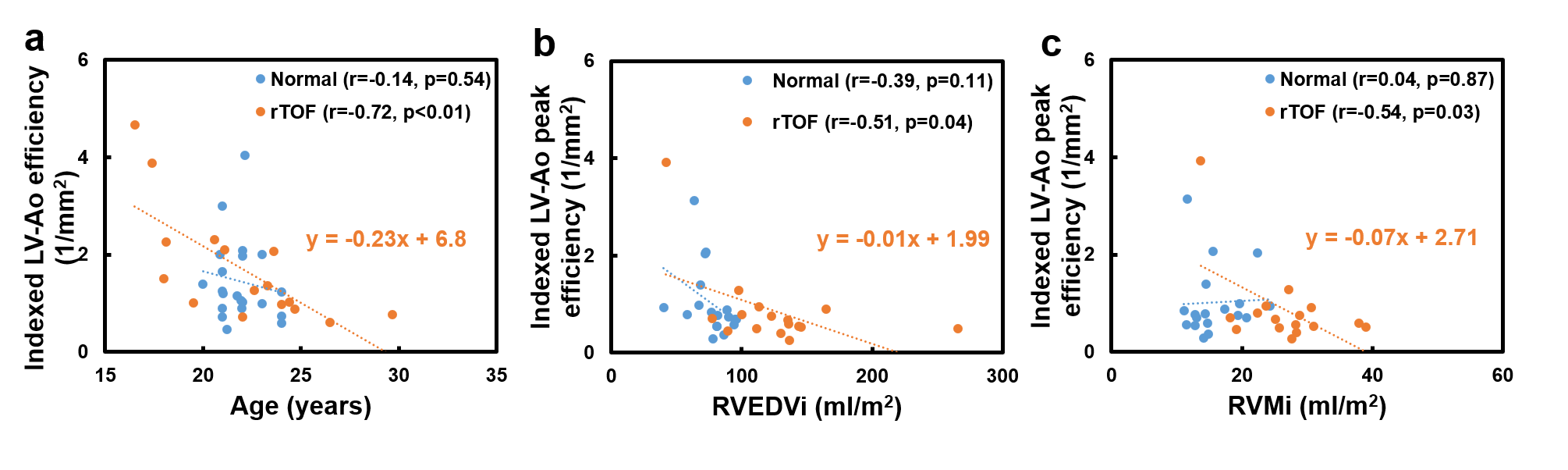
Table 1 summarizes the demographics characteristics in normal and rTOF groups. In comparison with normal group, rTOF group exhibited higher indexed right ventricular (RV) end diastolic and systolic volumes, stroke volume, and mass (all p<0.05~0.001), and significantly decreased RV ejection fraction (p<0.01). The LV volumetric indices and LVEF in rTOF group were comparable with normal group. In Figure 2, rTOF group presented preserved indexed aortic root KE, indexed LV KE and indexed LV-Ao efficiency. In Figure 3, rTOF group exhibited negative correlations between indexed LV-Ao efficiency and age (r=-0.72, p<0.01), RVEDVi (r=-0.51, p=0.04), and RVMi (r=-0.54, p=0.03).Discussion and conclusion
In this study, the aortic root KE, LV KE, and LV-Ao efficiency in rTOF group were comparable with normal group. The indexed LV-Ao efficiency was negatively correlated with age and RV volumetric parameters.A previous study proposed that reduced aortic flow-to-LV KE ratio reflected energy loss in LV and reduced ability of maintaining systemic flow in rTOF patients [4]. However, small patient group with wide age ranged from 7 to 43 years might reduce the soundness of the results. In this study, we recruited rTOF patients with a narrow age range of around 20-year-old. The LV-Ao KE efficiency defined in this study could potentially avoid the underestimation of efficiency in flow with regurgitation.
The rTOF patients exhibited normal aortic root KE and LV KE, suggesting that young patients in our study was in an early disease progress and therefore presented preserved LV function for normally ejecting blood flow from LV to aorta. Nevertheless, the negative correlations between LV-Ao efficiency or LV-Ao peak efficiency and age, RVEDVi, and RVMi suggested the impacts of age and RV hypertrophy on the LV-Ao efficiency even in rTOF patients with preserved LVEF. The adverse interaction between RV and LV was consistent with previous study [6] and the impacts was expanded to the aorta even in an early disease progress in rTOF patients.
In conclusion, LV-Ao efficiency was associated with increasing age and RV hypertrophy in rTOF patients, suggesting that the adverse interaction between RV and LV was expanded to the aorta in rTOF patients with preserved LV function.
Acknowledgements
No acknowledgement found.References
[1] Ghai et al. "Left ventricular dysfunction is a risk factor for sudden cardiac death in adults late after repair of tetralogy of Fallot." Journal of the American College of Cardiology 40.9 (2002): 1675-1680.
[2] Broberg et al. "Prevalence of left ventricular systolic dysfunction in adults with repaired tetralogy of Fallot." The American journal of cardiology 107.8 (2011): 1215-1220.
[3] Grotenhuis et al. "Aortic elasticity and size are associated with aortic regurgitation and left ventricular dysfunction in tetralogy of Fallot after pulmonary valve replacement." Heart 95.23 (2009): 1931-1936.
[4] Jeong et al. "Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot." The Journal of thoracic and cardiovascular surgery 149.5 (2015): 1339-1347.
[5] Sarikouch et al. "Impact of gender and age on cardiovascular function late after repair of tetralogy of Fallot: percentiles based on cardiac magnetic resonance." Circulation: Cardiovascular Imaging 4.6 (2011): 703-711.
[6] Kempny et al. "Right ventricular–left ventricular interaction in adults with tetralogy of Fallot: a combined cardiac magnetic resonance and echocardiographic speckle tracking study." International journal of cardiology 154.3 (2012): 259-264.
Figures