4023
Clinical Evaluation of a Lightweight, Flexible Pediatric RF Coil1Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States
Synopsis
In this abstract, we conducted a clinical evaluation of a prototype lightweight, flexible pediatric RF Coil. We evaluated the image quality on phantoms, an adult volunteer, and four pediatric clinical patients. For the phantom scans, identical 2D GRE protocols were prescribed between arrays and scanners for study reproducibility and accurate image comparisons. For the pediatric clinical patients, different anatomical studies were clinically ordered. Each study was reviewed clinically and found to achieve diagnostic quality with excellent tissue contrast, coverage, and SNR.
Introduction
Magnetic resonance (MR) imaging can be challenging as it is a technique that can suffer from motion artifacts, long scan times, and difficulty acquiring adequate signal/minimizing noise to ensure clinical utility. When working with pediatric patients it is also important to provide a comfortable imaging experience and this is where screen-printed coils have excellent utility 1,2,3. The array’s flexible nature improves patient comfort during scanning, and allows the coils to be closer to the patient, improving form factor and therefore SNR.2 This study investigates the use of a prototype 24-channel pediatric coil4 and its clinical utility.Methods
The RF coil under evaluation was a prototype 24-channel pediatric coil4 (InkSpace Imaging, USA), which was developed using screen-printing technology2,3. The coil is made up of two flexible 12-channel pads, each with array dimensions of 27x25cm 4, making it particularly well suited for body imaging applications for children.Array sensitivity was first evaluated on a phantom (SiOil box phantom, GE Healthcare, USA) on a 3T GE MR750 research scanner and two 3T MR750 clinical hospital scanners using a 2D GRE sequence (TE/TR/FoV/Slice/Matrix/FA = 6.7ms/250ms/40x40cm/10mm/256x256/90°). The InkSpace Imaging prototype4 was evaluated alongside a 32-channel GE cardiac coil and a GE AIR coil (GE Healthcare, USA) adhering to the same 2D GRE protocol for study reproducibility and accurate image comparisons. SNR was then evaluated on an adult volunteer (3T GE MR750 research scanner), and the anatomy imaged was the knee. Again, all three arrays were evaluated with the same 2D GRE protocol (TE=6.7 ms, TR = 250 ms, resolution=1.4 mm isotropic, flip angle = 4). SNR was evaluated using the ROI method on the clinical images (Horos Viewer, Horos Project). Three to four ROIs were drawn at the periphery and near the center of the imaging volume. Images were windowed to ensure that noise was evaluated from an artifact-free region. Resulting SNR values were averaged to report SNR for each image.
After evaluation the prototype coil4 was used for four pediatric scans at the 3T clinical hospital scanner, including one pediatric chest/clavicle scan and three pediatric abdomen studies. The ages of the patients were 2, 10, 11, and 14. These were for clinically ordered studies, performed with UCSF IRB approval.
Results
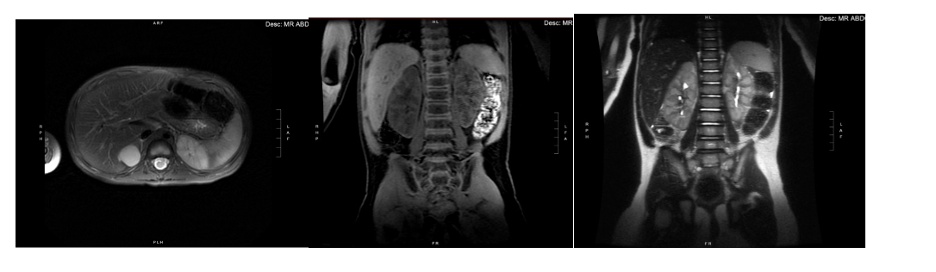
For the phantom evaluation studies, the 24-channel prototype flexible coil4 image quality was excellent, and the visible SNR was comparable or better than both other standard clinical coil configurations under the same imaging protocol. The same results can be seen in the images of the knee in the adult volunteer, which was used to mimic the size of a pediatric subject. In the axial leg images, the average SNR was calculated as 571.8, 210.1, and 328.0 for the InkSpace Imaging coil, AIR coil, and 32-channel cardiac coil, respectively. In the sagittal leg images, the average SNR was found to be 92.2, 83.5, and 72.9 for the InkSpace Imaging coil, AIR coil, and 32-channel cardiac coil, respectively. The decreased element size and increased form factor of the pediatric prototype coil provided more appropriate coverage relative to the adult body arrays, resulting in improved relative SNR.In all clinical studies, the images were reviewed clinically and deemed to be of diagnostic quality. In the abdomen studies, the high quality of the studies is clearly shown in the example images in Figures 2-5. These images show excellent spatial coverage, image SNR, and lack of artifacts. In the chest/clavicle study, there was visible motion artifact in both the prototype pediatric array4 and another “FLEX” coil’s images. This artifact was primarily due to patient motion.
Anecdotally, the technologists running these studies reported that the prototype pediatric coil4 was very easy to setup because of its lightweight and flexible properties.
Discussion/Conclusion
From the evaluation studies, it can be seen that this new flexible coil4 designed specifically for pediatric patients provided high image quality and SNR compared to adult body coils in both the phantom study and the volunteer leg study. Qualitatively the clinical images are crisp and show excellent tissue contrast, coverage, and SNR. The repeatability of the coil image quality was strong as well, with nearly identical phantom scan results on three different 3T scanners (not shown).In conclusion, this prototype coil exhibited excellent, reproducible image quality and improved ease of use while producing equivalent or improved diagnostic images. This demonstrates its ability for eventual more widespread use, and we plan to continue to utilize this coil under IRB.
Acknowledgements
This work is supported by NIH grant R01 HL136965.References
1 Renz, D.M., Herrmann, KH., Kraemer, M. et al. Ultrashort echo time MRI of the lung in children and adolescents: comparison with non-enhanced computed tomography and standard post-contrast T1w MRI sequences. Eur Radiol (2021). https://doi.org/10.1007/s00330-021-08236-7
2 Corea, J., Flynn, A., Lechêne, B. et al. Screen-printed flexible MRI receive coils. Nat Commun 7, 10839 (2016). https://doi.org/10.1038/ncomms10839
3 Simone Angela Winkler, Joseph Corea, Balthazar Lechêne, Kendall O’Brien, John Ross Bonanni, Akshay Chaudhari, Marcus Alley, Valentina Taviani, Thomas Grafendorfer, Fraser Robb, Greig Scott, John Pauly, Michael Lustig, Ana Claudia Arias, and Shreyas Vasanawala, Evalulation of a Flexible 12-channel Screen-printed Pediatric MRI Coil Radiology 2019 291:1, 180-185
4 InkSpace Imaging, 24 Channel Pediatric Coil Array, IFU 001 Rev B (2021-08). The device under evaluation is a prototype with pending 510(k). Use is limited under IRB and the device is not available for sale within the United States.
Figures