4015
Quantitative DCE-MRI Prediction of Breast Cancer Recurrence Following Neoadjuvant Chemotherapy1Division of Hematology and Oncology, Oregon Health and Science University, Portland, OR, United States, 2Oregon Health and Science University, Portland, OR, United States
Synopsis
Neoadjuvant chemotherapy (NAC) is considered standard of care for locally advanced breast cancer. Pre- and post-NAC MRI is routinely used to assess response. This study aims to investigate pre- and post-NAC quantitative DCE-MRI parameters, alone and in combination with clinico-pathologic variables, for prediction of breast cancer recurrence following NAC. 47 patients underwent DCE-MRI studies pre- and post-NAC. The results show that quantitative pharmacokinetic DCE-MRI parameters, whether alone or in combination with clinico-pathologic variables, outperformed tumor size measurement by conventional imaging in prediction of recurrence. Furthermore, DCE-MRI parameters provided added value in predictive performance when combined with clinico-pathologic variables.
Introduction
Neoadjuvant chemotherapy (NAC) is considered standard of care for locally advanced breast cancer. 1 A recent meta-analysis reported a 15-year local recurrence rate of 21.4% in patients who received NAC. 2 Clinico-pathologic factors associated with risk of recurrence include clinical N2 status, estrogen receptor (ER) negative staining, and failure to achieve pathological complete response to NAC. 3 Accurate identification of patients predicted to recur post NAC may help select for appropriate treatment escalation and de-escalation strategies to improve outcomes. Pre- and post-NAC MRI is routinely used in clinical practice to assess response to NAC. This study aims to investigate pre- and post-NAC quantitative dynamic contrast-enhanced (DCE) MRI parameters, alone and in combination with clinico-pathologic variables, for prediction of recurrence in patients treated with NAC.Methods
Breast cancer patients treated with standard of care NAC were consented to the study. Clinico-pathologic variables [residual cancer burden (RCB), tumor type, tumor grade, ER status, progesterone receptor (PR) status, Her2 status, clinical nodal disease, stage, and age] were collected. These patients underwent research DCE-MRI exams at visit 1 (V1) - before NAC, V2 - after first NAC cycle, V3 – midpoint of NAC, and V4 - after NAC completion but prior to surgery. Axial bilateral and full-coverage breast DCE-MRI was performed using a 3T Siemens system with 14-20 s temporal resolution and ~ 10 min acquisition time. 4 Other acquisition parameters included 10o flip angle, TE/TR = 2.7/6.2 ms, 30-36 cm FOV, 320x320 in-plane matrix size, and 1.4 mm slice thickness. Tumor regions of interest (ROIs) were manually drawn by experienced radiologists on all post-contrast image slices covering the contrast-enhanced tumor, and the tumor size in the longest diameter (LD) was measured according to the RECIST guidelines. 5 Within the ROIs, the voxel DCE time-course data were subjected to the Shutter-Speed model (SSM) pharmacokinetic analyses to extract the Ktrans, ve, Kep (= Ktrans/ve), and τi (mean intracellular water lifetime) parameters. 4 The τi parameter is unique to the SSM which accounts for the cross cell membrane water exchange kinetics. 4,6 The whole tumor mean parameter value was calculated by averaging the voxel parameter values. To align with routine clinical practice of performing pre- and post-NAC MRI, only the MRI parameters obtained at V1 and V4 were used in this study for recurrence prediction. Pathologic response to NAC and RCB ranks were determined from the post-NAC resection specimens. 7Independent t-test was used to compare means of continuous variables between recurrence and no-recurrence groups, and Fisher’s exact test for the distribution of categorical variables. Univariate logistic regression C statistics value, which is equivalent to the area under the ROC curve (ROC AUC), was reported for prediction of recurrence using MRI parameters. To mitigate potential bias caused by rare events and accommodate quasi-complete separation in the data, Firth logistic regression (FLR) was used to build multivariate prediction models for recurrence. Clinical variables with a p-value < 0.2 from the univariate analysis (RCB, stage, and age) were used to build the initial FLR model, followed by an automated stepwise model selection procedure using AIC (Akaike information criterion) to select a parsimonious main effect only model that accomplished a desired level of prediction without over-fitting the current data. The final model included RCB and age. Then, MRI parameters were added to this model one at a time to examine the predictive performance presented as ROC AUC.
Results
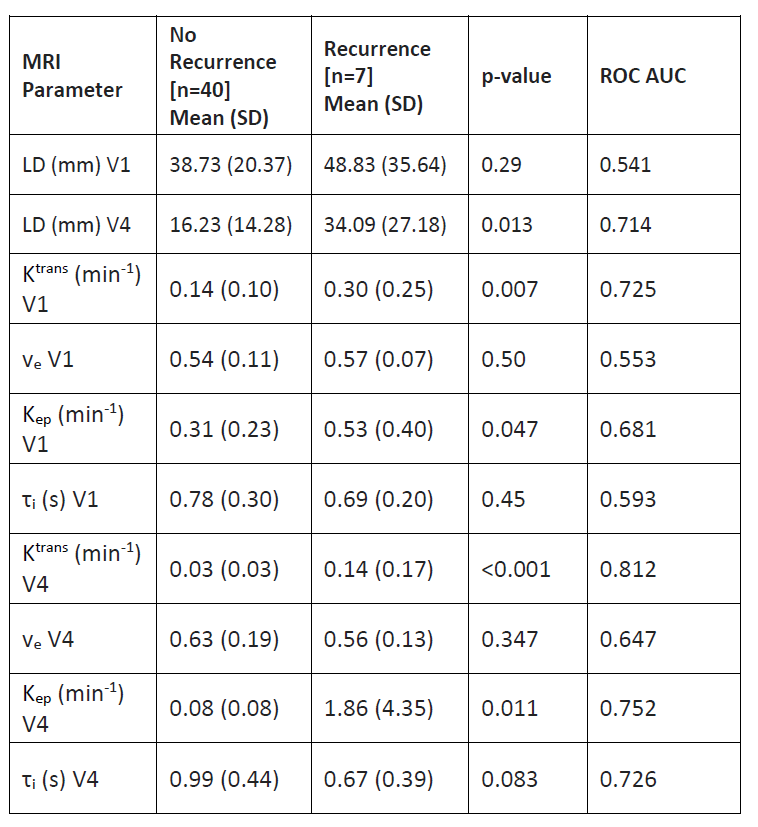
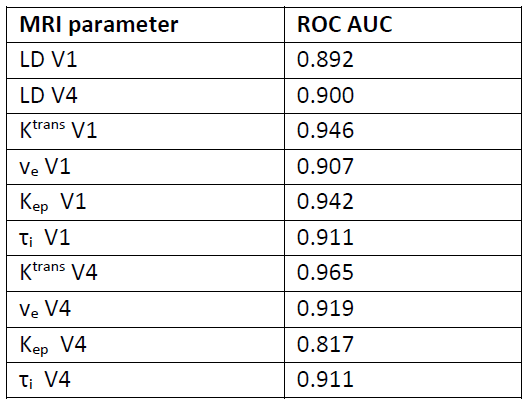
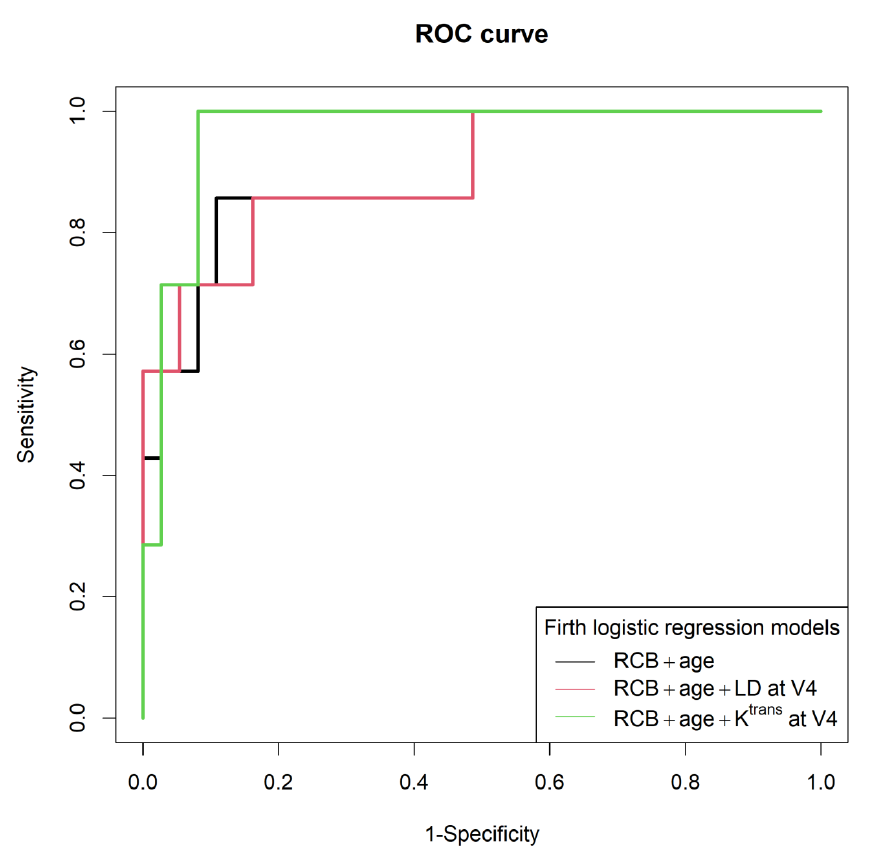
Among 47 participating patients, 7 patients experienced a recurrence. Table 1 lists the mean and SD values of the MRI parameters for the recurrence and no-recurrence groups, as well as the ROC AUC values for prediction of recurrence. At V4 (post-NAC), the quantitative DCE-MRI parameters of Ktrans, Kep, and τi outperformed LD in prediction of recurrence. It is interesting to note that, at V1 (pre-NAC), Ktrans showed good predictive performance with an AUC > 0.7. The final FLR model with the two clinical variables of RCB and age had an ROC AUC of 0.900. Table 2 summarizes the ROC AUC values when each MRI parameter was added to this model. While the addition of LD did not improve predictive performances, several quantitative DCE parameters at both V1 and V4 provided added value on top of the clinical variables for prediction of recurrence. As an example, Figure 1 shows the ROC curves for clinical variables only and additions of LD and Ktrans at V4, respectively.Discussion and Conclusion
Our study shows that quantitative DCE-MRI parameters, whether alone or in combination with clinico-pathologic variables, outperformed tumor size measurement by conventional imaging in prediction of breast cancer recurrence following NAC. Quantitative DCE parameters provided added value in predictive performance when combined with clinico-pathologic variables. Patients with recurrence tended to have higher perfusion/permeability as measured by Ktrans and Kep, and higher metabolic activity as measured by τi6 both pre- and post-NAC. Improved predictive accuracy for recurrence using clinical data and DCE-MRI parameters may allow clinicians to adjust therapy regimens to augment response to NAC and reduce recurrence risk. This study is limited by the small sample size and the moderate imbalance of the small recurrence group.Acknowledgements
NIH grant R01 CA248192References
1. Caudle AS, Yu T-K, Tucker SL, Bedrosian I, Litton JK, Gonzalez-Angulo AM, et al. Local-regional control according to surrogate markers of breast cancer subtypes and response to neoadjuvant chemotherapy in breast cancer patients undergoing breast conserving therapy. Breast Cancer Res. 2012 May 23;14(3):R83.
2. Asselain B, Barlow W, Bartlett J, Bergh J, Bergsten-Nordström E, Bliss J, et al. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018 Jan 1;19(1):27–39.
3. Chou H-H, Chung W-S, Ding R-Y, Kuo W-L, Yu C-C, Tsai H-P, et al. Factors affecting locoregional recurrence in breast cancer patients undergoing surgery following neoadjuvant treatment. BMC Surg. 2021 Mar 23;21(1):160.
4. Tudorica A, Oh KY, Chui SY-C, Roy N, Troxell ML, Naik A, et al. Early Prediction and Evaluation of Breast Cancer Response to Neoadjuvant Chemotherapy Using Quantitative DCE-MRI. Transl Oncol. 2016 Feb;9(1):8–17.
5. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer Oxf Engl 1990. 2009 Jan;45(2):228–47.
6. Springer CS, Li X, Tudorica LA, Oh KY, Roy N, Chui SY-C, et al. Intratumor mapping of intracellular water lifetime: metabolic images of breast cancer? NMR Biomed. 2014 Jul;27(7):760–73.
7. Symmans WF, Peintinger F, Hatzis C, Rajan R, Kuerer H, Valero V, et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J Clin Oncol Off J Am Soc Clin Oncol. 2007 Oct 1;25(28):4414–22.
Figures