4013
Evaluation of the Combined Deep Learning Networks Using Mask R-CNN and ResNet50 Classification for Detection and Diagnosis of Breast Cancer on MRI1Department of Radiological Sciences, University of California, Irvine, CA, United States, 2Department of Radiation Oncology, Rutgers-Cancer Institute of New Jersey, Robert Wood Johnson Medical School, New Brunswick, NJ, United States, 3Department of Radiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China
Synopsis
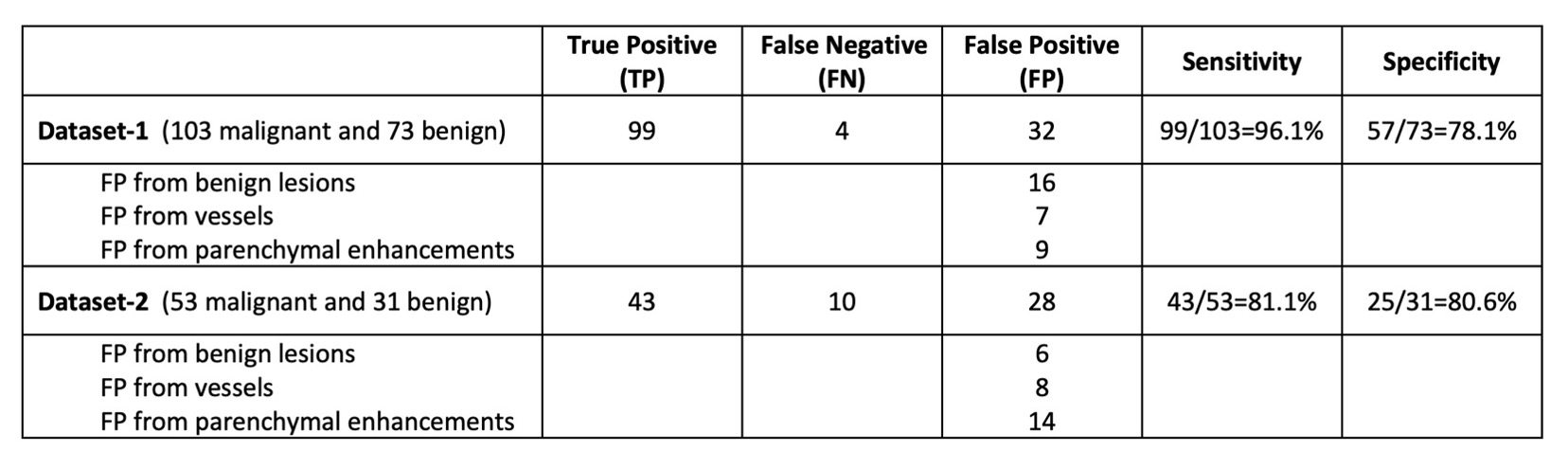
We developed two deep learning methods for breast MRI evaluation, first using Mask R-CNN for detection of suspicious areas, and then using ResNet50 for estimating the malignancy probability. These two networks were combined to test its diagnostic validity in two datasets. In Dataset-1, sensitivity=96.1% and specificity=78.1%. In Dataset-2, sensitivity=81.1% and specificity= 80.6%. We further characterized all false positives (FPs), and found other than confirmed benign lesions, FPs may come from vessels and asymmetric parenchymal enhancements, which can be further eliminated by other algorithms. The results suggest the potential of combined deep learning networks as a fully-automatic breast MRI CAD.
Introduction
Breast MRI is a well-established clinical imaging modality for diagnosis of breast cancer and screening in high-risk women. After the images are acquired, the first task is to identify suspicious abnormalities, and then to further characterize them for making the differential diagnosis of benign or malignant. Since hundreds of images were acquired, it’s challenging for radiologists to evaluate the entire dataset. Therefore, the reading is usually done with the assistance of computer-aided diagnosis (CAD) software to display important information on the workstation for evaluation. In recent years, deep learning algorithms have been applied to perform many clinical tasks, including automatic search of abnormality and diagnostic classification. We have previously developed a fully-automatic detection model using Mask Reginal-Convolutional Neural Network (R-CNN) by considering the symmetry of bilateral breasts, and achieved a high sensitivity in detecting cancers; however many enhanced areas were detected as suspicious [1]. We have also developed a diagnostic model using ResNet50 to predict the malignancy probability of the detected lesions [2]. In this study, these two networks were combined to test its diagnostic validity in clinical practice by using two different datasets to evaluate its performance. For the diagnosed false positives, we further evaluated the source of error.Methods
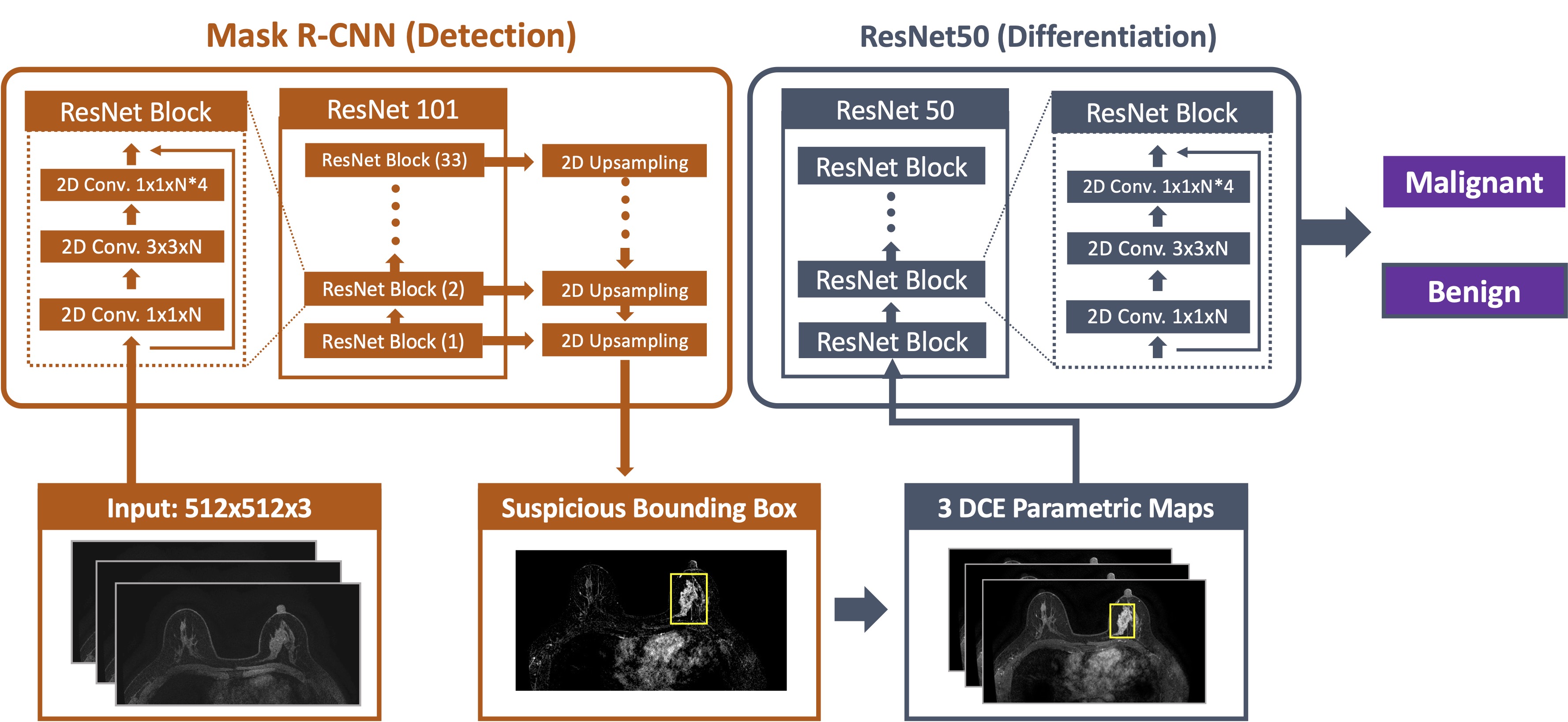
The first dataset had 176 cases, 103 cancer and 73 benign. The second dataset had 84 cases, 53 cancers and 31 benign. The MRI was performed using a GE 3.0T system. DCE was acquired using the VIBRANT sequence with 6 frames, one pre-contrast (F1) and 5 post-contrast (F2-F6). All slices were evaluated using the trained and validated Mask R-CNN framework to detect suspicious lesions. The architecture is shown in Figure 1. The ResNet101 was selected as the backbone network to build Feature Pyramid Network (FPN) and ImageNet was used as initial parameter values. The pre-contrast image, and the subtraction images of the diseased breast and the contralateral normal breast were used as inputs, where the symmetry could be used to eliminate the false detection coming from symmetric normal parenchymal enhancements. The outputs of FPN were sent to three sub-networks: bounding box regression network, object classification network, and mask network. This Mask R-CNN model was trained and tested using two different datasets [1]. After the suspicious lesions were identified, the differential diagnosis was made using three heuristic DCE parametric maps: the early wash-in signal enhancement (SE) ratio [(F2-F1)/F1]; the maximum SE ratio = [(F3-F1)/F1]; the wash-out slope [(F6-F3)/F3]. The cropped maps containing the suspicious lesion areas were put into the ResNet50 to assess the malignancy probability, by using a previously trained model [2]. Then, for the lesions falsely diagnosed as cancers, we further determined whether they were from enhanced vessels, normal parenchymal tissues, or histologically confirmed benign lesions.Results
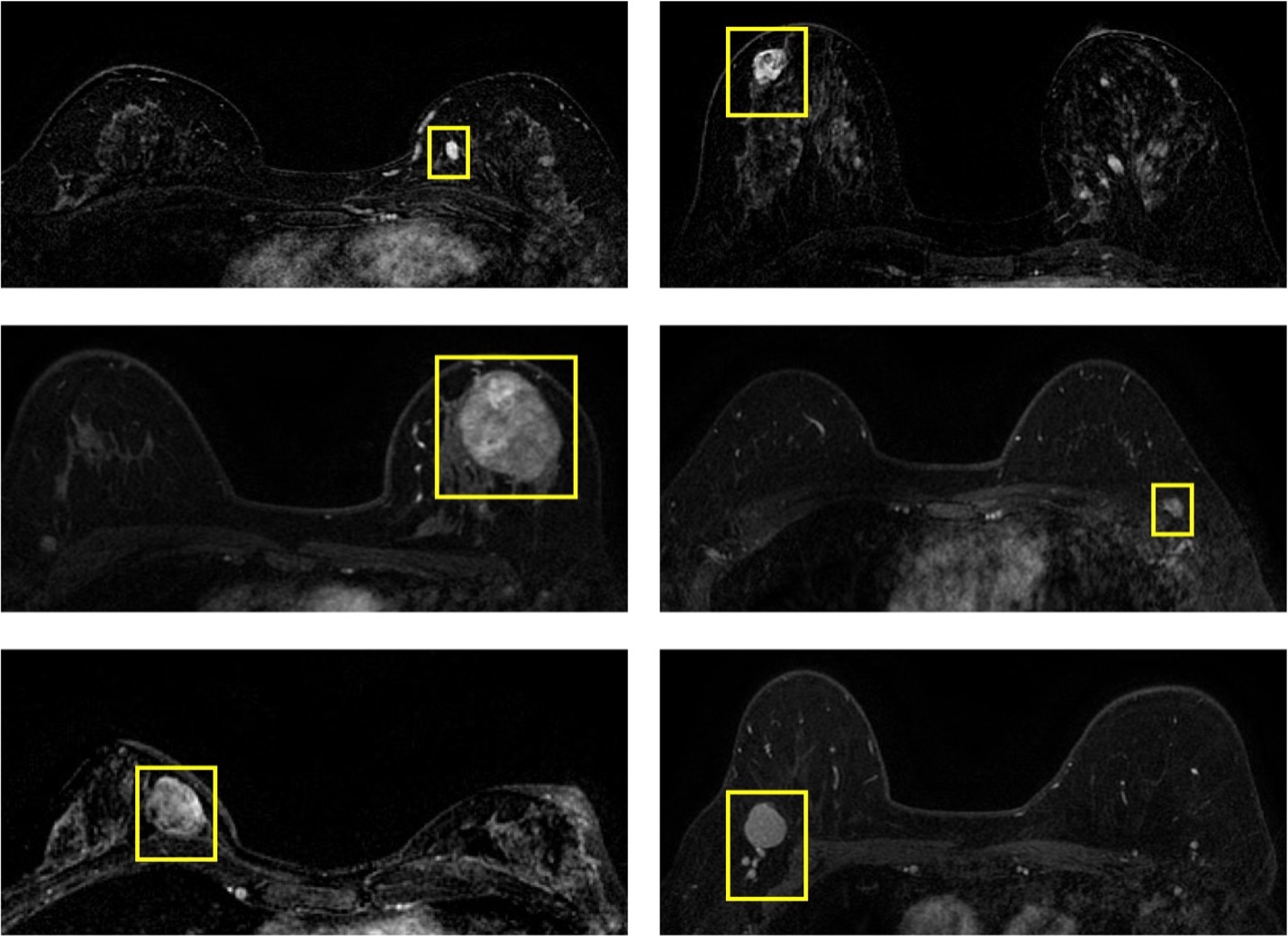
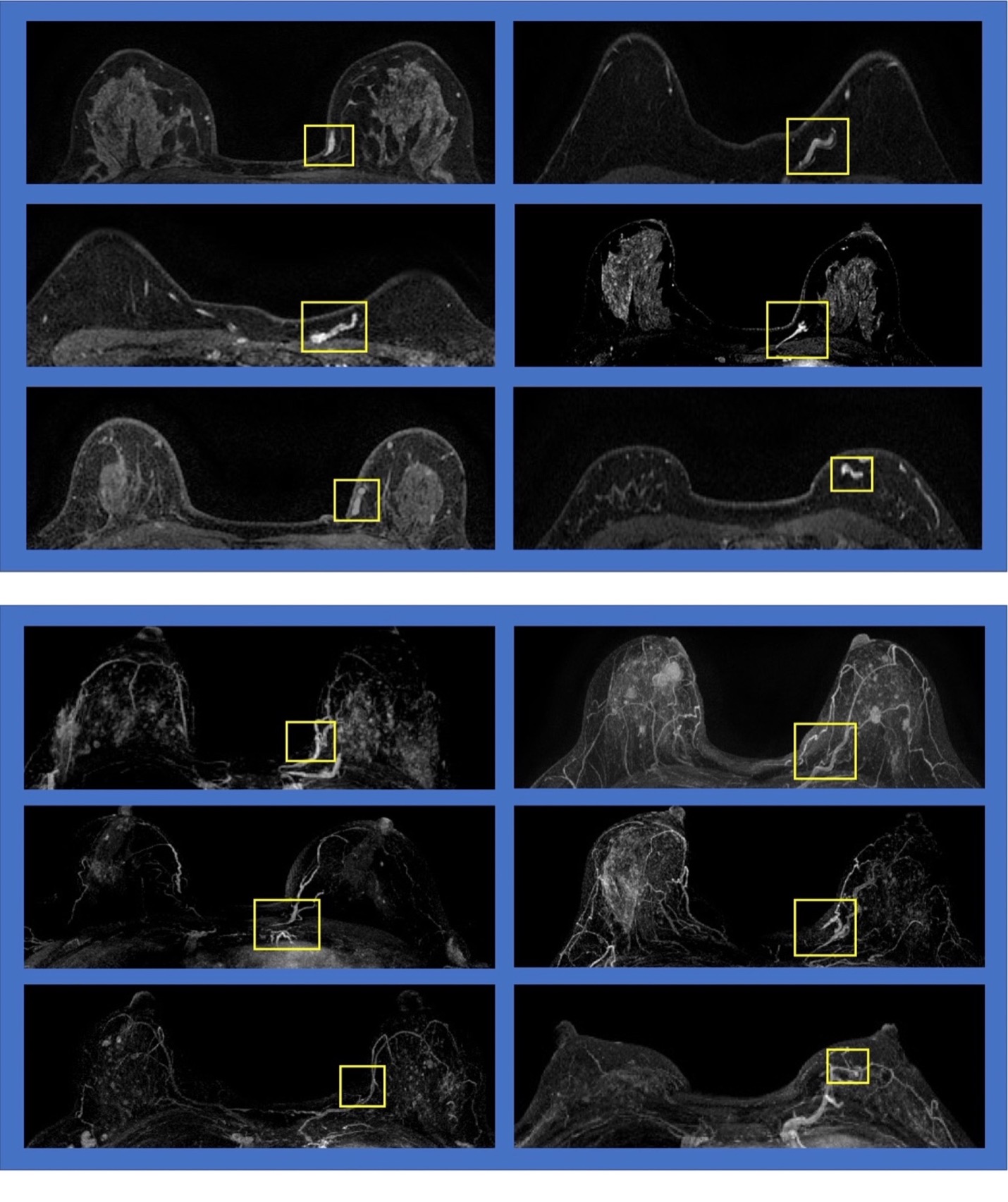
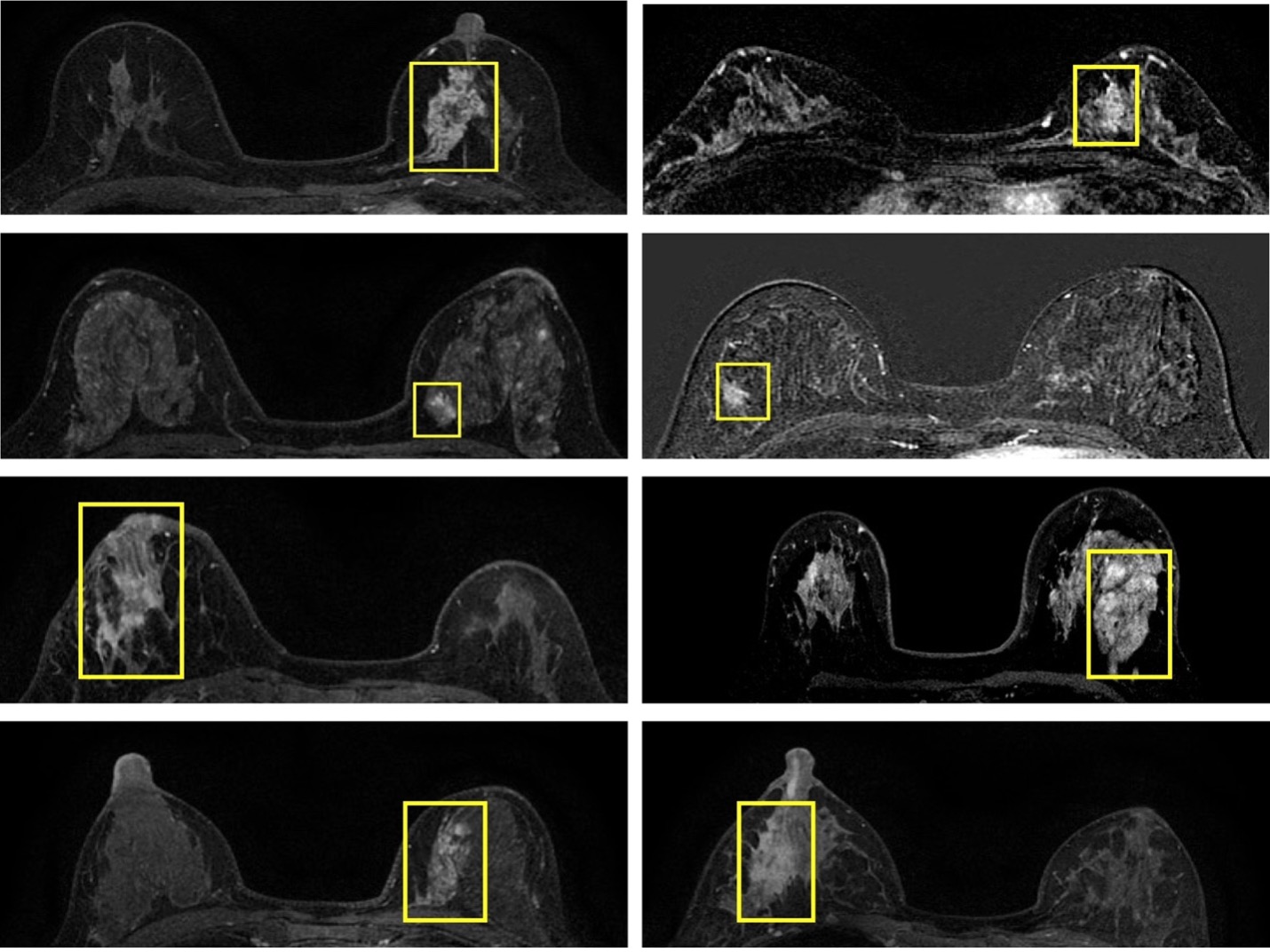
The results are summarized in Table 1. Dataset-1 has 103 confirmed cancers, and 99 of them were correctly diagnosed and 4 were missed, with a sensitivity of 96.1%. Of the 73 confirmed benign lesions, only 16 were diagnosed as false positives, with a specificity of 78.1%. Several examples of mis-classified benign lesions are shown in Figure 2. Other than these pathologically confirmed lesions, there were 16 areas diagnosed as false positives, including 7 from vessels and 9 from parenchymal enhancements. Six cases of false positives from vessels are shown in Figure 3, and the vessels are confirmed to be part of the vasculature based on the corresponding maximum intensity projection (MIP). Figure 4 shows eight false positives from parenchymal enhancements, in which the obvious asymmetric enhancements are observed. Dataset-2 has 53 confirmed cancers, and of them 43 were correctly diagnosed with a sensitivity of 81.1%. Of the 31 benign lesions, only 6 were diagnosed as cancers, with a specificity of 80.6%. There were 8 false positives from vessels and 14 from parenchymal enhancements. The results suggest that the ResNet50 can eliminate many enhanced areas identified by the Mask R-CNN detection algorithm.Discussion
Many studies have investigated the value of machine learning for differentiation of benign and malignant lesions. These studies mainly focused on characterization of already identified abnormal lesions. In fact, the automatic detection was a much more challenging task, especially in MRI where many images were acquired to cover the entire breast. In this study, we implemented a fully automatic deep learning method, by first applying the Mask R-CNN to search the entire set of MR images and identify suspicious lesions, and then by applying ResNet50 to further characterize the lesions and predict the diagnosis as malignant or benign. The results in two datasets suggest that a high sensitivity and a high specificity can be achieved. Although Mask R-CNN will identify many suspicious areas, the followed ResNet50 can eliminate many of them. By doing so, many identified suspicious areas will be dismissed, which can reduce the false positives while maintaining a high true positive detection rate. For the false positives coming from vessels and the asymmetric parenchymal enhancements, these can be quickly discarded by radiologists, or by using other computer algorithms according to their unique features. In conclusion, the proposed Mask R-CNN and ResNet50 has the potential to provide an automatic detection and diagnosis system for breast MRI.Acknowledgements
This work was supported in part by NIH/NCI R01 CA127927, R21 CA208938, P30 CA062203, and Foundation of Wenzhou Science & Technology Bureau (No. Y20180187 and Y20180144), Medical Health Science and Technology Project of Zhejiang Province Health Commission (No. 2019KY102).References
[1] Zhang Y, Chan S, Park VY, et al. Automatic Detection and Segmentation of Breast Cancer on MRI Using Mask R-CNN Trained on Non–Fat-Sat Images and Tested on Fat-Sat Images. Academic Radiology E-pub before print. https://doi.org/10.1016/j.acra.2020.12.001
[2] Zhou J, Zhang Y, Chang KT, et al. Diagnosis of Benign and Malignant Breast Lesions on DCE-MRI by Using Radiomics and Deep Learning With Consideration of Peritumor Tissue. J Magn Reson Imaging. 2020 Mar;51(3):798-809. doi: 10.1002/jmri.26981.
Figures