3922
Deep learning-based slice resolution for improved slice coverage in abdominal T2 mapping1Electrical and Computer Engineering, University of Arizona, Tucson, AZ, United States, 2Medical Imaging, University of Arizona, Tucson, AZ, United States, 3Radiology, Houston Methodist Hospital, Houston, TX, United States, 4Biomedical Engineering, University of Arizona, Tucson, AZ, United States
Synopsis
This study presents a deep learning based technique for slice super resolution in RADTSE T2 mapping. The proposed method may be used to accelerate full liver imaging, while maintaining sufficient through-plane resolution for detection of small pathologies.
Introduction
Abdominal T2 mapping provides quantitative evaluation of tissue, which can be used for standardized assessment of pathologies (e.g., focal liver lesions).1,2 Comprehensive liver evaluation requires complete anatomical coverage, at sufficiently high in-plane and through-plane resolution for accurate detection of small lesions. Radial turbo spin-echo methods have been proposed for motion robust high-resolution (in-plane) abdominal T2 mapping, allowing acquisition of up to 11 slices within a 18s breath hold period (BHP).3-5 To achieve full liver coverage (150mm) within a BHP, a slice thickness of 13.6mm is required. Acquisition at such low through-plane resolution would inhibit identification of most liver and pathological structures. As a result, data must be acquired over multiple BHPs (3-4) using a higher (4-6mm) through-plane resolution.Recently, deep learning (DL) techniques have been proposed for MRI slice super-resolution (SR).6-9 These techniques rely on exploitation of spatial redundancies to recover high-frequency signal components which were not acquired during original signal acquisition. In this study, we propose an accelerated T2 mapping framework, which utilizes DL SR to recover structural information lost due to slice undersampling. This will allow a decreased through-plane resolution to be used during acquisitions, allowing increased anatomical coverage in fewer BHPs.
Methods
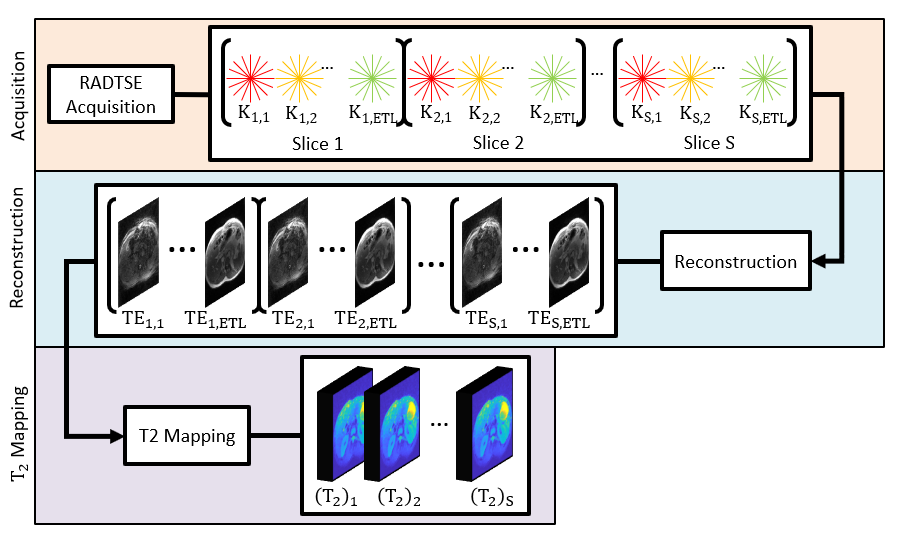
Figure 1 summarizes the RADTSE T2 framework. For each slice, k-space radial views are acquired at each echo time (TE) for the full echo train lengths (ETL). After all TRs complete, the groups of radial lines ($$$K_{s,n}$$$) at each TE are used in reconstruction to obtain a corresponding set of TE images ($$$I_{s,n}$$$). T2 maps are then generated form the TE images.In traditional DL based SR, a high-resolution ground truth is made available, which is deteriorated through low-pass filtering and/or decimation to simulate a low-resolution counterpart. The model is then trained mapping between the low-resolution and original image. For abdominal T2 mapping slice SR, this approach would require training data with high through-plane resolution for ground truth. Unfortunately, acquisition of high through-plane resolution T2 mapping data is difficult, making this approach infeasible for abdominal imaging. As a result, we adopt the approach proposed by Zhao et al, where a model is trained to perform SR on simulated through-plane data produced using in-plane data, then is applied directly on through-plane data during deployment. While Zhao et al considers training individual models for individual acquired volumes, here we consider an offline approach where a single SR model is trained using many volumes.
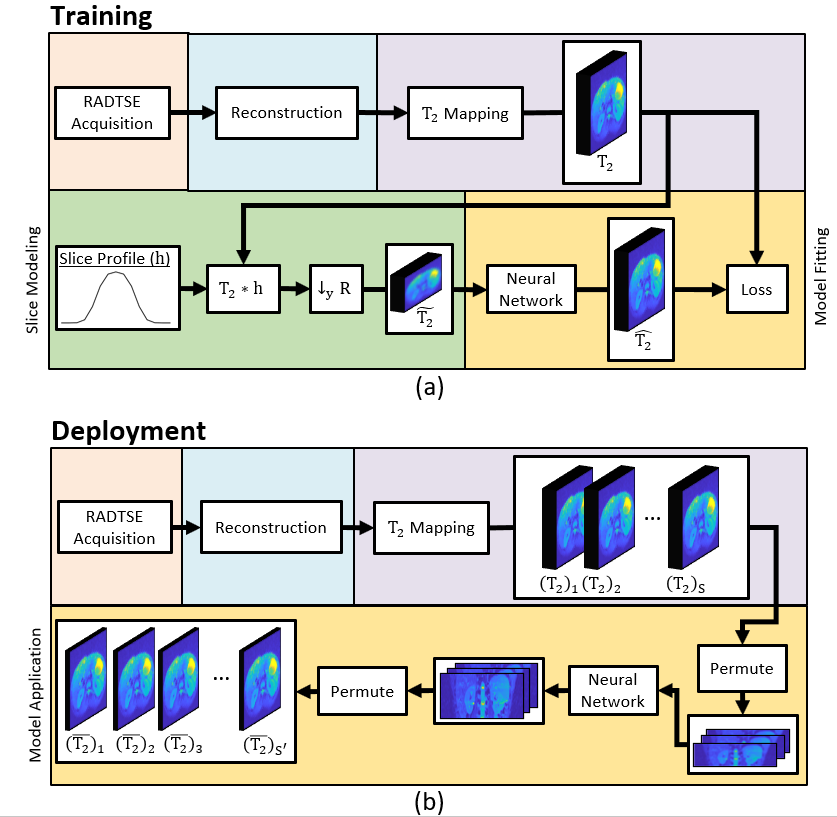
The proposed DL framework is presented in Figure 2. For training, a set of T2 maps are acquired using the pipeline outlined in Figure 1. For each acquired T2 map, slice modeling is performed to produce synthetic through-plane images. First, the row dimension is filtered using the slice profile filter $$$h$$$, which is designed to match the acquired through-plane resolution and simulates slice crosstalk due to non-ideal slice-selective excitation. The result is then downsampled by a factor $$$R$$$ (the through to in-lane resolution ratio) in the row dimension. The resulting T2-tilde is a synthetic though-plane image, with low-resolution in the row dimension and high-resolution in the column dimension. A model is then trained to estimate the original T2 map from T2-tilde.
Training data was acquired from imaging 68 subjects using RADTSE with TR=2500ms, echo spacing=7.3ms, ETL=32, base resolution=256, FOV=400mm, slice thickness=8mm, slices=21 and radial views=192. TE images are obtained using a locally low-ranked iterative reconstruction.10 T2 maps are generated from TE images using a dictionary based on the SEPG model.11 We use EDSR12 with 1D pixel shuffling to perform SR only in a single dimension, with R=5.12. This eliminates the need to train an additional anti-aliasing model as described in Zhao et al, reducing the complexity of the model. The network was trained for 200 epochs using a fixed learning rate of 1e-4. Training is performed on 21x21 pixel patches. Data is augmented using random rotation and flipping. In addition, we train a separate model for SR on composite images produced by combining all TE images. We perform both qualitative and quantitative evaluation of each trained model. For quantitative evaluation we use PSNR, SSIM and S3 shapress.13
Results and Discussion
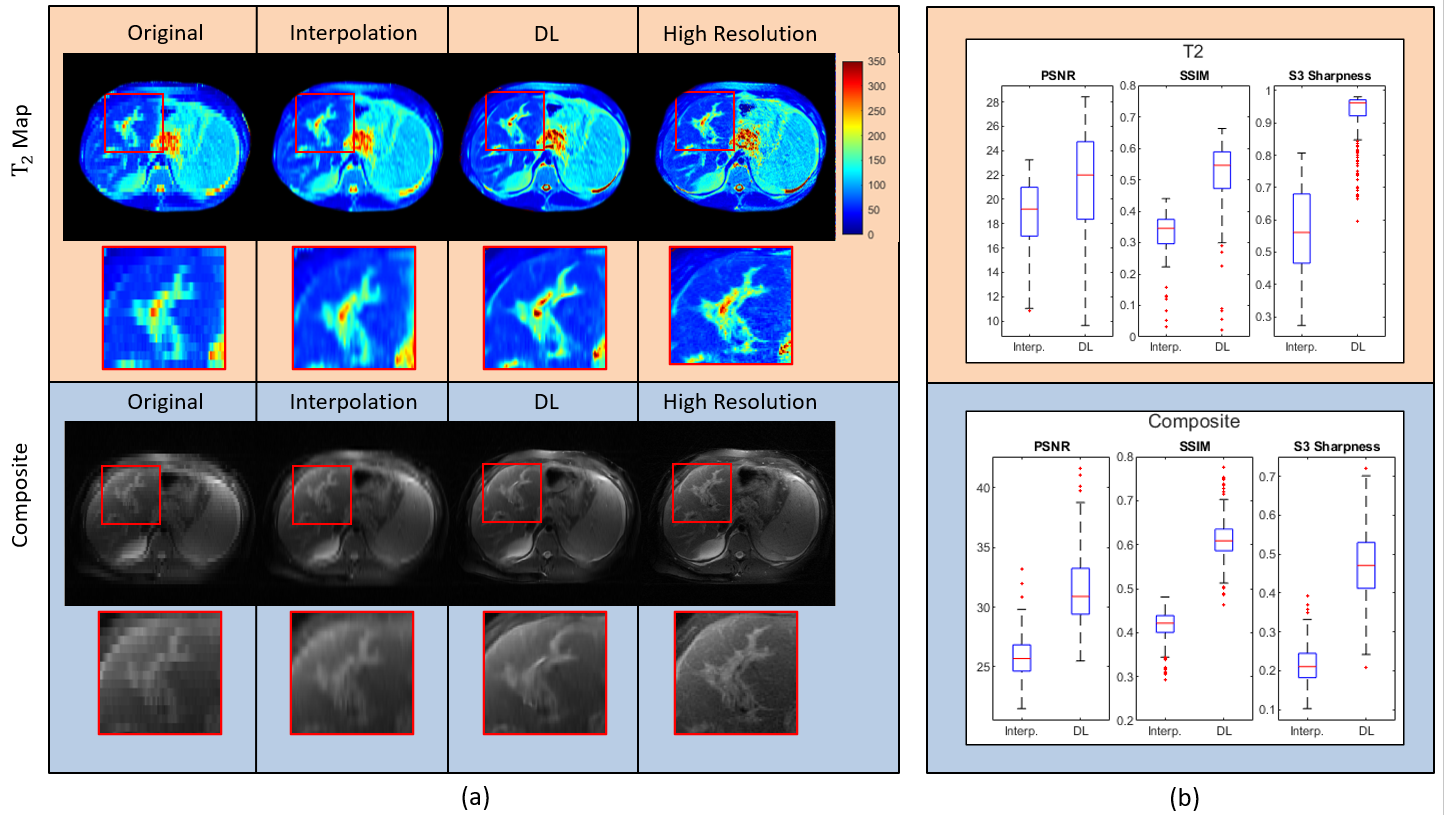
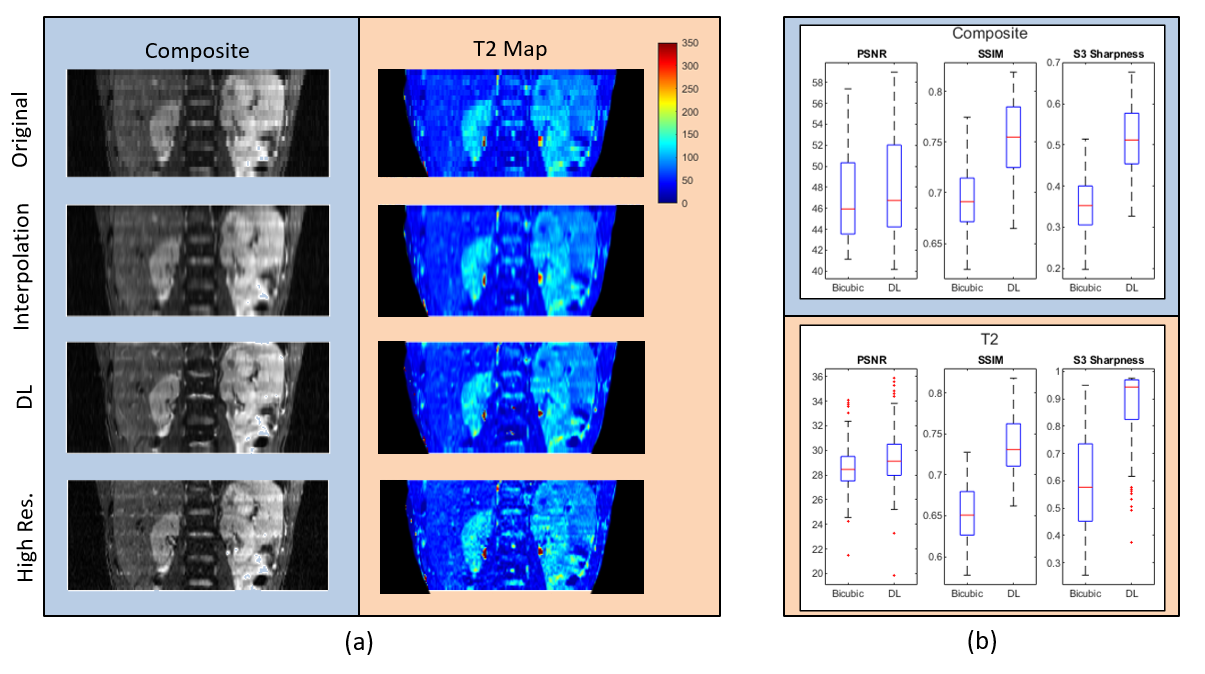
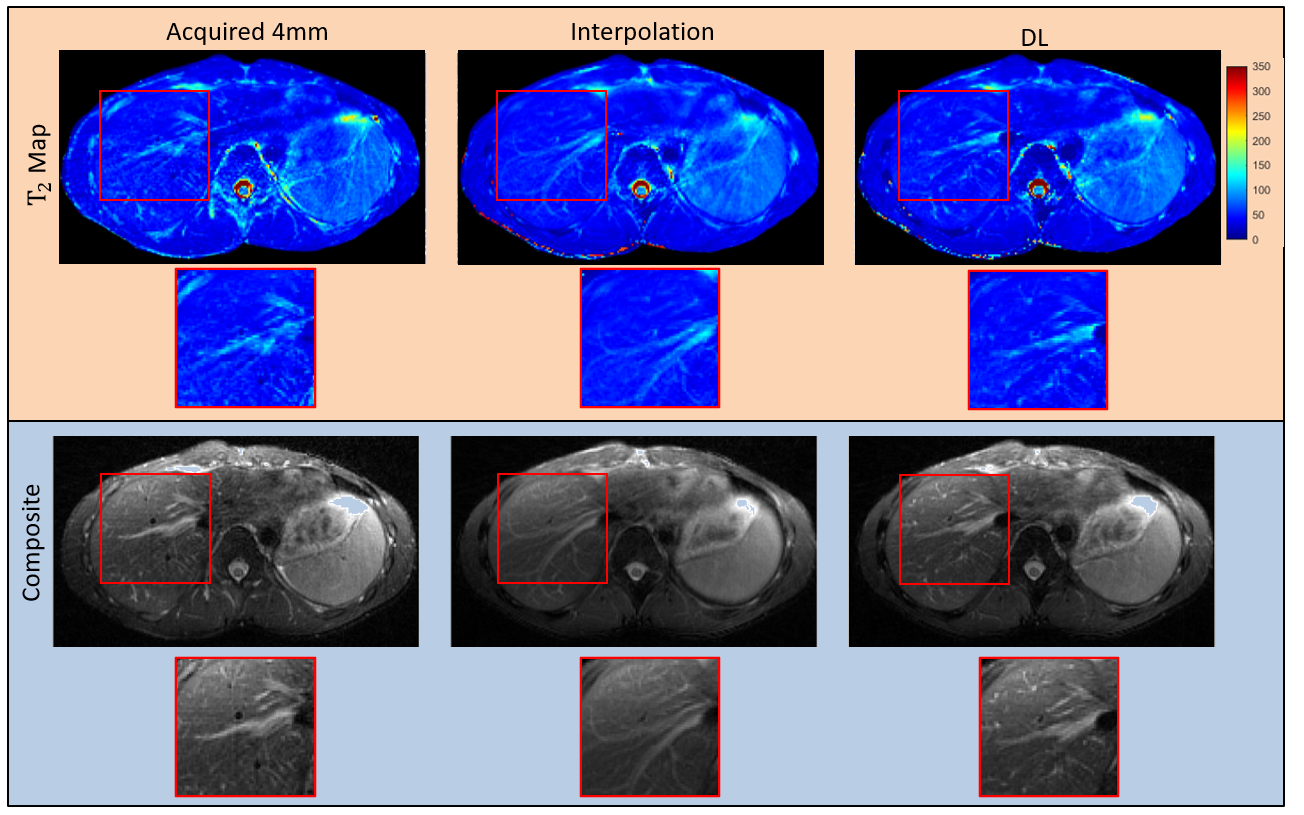
Figure 3 demonstrates SR performance of the trained models when applied to synthetic through-plane images. Here the DL model applied to T2 maps achieved a 13.2%, 37.3% and 73.2% improvement in PSNR, SSIM and S3 sharpness, respectively. Figure 4 shows the performance of the trained models on through-plane data. Here, a 4mm acquired volume was retrospectively filtered and downsampled to produce an 8mm volume, and the trained model was applied across coronal slices. The DL model again outperformed interpolation with a 2.7%, 13% and 54% improvement in PSNR, SSIM and S3-sharpness, respectively. Figure 5 provides qualitative assessment on true 8mm acquired data. Each slice gives the image produced at the same anatomical location using each method. Note that DL can reproduce structures at the correct anatomical location, while interpolation incorrectly reproduces vascular structures in the liver.Conclusions
We presented a DL based SR method for improving volumetric imaging in abdominal T2 mapping. The method has the potential to accelerate full liver parametric imaging, while maintaining adequate through-plane resolution for assessment of small pathological structures.Acknowledgements
We would like to acknowledge grant support from NIH (CA245920 and CA245920S1), the Arizona Biomedical Research Commission (CTR056039), and the Technology and Research Initiative Fund Technology and Research Initiative Fund (TRIF).References
1. Farraher S, Jara H, Chang K, Ozonoff A, Soto J. Differentiation of hepatocellular carcinoma and hepatic metastasis from cysts and hemangiomas with calculated T2 relaxation times and the T1/T2 relaxation times ratio. J Magn Reson Imaging 2006;24(6):1333-1341.
2. Cieszanowski A, Anysz-Grodzicka A, Szeszkowski W, et al. Characterization of focal liver lesions using quantitative techniques: Comparison of apparent diffusion coefcient values and T2 relaxation times. Eur Radiol 2012;22(11):2514-2524.
3. Altbach M, Outwater E, Trouard T, et al. Radial fast spin-echo method for T2-weighted imaging and T2 mapping of the liver. Journal of Magnetic Resonance Imaging, 16(2):179–189, 2002.
4. Altbach M, Bilgin A, Li Z, et al. Processing of radial fast spin-echo data for obtaining T2 estimates from a single k-space dataset. Magnetic Resonance in Medicine, 54(3):549–559, 2005.
5. Keerthivasan M, Galons J, Johnson K, et al. Abdominal T2-Weighted Imaging and T2 Mapping Using a Variable Flip Angle Radial Turbo Spin-Echo Technique. J Magn Reson Imaging (2021), https://doi.org/10.1002/jmri.27825
6. Zhao C, Dewey BE, Pham DL, et al. SMORE: A Self-Supervised Anti-Aliasing and Super-Resolution Algorithm for MRI Using Deep Learning. IEEE Trans Med Imaging. 2021 Mar;40(3):805-817. doi: 10.1109/TMI.2020.3037187. Epub 2021 Mar 2. PMID: 33170776; PMCID: PMC8053388.
7. Jog A, Carass A, Prince L. Self super-resolution for magnetic resonance images, in Proc. Int. Conf. Med. Image Comput. Comput. Assist. Intervent. Cham, Switzerland: Springer, 2016, pp. 553–560.
8. Zhao C, Carass A, Dewey B, Prince J. Self super-resolution for magnetic resonance images using deep networks, in Proc. IEEE 15th Int. Symp. Biomed. Imag. (ISBI), Apr. 2018, pp. 365–368.
9. Zhao C. A deep learning based anti-aliasing self super-resolution algorithm for MRI, in Proc. Int. Conf. Med. Image Comput. Comput. Assist. Intervent. Cham, Switzerland: Springer, 2018, pp. 100–108.
10. https://mrirecon.github.io/bart
11. Huang C, Altbach M, El Fakhri G. Pattern recognition for rapid T2 mapping with stimulated echo compensation. Magn Reson Imaging 2014;32(7):969-974
12. Lim B, Son S, Kim H, Nah S, Lee K. Enhanced deep residual networks for single image super-resolution, in Proc. IEEE Conf. Comput. Vis. Pattern Recognit. Workshops (CVPRW), Jul. 2017, pp. 1132–1140.
13. Vu C, Chandler D. S3: A spectral and spatial sharpness measure, in Proc. 1st Int. Conf. Adv. Multimedia, Jul. 2009,pp. 37–43.
Figures