3887
A fixel-based analysis of white matter alterations in patients with acute mild traumatic brain injury1Center for Advanced Imaging Research, University of Maryland Baltimore, Baltimore, MD, United States, 2Department of Diagnostic Radiology & Nuclear Medicine, University of Maryland Baltimore, Baltimore, MD, United States
Synopsis
Mild traumatic brain injury (mTBI) accounts for the majority of head injuries and is often associated with physical, cognitive, and effective deficits. We used fixel-based analysis (FBA) to investigate the white matter (WM) structural alterations in acute mTBI patients. Three fixel-based metrics were used: fibre density (FD), fibre-bundle cross-section area (FC) and a combination of FD and FC (FDC). We found out that mTBI patients demonstrated reduced FC and FDC in multiple WM tracts and it may suggest that FBA can be used to detect subtle WM changes following mild injuries.
Introduction
Mild traumatic brain injury (mTBI) accounts for roughly 75% of the 1.5 million head injuries reported annually in the United States [1] and has been found to be associated with physical, cognitive, and affective impairment. Diffusion axonal injury (DAI) is thought to be responsible for much of the observed deficits [2]. Diffusion tensor imaging have been used to assess WM abnormality following mTBI [3]. However, DTI can be challenging particularly when dealing with voxels that contain crossing fiber tracts. Recently, a novel framework, fixel-based analysis (FBA), was proposed for fiber-specific statistical analysis of diffusion MRI data which addressed this limitation. The FBA provides three fixel-based quantitative measures: fibre density (FD) for tissue microstructure; fibre-bundle cross-section area (FC) for tissue macro-structure; and a combined FD and FC (FDC) for both micro- and macro-structure. In this study, we applied FBA to investigate the white matter micro- and macro-structural alterations in patients with mTBI at acute stage.Methods
A cohort of 57 patients with mTBI at acute stage and 35 age-matched healthy controls (HCs) were retrospectively examined. The multi-shell diffusion MRI (dMRI) were performed on a 3T Siemens Tim Trio Scanner using the following parameters: TR = 6000 ms, TE = 93 ms; voxel size = 2.7 x 2.7 x 2.7 mm3; FOV = 22 x 23 cm2, 3 consecutive volumes at b-value = 0 and interleaved with other two b-values, 30 gradient directions at both b = 1000 s/mm2 and b = 2000 s/mm2 with two repetitions. Total acquisition time was about 13 minutes for total of 132 volumes. All DWI data preprocessing and analysis were implemented from the recommended FBA pipeline in MRTrix 3 (http://www.mrtrix.org) [4]. Pre-processing included denoising [5], head motion and eddy-current distortion and susceptibility correction [6], and bias field correction. The DWI images were then up-sampled to a voxel-size of 1.25 mm in all directions [7]. Individual fiber response functions for WM, GM and CSF were first estimated [7] and were subsequently averaged across participants to generate a group-level response function. Multi-shell multi-tissue constrained spherical deconvolution (MSMT-CSD) was performed for each patient to obtain WM fiber orientation distribution (FOD) map. A study-specific FOD template were created using both linear and nonlinear registration of individual FOD images from 20 mild TBI patients and 20 HCs. Individual FOD images for all participants were then nonlinearly registered to this template and segmented to produce a set of discrete fixels. For each participant, three fixel-based metrics (FD, FC and FDC) across all WM fixels were then calculated [4]. We also generated a whole-brain tractogram using probabilistic tractography on the population template. To compare the differences in FD, FC, and FDC at each WM fixel between mTBI and HCs, we used a general linear model (GLM) with controlling covariates of age and sex. Based on one million streamlines from the whole brain tractogram, we performed connectivity-based smoothing and statistical inference using connectivity-based fixel enhancement (CFE) [4]. Family-wise error (FWE)-corrected p-values were then computed for each fixel using non-parametric permutation testing over 5,000 permutations.Results
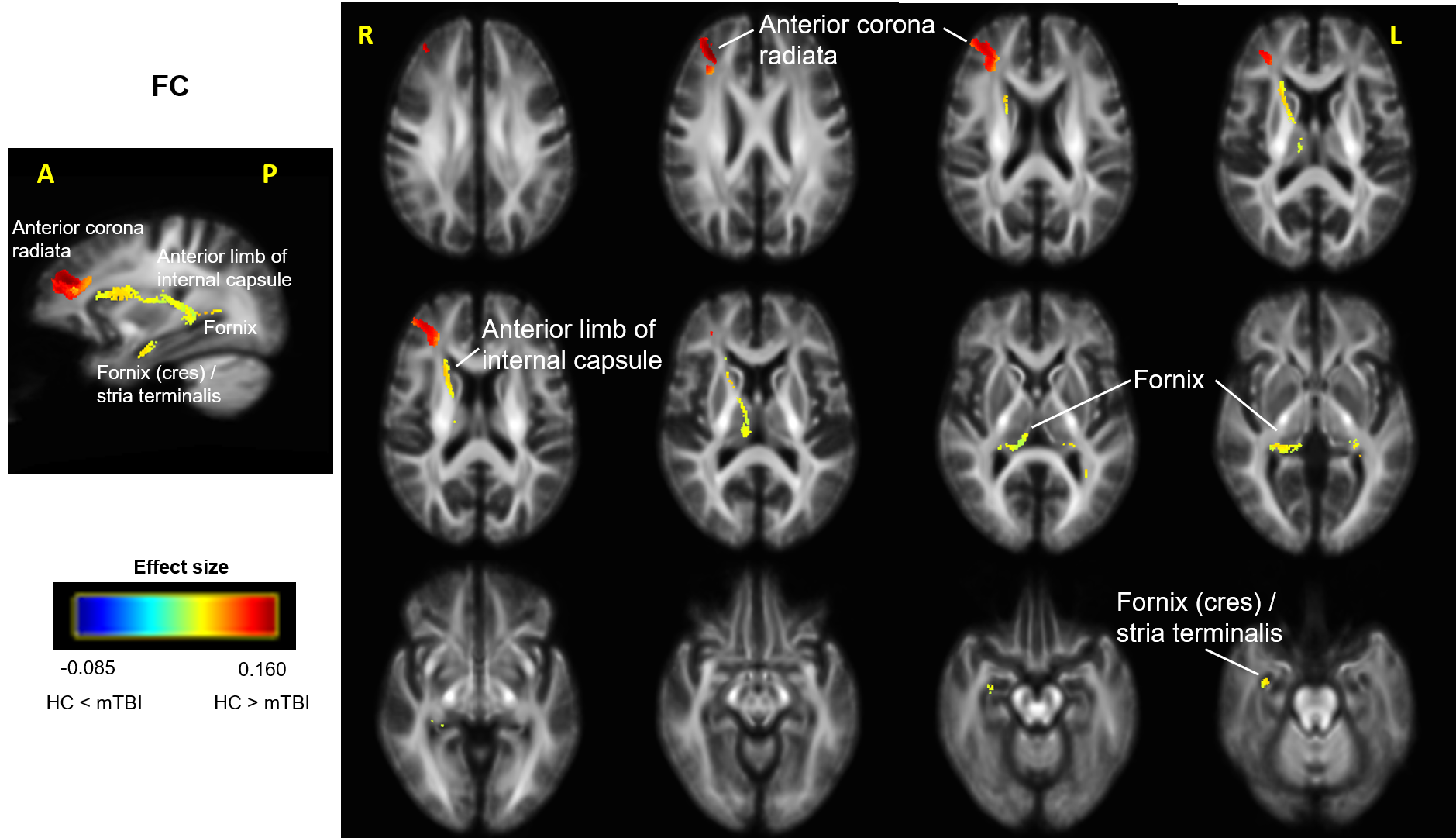
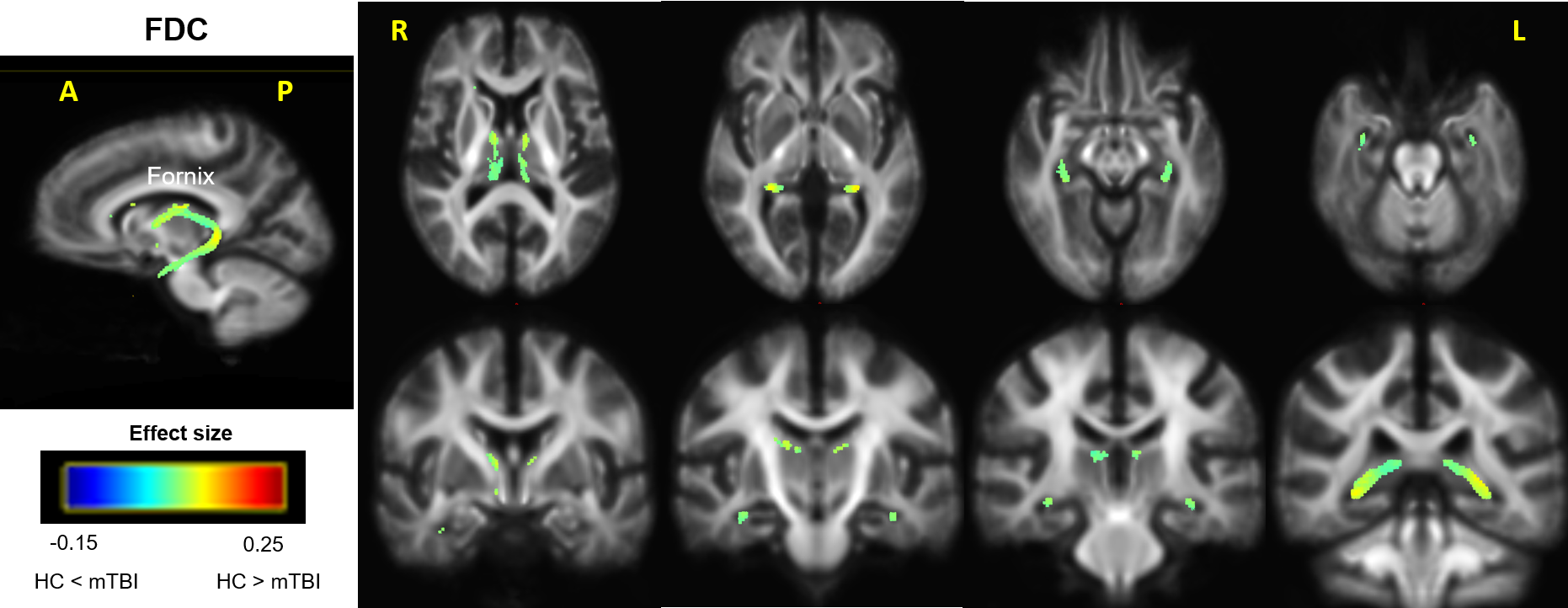
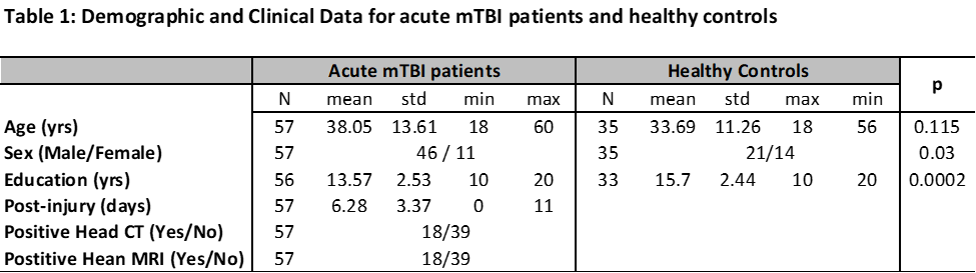
Table 1 shows that information of all patients and controls. The mTBI group had 46 males/11 females; age of 38.05 ± 13.61 and age range of 18 ~ 60 years old; GCS of 15 at acute stage (post injury days: 6.28 ± 3.37, range of 0 ~ 11 days). Only 18 out of 57 had clinically positive CT and positive MRI. The 35 age-matched HCs had 21 males/14 females; age of 33.69 ± 11.26 and age range of 18 ~ 56 years old. In this study, we observed that acute mild TBI patients had significant change in FC and FDC (p < 0.05, FWE-corrected) whereas no significant changes in FD. Figure 1 shows streamline segments associated with fixels demonstrating significant reduced FC in patients with acute mTBI. As shown in Figure 1, deceased FC was observed in the white matter fiber pathways of right anterior corona radiate, right anterior limb of internal capsule, bilateral fornix, and right fornix cres/stria terminalis in the mTBI group. Figure 2 shows streamline segments associated with fixels demonstrating significant reduced FDC in bilateral fornix fiber in patients with mild TBI. We did not observe significant micro-structural FD changes in patients with mild TBI.Discussion
In this study, we used FBA to investigate micro- and macro-structural changes in WM tracts of patients with mTBI compared with HCs. Our results showed that the mTBI patients demonstrated significantly reduced FC and FDC in multiple WM tracts, including corona radiate, internal capsule, and fornix. These regions are consistent with previous DTI studies, which report that mTBI is associated with altered WM in corpus callosum, fornix, superior longitudinal fasciculus, thalamic radiations, external and internal capsule, cingulum, and corona radiate [3]. It’s interesting to note that TBSS analysis of the same dMRI data resulted in no significant difference in FA and MD across the whole. These findings may suggest that the FBA can be more sensitive to detect subtle WM changes following mild injuries. Future work will be conducted to correlate the fixel-wise metrics with behavioral and clinical data to understand the underlying neurophysiological mechanism of mTBI.Acknowledgements
The study was conducted at University of Maryland School of Medicine Center for Innovative Biomedical Resources, Translational Research in Imaging @ Maryland (CTRIM) – Baltimore, Maryland. The study is supported by NIH under grant 5R01NS105503.References
1. Bazarian, J.J., et al., Mild traumatic brain injury in the United States, 1998--2000. Brain Inj, 2005. 19(2): p. 85-91.
2. Narayana, P.A., White matter changes in patients with mild traumatic brain injury: MRI perspective. Concussion, 2017. 2(2): p. CNC35.
3. Rutgers, D.R., et al., White matter abnormalities in mild traumatic brain injury: a diffusion tensor imaging study. AJNR Am J Neuroradiol, 2008. 29(3): p. 514-9.
4. Raffelt, D.A., et al., Investigating white matter fibre density and morphology using fixel-based analysis. Neuroimage, 2017. 144(Pt A): p. 58-73.
5. Veraart, J., et al., Denoising of diffusion MRI using random matrix theory. Neuroimage, 2016. 142: p. 394-406.
6. Andersson, J.L.R. and S.N. Sotiropoulos, An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage, 2016. 125: p. 1063-1078.
7. Tournier, J.D., et al., MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. Neuroimage, 2019. 202: p. 116137.
Figures