3877
Exploring the Application of Compressed-SENSE Accelerated Fast MR Based Bone Imaging Method in CVJ Anomalies: Preliminary Experience1Neuroimaging and interventional radiology, NIMHANS, Bangalore, India, 2Neurosurgery, NIMHANS, Bangalore, India, 3Philips India Ltd, Bangalore, India
Synopsis
Imaging analysis of craniovertebral junction anomalies comprises of bony, ligament, vascular and spinal cord evaluation. MDCT falls short in the evaluation of the latter while conventional MRI does not offer optimal bone resolution. Novel Compressed SENSE accelerated Fast field echo resembling a CT using restricted echo-spacing (CS-FRACTURE) technique is a bid to overcome this shortcoming in routine clinical setup and we aim to explore the same.
Introduction
Abnormalities of the cranio-vertebral junction (CVJ) Craniovertebral junction (CVJ) anomalies are well-recognized causes of myelopathy. Craniovertebral junctional anomalies are challenging to treat surgically, and preoperative information regarding the osseous abnormalities, course of the vertebral arteries, size of the pedicles, and location of the transverse foramina is invaluable to surgeons operating on these challenging cases. While MDCT is considered the sine qua non for analysis of bony abnormalities however due suboptimal soft tissue/ligament resolution -cord abnormalities cannot be assessed. This makes MRI an important adjunct investigation for the evaluation of craniovertebral junction. Additionally dynamic scans are often performed to make the diagnosis of atlanto-axial dislocation (AAD). CT angiography is further required to determine the exact course of the vertebral arteries. Most importantly CT is associated with significant exposure to ionizing radiation.FRACTURE (FFE Resembling A CT Using Restricted Echo-spacing) is a novel MRI technique which gives bone like images which are visibly comparable to CT contrast. This technique has been utilized for the evaluation of bone fractures. We aim to describe with illustrations the application of Compressed-SENSE accelerated FRACTURE (CS-FRACTURE) technique for evaluation of subjects with CVJ anomalies.
Materials and methods
A prospective recruitment of 5 cases with suspected CVJ anomalies was done with concurrent evaluation on CT and MRI.Imaging Protocol
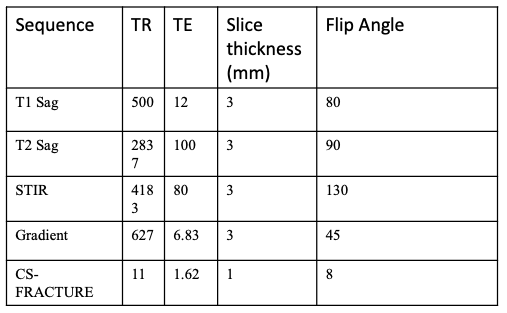
CT imaging was performed at a 128 slice scanner with the following protocol parameters : 120 Kv, 106 mAs Pitch factor 0.8 reformatted on 1mm slice thickness utilizing bone specific kernel.MR imaging was obtained on 3.0T (Ingenia 3.0 T CX; Philips Healthcare,n=6) using 32 channel coils. The routinely acquired sequences are summarised in Table I.
Additionally, MR based bone imaging sequence CS-FRACTURE which is a high resolution 3D fast field echo utilizing multiple echoes with an in-phase echo-spacing followed by additional post-processing with image algebra was added. In this study, CS-FRACTURE used optimised Compressed-SENSE factor 12 that resulted in only 2.5 minutes for data acquisition.
By virtue of optimal echo time utilisation only at in-phase intervals minimisation of the chemical shift between fat and water is achieved. This thereby allows accentuation of the T2 decay of bone while still preserving the signal from other tissues. The high resolution also aids in containing the dephasing across voxels. The post-processing steps following image acquisition include an automated summation of all echoes to increase signal and the resultant image is then subtracted from the last echo followed by inversion of the window to produce an image with CT like contrast.
Image Analysis
Independent analysis of both modalities by neuroradiologist with >15 years experience blinded to both clinical data and final diagnosis was performed. The acquired datasets were subject to multiplanar reconstruction in coronal and sagittal planes. Image quality assessment was subject to diagnostic confidence, resolution and artifacts.Results
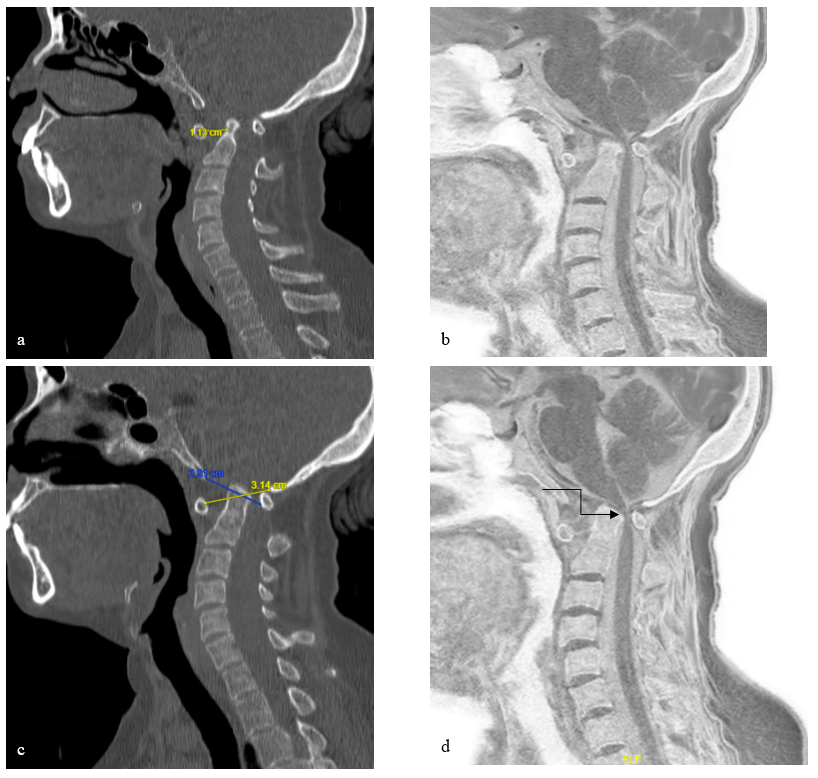
Case 1: A 55-year-old male was evaluated for restricted neck movements. MDCT revealed Power’s ratio of 1.15 inferring atlanto-occipital dislocation with increased dens, basion distance ~10mm, retroflexion of dens, narrowing at the foramen magnum and concomitant increased basion axial line interval of >12mm and increased atlanto dental interval ~11.3mm.CS-FRACTURE imaging on MRI very well demonstrated all the abnormalities as shown in figure I.
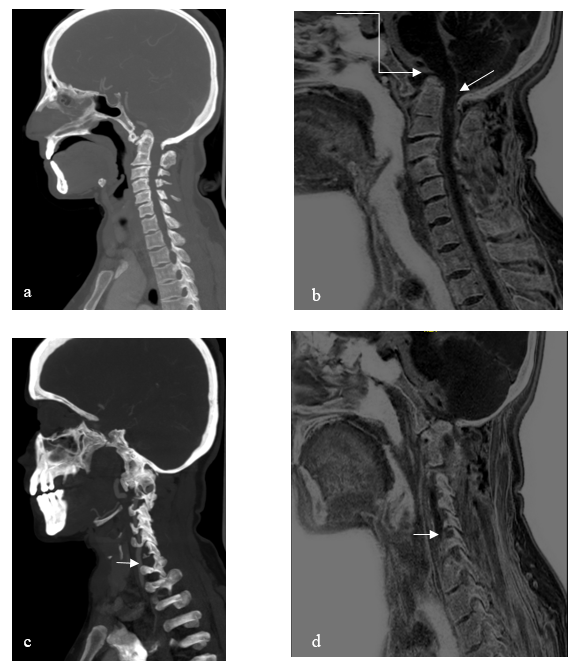
Case 2: A 40-year female previously diagnosed with CVJ was imaged for vertebral artery tracing. MDCT revealed basilar invagination with suggestion of atlantoaxial dissociation. Corroboratory flexion-extension study was also performed with CT angiography to demonstrate the course of the vertebral artery.
CS-FRACTURE bone imaging on MRI very well demonstrated the AAD, basilar invagination and vascular anatomy of vertebral artery as shown in figure II.
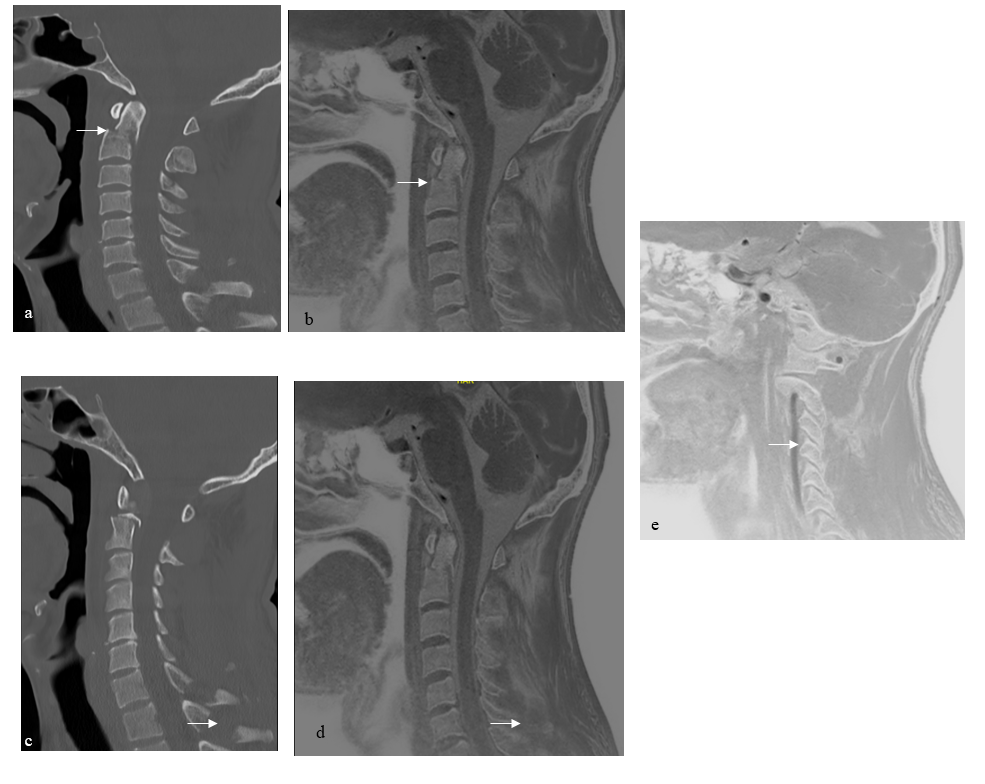
Case 3: A 36-year-old male referred for MRI imaging for assessment of vertebral artery in post-traumatic odontoid fracture was included in our study. MDCT revealed type 2 Odontoid fracture with normal flow related signals in bilateral vertebral arteries along with fractures of spinous process of C6 and C7 vertebra.
CS-FRACTURE imaging on MRI demonstrated all the three fractures with patent VA.(figure III)
Case 4 & 5: 19 year old male with clinical suspicion of CVJ anomaly and 55 year old male with complains of headache served as controls on account of no abnormality demonstrated. However, these cases served to increase the diagnostic confidence.
Hence, although a meagre sample size our preliminary study has demonstrated the efficacy of FFE Resembling A CT Using Restricted Echo-spacing in demonstrating CVJ anomalies, with added benefit of one stop solution for bone, artery and soft tissue evaluation. Additionally, fracture assessment and flexion extension study can also be performed without exposing the patients to harmful ionizing radiation.
Discussion
Novel applications of CS-FRACTURE is extremely useful for the bone fracture assessment as demonstrated in one of patient. (1)In addition it could also demonstrate other CVJ anomalies with image quality and diagnostic information similar to the conventional CT. Further, the necessity to investigate thoroughly the vascular anatomy in particular of the vertebral artery is also captured satisfactorily with this single sequence.(2,3,4) Our small case series illustrates the usefulness of this novel sequence offers in terms of diagnostic quality bone information, cord morphology as well as vascular information.Conclusion
CS-FRACTURE as a sequence offers resolution such that anatomic delineation of bone, soft tissue and vasculature is achieved.Acknowledgements
No acknowledgement found.References
1. Johnson B, Alizai H, Dempsey M. Fast field echo resembling a CT using restricted echo-spacing (FRACTURE): a novel MRI technique with superior bone contrast. Skeletal Radiol. 2021 Aug;50(8):1705-1713.
2. Abtahi AM, Brodke DS, Lawrence BD. Vertebral artery anomalies at the craniovertebral junction: a case report and review of the literature. Evid Based Spine Care J. 2014 Oct;5(2):121-5.
3. Li T, Yin YH, Qiao GY, Wang HW, Yu XG. Three-Dimensional Evaluation and Classification of the Anatomy Variations of Vertebral Artery at the Craniovertebral Junction in 120 Patients of Basilar Invagination and Atlas Occipitalization. Oper Neurosurg (Hagerstown). 2019 Dec 1;17(6):594-602
4. Sardhara J, Behari S, Mohan BM, Jaiswal AK, Sahu RN, Srivastava A, Mehrotra A, Lal H. Risk stratification of vertebral artery vulnerability during surgery for congenital atlanto-axial dislocation with or without an occipitalized atlas. Neurology India. 2015 May 1;63(3):382.
Figures