3816
Amide proton transfer weighted imaging in differential diagnosis of hepatocellular carcinoma from intrahepatic cholangiocarcinoma1Clinical Medical School of Yangzhou University, Northern Jiangsu People’s Hospital, Yangzhou, China, Yangzhou City, China, 2GE Healthcare, MR Research China, Beijing, P.R. China, Beijing City, China
Synopsis
In this study, we aimed to investigate the feasibility of amide proton transfer weighted (APTw) imaging for differentiating hepatocellular carcinoma(HCC) from intrahepatic cholangiocarcinoma(ICC) patients. With the APTw imaging metric of magnetization transfer ratio asymmetry (MTRasym), significantly different magnetization transfer ratio asymmetry (MTRasym) values, a typical metric of APTw imaging, were shown between hepatocellular carcinoma and intrahepatic cholangiocarcinoma. With this finding, APTw imaging could be considered an effective imaging biomarker for differentiating HCC from ICC.
Introduction
Hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC) are two major primary liver cancers. They had different therapy management and different prognosis, thus their preoperational differentiation diagnosis is of great clinic concern. However, these hepatic lesions sometimes showed similar imaging features even scans with contrast. The research on non-invasive imaging methods for making the differentiation diagnosis has always been a hot point.Amide proton transfer weighted (APTw) imaging, as a branch of chemical exchange saturation transfer (CEST) imaging[1], focuses on proton exchange between amide protons of peptides and proteins and bulk water. Some studies have shown that APTw imaging has been extensively applied for grading gliomas, differentiating benign and atypical meningiomas, and brain tumors from edema[2-3]. Moreover, two recent studies showed the potential of APTw imaging in predicting the histologic grades of HCC [4-5]. With these applications, we hypothesized that APTw imaging may help to differentiate hepatocellular carcinoma (HCC) from intrahepatic cholangiocarcinoma (ICC). Therefore, the purpose of this study was to explore the feasibility of APTw imaging in the differential diagnosis between hepatocellular carcinoma and intrahepatic cholangiocarcinoma.
Materials and Methods
SubjectsThe study was approved by the local ethical community and consent forms were obtained from all patients. 13 patients with hepatocellular carcinoma and 5 patients with intrahepatic cholangiocarcinoma, as well as 10 control subjects with normal liver were enrolled in this study. All patients were received liver tumor resection and pathological examination.
MRI experiments
All patients underwent liver MR scanning on a 3.0-tesla scanner (GE DISCOVERY MR750; Milwaukee, Wisconsin, USA) with a 32-channel phased-array torso coil. All patients underwent fasting 4-6 hours before the examination. Liver tumor scan protocol was used including routine T2 weighted imaging, T1 weighted imaging, diffusion-weighted imaging, and four phases dynamic T1 weighed scanning with contrast. Before contrast injection, APTw imaging was performed with a respiratory triggered single slice Spin-echo echo-planar-imaging sequence. Images at 52 frequencies were acquired, including 49 frequencies ranging from -600 to 600 Hz with an increment of 25 Hz. The applied saturation B1 power was 2µt and the saturation duration was 2000ms. Other scan parameters were TE=32.7ms, TR=5432ms, FOV=34cm × 26 cm, Matrix size=128 × 128, and slice thickness=8mm. The scan time was around 2 minutes 36 seconds.
Imaging analysis
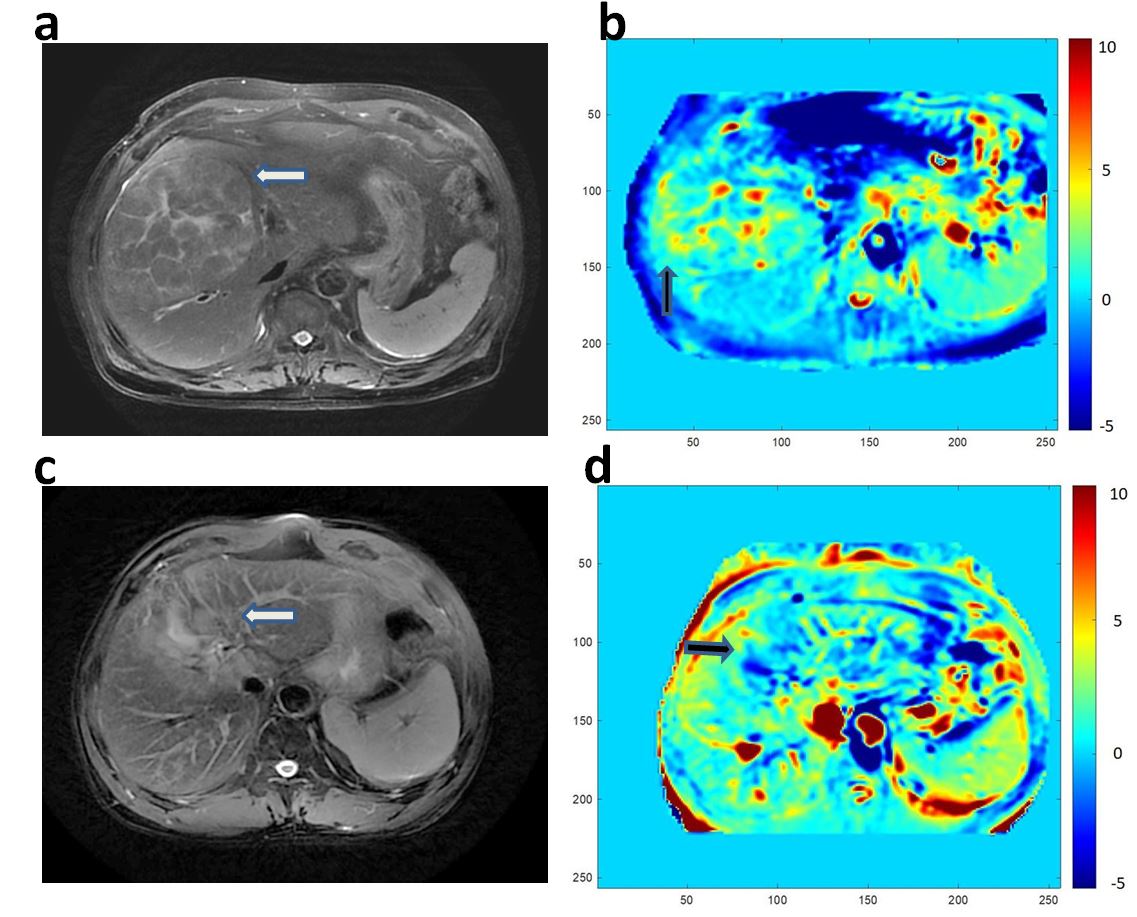
APTw images were analyzed using vendor-provided post-processing software at GE workstation 4.6. The corresponding metric mapping of magnetization transfer ratio asymmetry (MTRasym) at 3.5ppm was obtained for each patient accordingly(Fig 1).
Two radiologists with 5 and 13 experiences were employed for data analysis. Three circular regions of interest (ROIs) with approximately 50mm2 were manually drawn for background liver based on unsaturated M0 images while avoiding gross vessels or tumors. With the reference of axial T2WI images, three identical ROIs were placed manually in the solid component of the tumor for each patient on unsaturated M0 images. Large cystic cavities, large areas of necrosis, calcification, or hemorrhage, or large vessels were excluded from ROI selections. ROIs of background liver and tumor were copied on MTRasym mapping. Averaged MTRasym values over three ROIs of background liver and tumor were calculated separately and used for further analysis. While for the 10 control subjects, three ROIs were also drawn on unsaturated M0 images and copy it to MTRasym mapping.
Statistical analysis
All statistical analyses were performed in SPSS 23.0. The inter-class correction coefficient (ICC) was used to evaluate the inter-observer agreement of measuring MTRasym between two radiologists. ICC>0.75 was considered good reproducibility. Wilcoxon signed-rank test was separately used to analyze the difference of MTRasym between liver tumor and the background liver. The Mann Whitney U test was used to compare MTRasym between HCCs and ICCs. The Kruskal-Wallis test was used to analyze the difference of MTRasym of the background liver between patients with clinically normal livers, ICCs, and HCCs. P<0.05 was considered significant.
Results
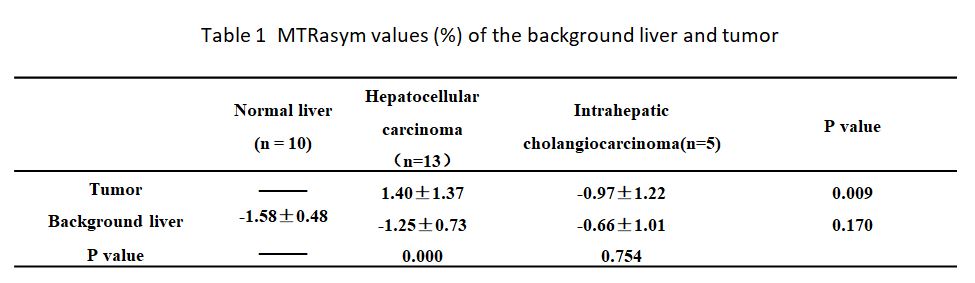
Excellent inter-observer agreements of MTRasym measurement for background liver and tumor between both radiologists were confirmed by high ICCs (0.932, 0.914). The MTRasym of hepatocellular carcinoma was significantly higher than that of intrahepatic cholangiocarcinoma (1.40 ±1.37% vs. 0.97 ±1.22%, P = 0.009). In patients with HCC, the MTRasym values of the background liver (− 1.25 ± 0.73%) were significantly lower than those of HCCs (1.40 ± 1.37%, P < 0.001). Conversely, those values were not significantly different (P = 0.754) in patients with ICC. In addition, the MTRasym values of the background liver among patients with clinically normal livers, HCCs, and ICCs were not significantly different (P = 0.170) (Table1)Discussion and conclusions
Different types of hepatic lesions have distinctly varied cell density and proliferation, which may lead to different APTw effects between proteins and water, resulting in different MTRasym between lesions. In this study, we found that the MTRasym of hepatocellular carcinoma was significantly higher than that of intrahepatic cholangiocarcinoma, implying that hepatic carcinoma and intrahepatic cholangiocarcinoma might have different protein/peptide compositions. In conclusion, this study confirmed the feasibility of APTw imaging in distinguishing hepatic carcinoma and intrahepatic cholangiocarcinoma. Follow-up studies with a larger patient cohort are needed to further validate its diagnostic performance.Acknowledgements
We thank Weiqiang Dou from GE Healthcare for this valuable support on APT sequences.References
1 Zhou J, Heo HY, Knutsson L, van Zijl PCM, Jiang S. APT-weighted MRI: Techniques, current neuro applications, and challenging issues. J Magn Reson Imaging. 2019;50(2):347-364. doi:10.1002/jmri.26645 2 Joo B, Han K, Choi YS, et al. Amide proton transfer imaging for differentiation of benign and atypical meningiomas. Eur Radiol. 2018;28(1):331-339. doi:10.1007/s00330-017-4962-1
3 Choi YS, Ahn SS, Lee SK, et al. Amide proton transfer imaging to discriminate between low- and high-grade gliomas: added value to apparent diffusion coefficient and relative cerebral blood volume. Eur Radiol. 2017;27(8):3181-3189. doi:10.1007/s00330-017-4732-0
4 Wu B, Jia F, Li X, Li L, Wang K, Han D. Comparative Study of Amide Proton Transfer Imaging and Intravoxel Incoherent Motion Imaging for Predicting Histologic Grade of Hepatocellular Carcinoma. Front Oncol. 2020;10:562049. Published 2020 Oct 29. doi:10.3389/fonc.2020.562049
5 Lin Y, Luo X, Yu L, et al. Amide proton transfer-weighted MRI for predicting histological grade of hepatocellular carcinoma: comparison with diffusion-weighted imaging. Quant Imaging Med Surg. 2019;9(10):1641-1651. doi:10.21037/qims.2019.08.07
Figures