3779
Intravoxel Incoherent Motion MR Imaging-based Virtual Elastography for the Assessment of Placenta Accreta1Department of Radiology, the first Affiliated Hospital of Xi'an Jiaotong University, xi'an, China
Synopsis
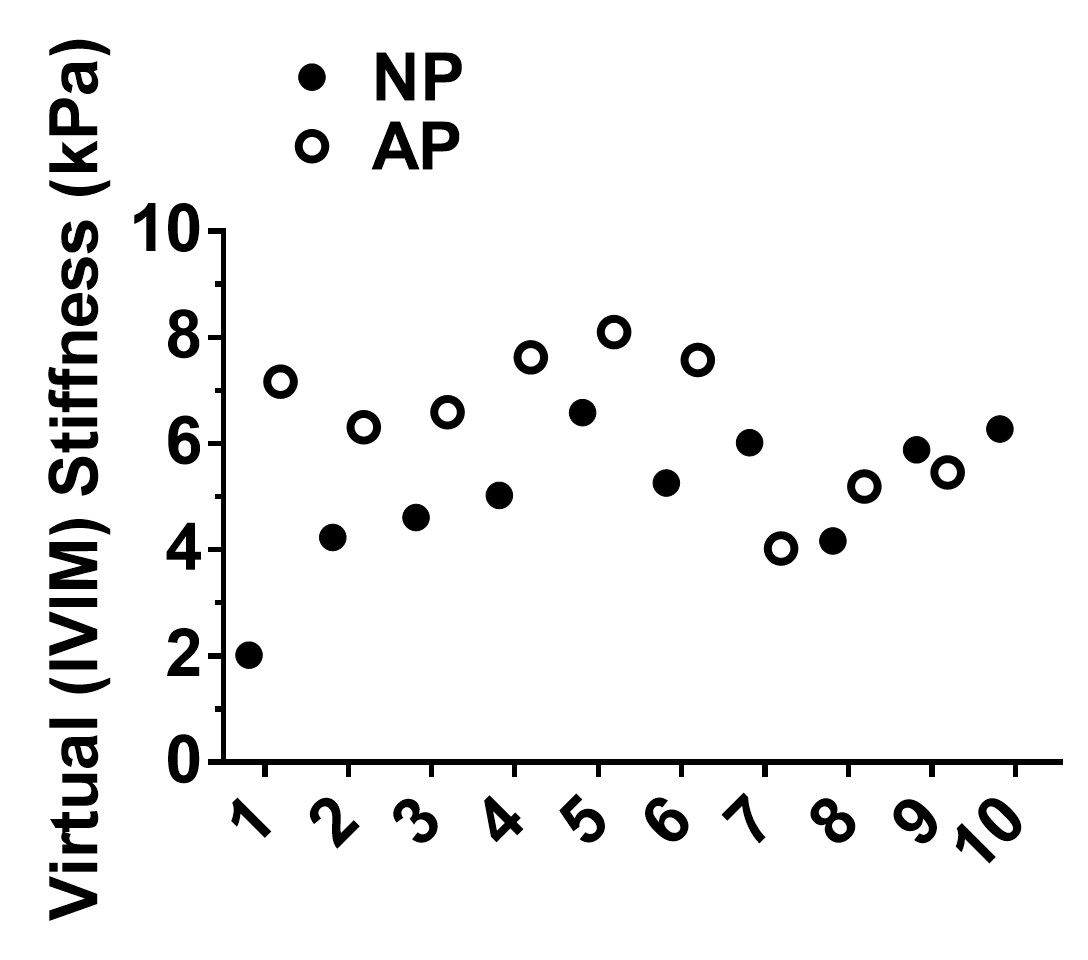
Placenta accreta may lead to life-threatening complications and is difficult to distinguish by traditional MRI sequences. In this study, IVIM-based virtual elastography was used for the first time to detect the stiffness of the placenta, and it was found that the virtual (IVIM) stiffness values for the AP-ROIs were mostly higher than those for the NP-ROIs; the IR-ROIs were also significantly higher than the NIR-ROIs. Thus, the implanted regions of the placenta could be significantly stiffer than those of the non-implanted regions. That is helpful for adding a new method for clinical diagnosis of placenta accreta.
Introduction
Placenta accreta, one of the most fatal obstetric complications, has surged during the past decades because of the higher number of cesarean deliveries1. About 49% of the peripartum hysterectomies are due to abnormal placentation adherence, therefore, the prenatal diagnosis of placenta accrete plays an important role2. Although ultrasound (US) is the first imaging choice for the placenta accreta because of its convenience, magnetic resonance imaging (MRI) has a complementary role owing to the limitations of US under certain conditions. However, it was difficult to find implantable region using MRI alone, our study found a new method named virtual elastography based on Intra Voxel Incoherent Motion (IVIM) that could be helpful in diagnosis of placenta accrete.Materials and Methods
This study was approved by the ethical committee of First Affiliated Hospital of Xi’an Jiaotong University. Written informed consent was obtained for all participants. 19 participants were recruited from March 2017 to August 2020 in the First Affiliated Hospital of Xi’an Jiaotong University. No drugs were used for MRI. The scanning was stopped immediately once the participants feel uncomfortable. MRI examination for each participant was performed on a 3T MRI system (GE Healthcare, Milwaukee, Wisconsin) with an 8-channel body flex coil. IVIM images were collected with each of the following b values: 0, 20, 50, 80, 100, 150, 200, 400, 600, 800sec/mm2. IVIM images of the lower b-value (Slow, b value = 200 s/mm2) and those of the higher b-value (Shigh, b value = 800 s/mm2) were used to estimate the virtual (IVIM) stiffness: $$$virtual (IVIM) stiffness = α·ln (Slow/Shigh) + β$$$. The scaling (α) and the shift (β) factors were separately set to -9.8 and 14 according to the previous calibration studies3, 4. Regions of interest (ROI) were drawn under the direction of an experienced obstetrician and reference 1. AP-ROIs and NP-ROIs were drawn on the three thickest planes of the placenta. IR-ROIs were drawn in the center of the suspicious accreta lesion of the AP. NIR-ROIs were drawn on the placenta at least 2 cm away from the suspicious accreta lesion on the AP.Results
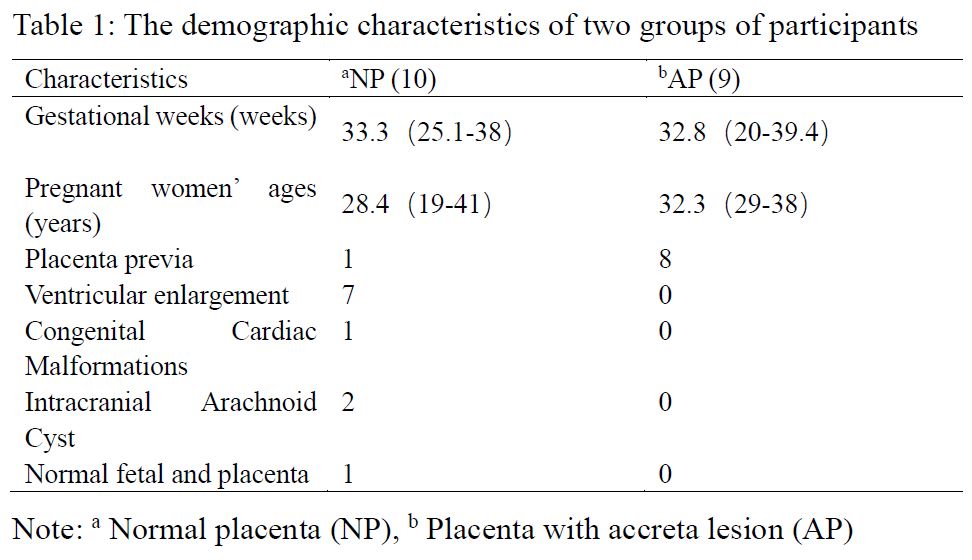
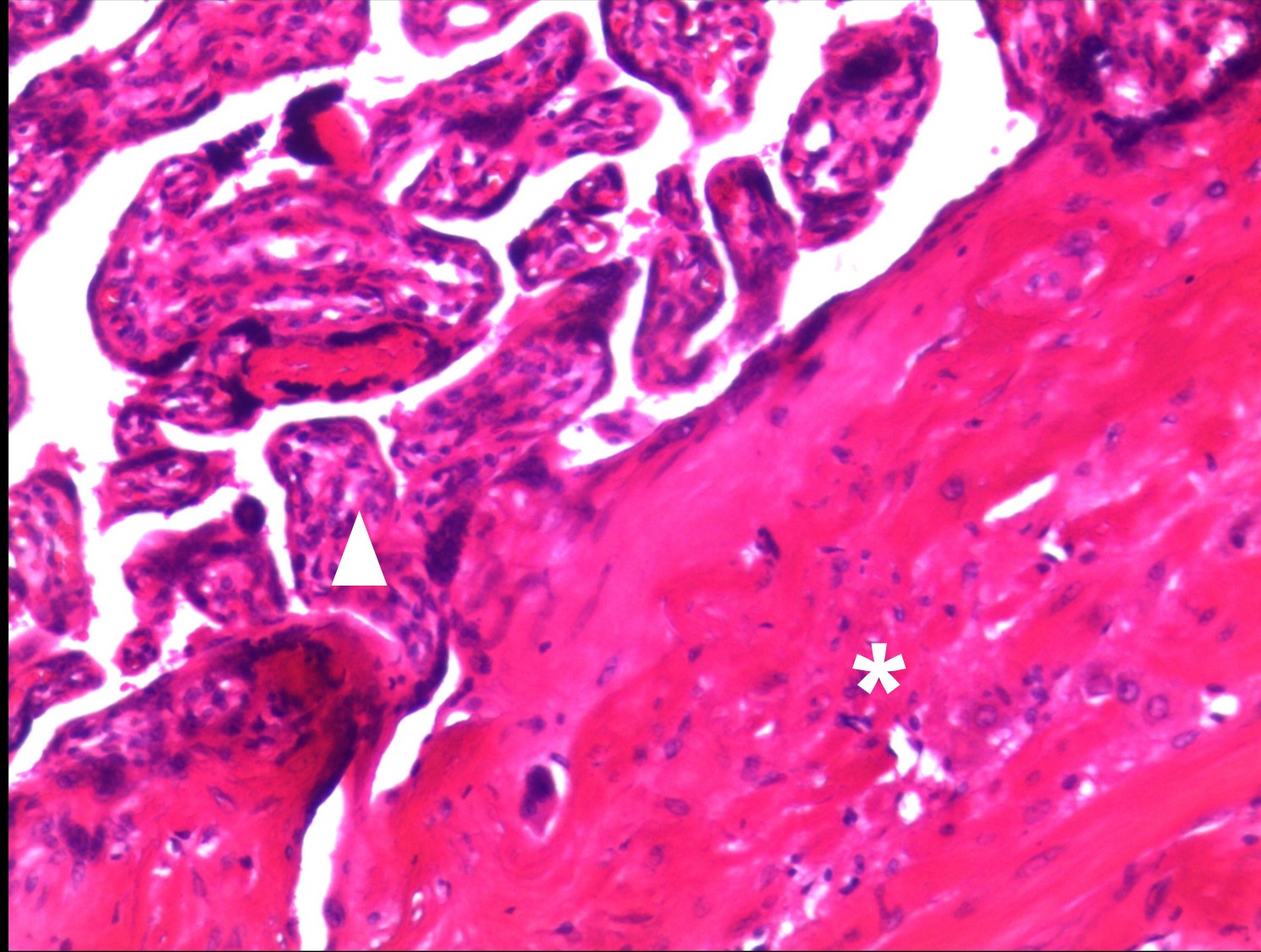
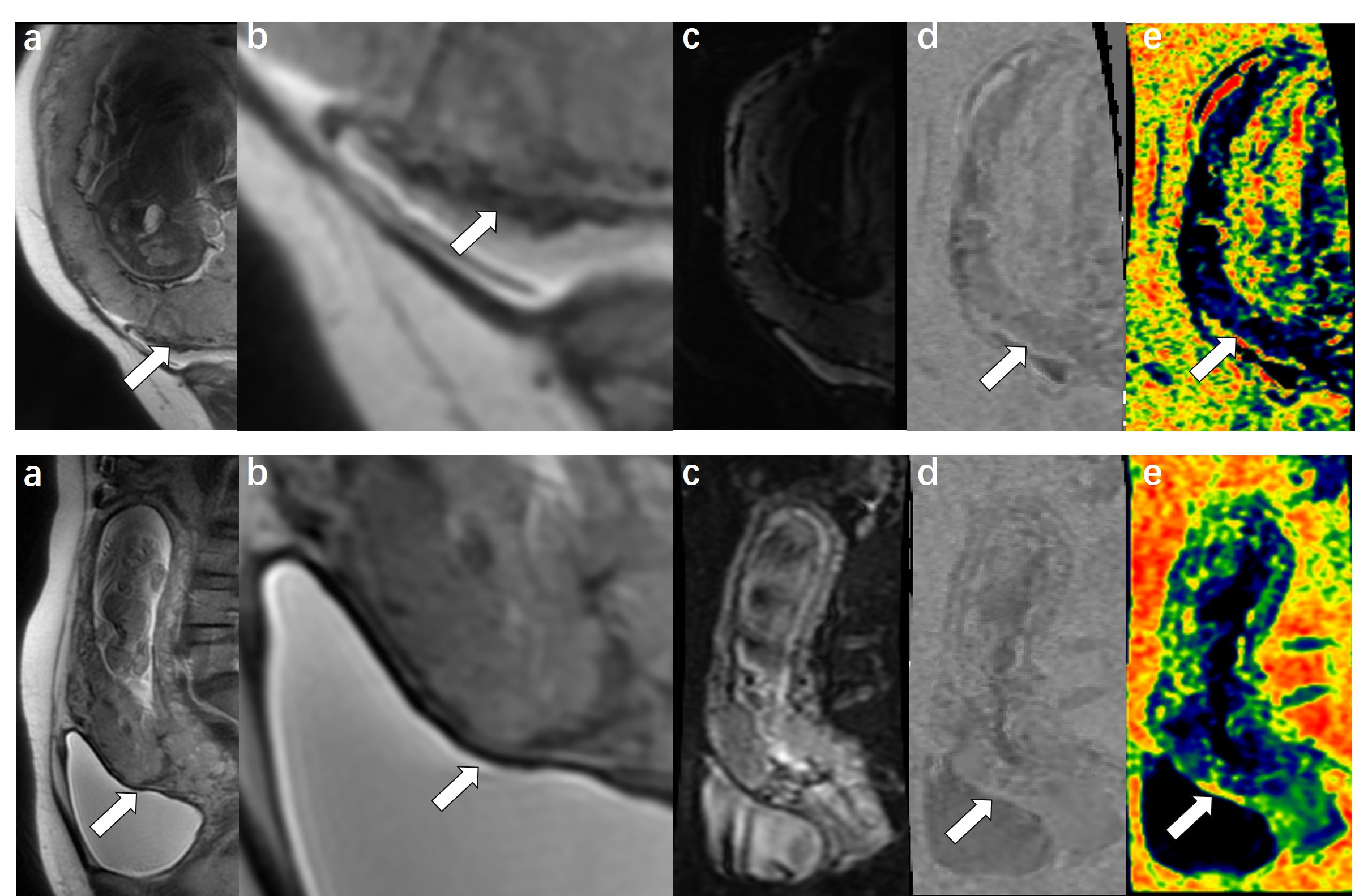
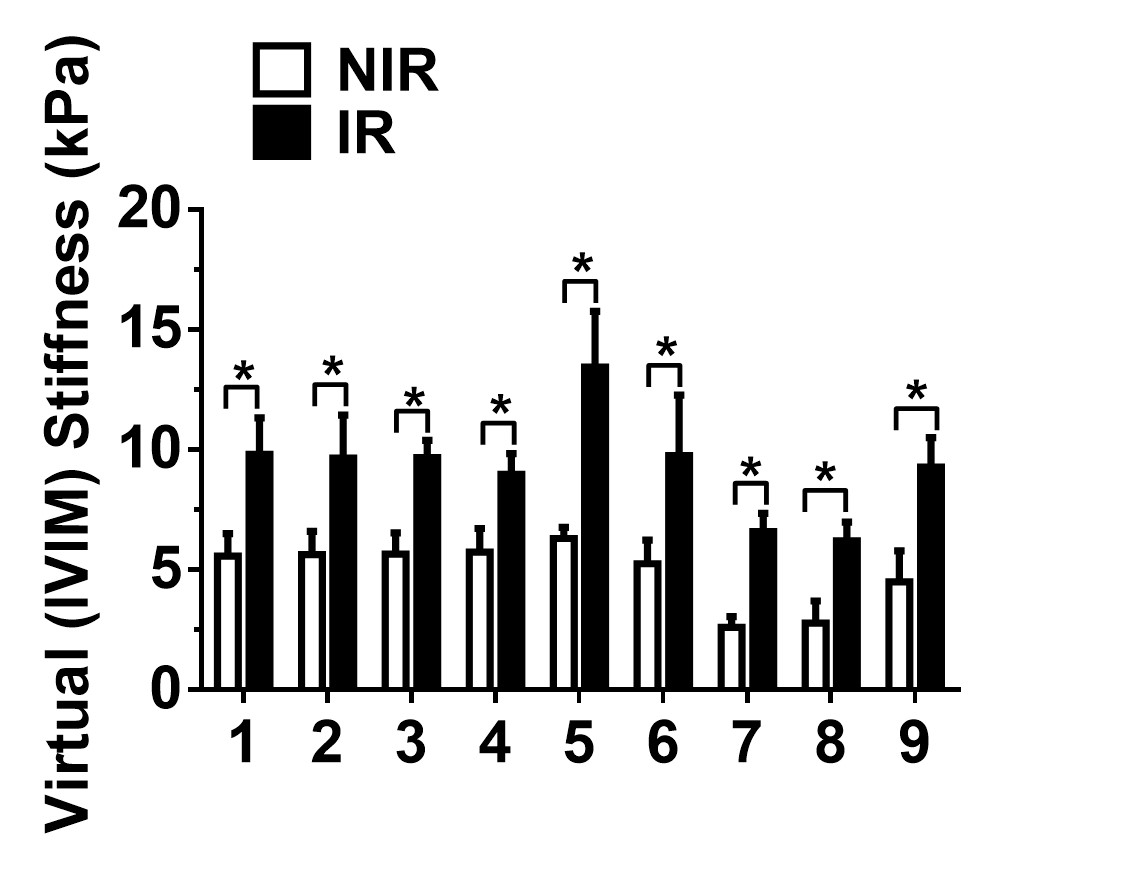
A total of 19 participants were enrolled, and 9 of them were patients who diagnosed placenta accreta surgically or pathologically (Figure 1). Demographic and clinical characteristics are described in Table 1. The median gestational ages at MRI scan were 28.4(19-41)years in the NP group and 32.3(29-38)years in the AP group. The median gestational weeks at MRI scan were 33.3(25.1-38)weeks in the NP group and 32.8(20-39.4)weeks in the AP group. No significant difference was found between the gestational ages and gestational weeks of the AP and NP groups at MRI (p > 0.05). IVIM post-processing virtual elastography images and T2WI for normal placenta and implantable placenta were shown in Figure 2. The virtual (IVIM) stiffness values were mostly higher in the AP group than in the NP group, as shown in Figure 3. The virtual (IVIM) stiffness values of each patient were significantly higher in the IR group than in the NIR group (p < 0.05), as shown in Figure 4. The median virtual (IVIM) stiffness values in the IR and NIR groups were 9.27 kPa and 4.90 kPa, respectively.Discussion
MRI elastography is not currently used in pregnant women because of its unknown effects on the fetus. Another method, shear-wave elastography (SWE), could only be used for superficial tissues and couldn't get comprehensive data of the placenta. In this study, a non-invasive diagnostic method named IVIM-based virtual elastography is ultilized for diagnosis of placenta accrete and has proven to be a new model which was originally applied for the assessment of liver fibrosis5. Through this method, we found that mostly the placenta with accreta was stiffer than that of the normal placenta, which is consistent with other studies ultilized the acoustic radiation force impulse elastography or SWE 6, 7. Furthermore, the implantable region of the placenta was stiffer than that of the non-implanted region. Durhan, G., et al. performed strain elastography and histopathological examinations on ex vivo placentas showing that the placentas of the intra-uterine growth restriction (IUGR) group were markedly stiffer than those of the control group and the placentas of the IUGR group showed more histopathological changes than those of the control group8. Thus, we speculated that this is possibly due to more histopathological changes of placenta accrete group than those of the control group. However, the relatively low number of participants and breathing artifacts limited the strength of the conclusion. Also, we did not identify the histopathological changes causing the stiffness in the accreta placenta. Objects that changes the magnetic field such as calcification may cause an inaccuracy due to the principle of IVIM-based virtual elastography calculation. Therefore, future studies should enroll more participants and combine with the pathology. In conclusion, this is the first report of IVIM-based virtual elastography used for placenta, which is likely to be used as a new method of diagnosis for placental implantation.Conclusion
The implanted region of placenta is stiffer compared to the normal placenta, which will be conducive for diagnosis.Acknowledgements
This work was supported by the Foundation of the First Affiliated Hospital of Xi'an Jiaotong University (Grant No. 2020QN‐27).References
1. Bourgioti C, Konstantinidou AE, Zafeiropoulou K, et al., Intraplacental Fetal Vessel Diameter May Help Predict for Placental Invasiveness in Pregnant Women at High Risk for Placenta Accreta Spectrum Disorders. Radiology, 2021. 298(2): p. 403-412.
2. D'Arpe S, Franceschetti S, Corosu R., et al, Emergency peripartum hysterectomy in a tertiary teaching hospital: a 14-year review. Arch Gynecol Obstet, 2015. 291(4): p. 841-7.
3. Lagerstrand K, Gaedes N, Eriksson S, et al., Virtual magnetic resonance elastography has the feasibility to evaluate preoperative pituitary adenoma consistency. Pituitary, 2021. 24(4): p. 530-541.
4. Le Bihan D, Ichikawa S, Motosugi U, S. Ichikawa, and U. Motosugi, Diffusion and Intravoxel Incoherent Motion MR Imaging-based Virtual Elastography: A Hypothesis-generating Study in the Liver. Radiology, 2017. 285(2): p. 609-619.
5. Kromrey ML, Le Bihan D, Ichikawa S, et al., Diffusion-weighted MRI-based Virtual Elastography for the Assessment of Liver Fibrosis. Radiology, 2020. 295(1): p. 127-135.
6. Dokumaci, D.S. and H. Uyanikoglu, Shear-wave elastography for detection of placenta percreta: a case-controlled study. Acta Radiol, 2021: p. 284185121997768.
7. Bayramoglu Tepe N, Gelebek Yilmaz F, Bozdag Z, et al., Subgroup analysis of accreta, increta and percreta cases using acoustic radiation force impulse elastography. J Obstet Gynaecol Res, 2020. 46(5): p. 699-706.
8. Durhan G, Unverdi H, Deveci C, et al., Placental Elasticity and Histopathological Findings in Normal and Intra-Uterine Growth Restriction Pregnancies Assessed with Strain Elastography in Ex Vivo Placenta. Ultrasound Med Biol, 2017. 43(1): p. 111-118.
Figures