3762
Reliability of the volumetric positional probability distribution of liver tumor using volumetric 4D-MRI: effect of temporal resolution
Oi Lei Wong1, Jing Yuan1, Darren Ming Chun Poon2, Yi Hang Zhou1, Siu Ki Yu3, and Kin Yin Cheung3
1Research Department, Hong Kong Sanatorium & Hospital, Hong Kong, Hong Kong, 2Comprehensive Oncology Center, Hong Kong Sanatorium & Hospital, Hong Kong, Hong Kong, 3Medical Physics Department, Hong Kong Sanatorium & Hospital, Hong Kong, Hong Kong
1Research Department, Hong Kong Sanatorium & Hospital, Hong Kong, Hong Kong, 2Comprehensive Oncology Center, Hong Kong Sanatorium & Hospital, Hong Kong, Hong Kong, 3Medical Physics Department, Hong Kong Sanatorium & Hospital, Hong Kong, Hong Kong
Synopsis
This study aims to evaluate the impact of temporal resolution on the positional probability distribution. Based on our results, PPV was independent of the fps setting and was most reliable at the probability of occurrence >35 - 50%. Thus, PPV is potentially useful to minimize the registration error during daily positional verification.
Purpose
Volumetric 4DMRI has been proposed for motion characterization and management in radiotherapy due to the superior soft-tissue contrast of MR images. While the feasibility of probabilistic volume generation using volumetric 4DMRI has been demonstrated [1,2], the characteristic of the probabilistic volume is yet to be investigated. With the inclusion of more respiration cycles using 4DMRI, the data sampling, in theory, better resembles the target motion during the radiotherapy treatment and, hence, leads to a more reliable positional probability distribution. This pilot study aims to investigate the reliability of the positional probability distribution estimated based on 4D-MR images at 4 temporal resolution settings.Methods:
A total of 7 patients (Table 1) with gross target volume (GTV) located in the abdominal area were recruited. Abdominal 4D-MRI was performed at a 1.5T MR simulator using 3D T1 weighted CAIPIRANHA-TWIST-VIBE sequence (Axial, TE/TR=0.35/1.57ms, flip angle=5o, FOV=350-382mm, acquisition matrix size=128 x 128; slices=52; slice thickness=4.5mm; reconstruction voxel size=2.7x2.7x4.5mm3, phase FOV=71.9%; partial Fourier factor 75% (phase encoding)/62% (slice encoding); slice over-sampling factor=20%; 20% central and 33% peripheral k-space sampling percent by TWIST; frame rate = 3.0 frame-per-sec (fps); acceleration factor=4). For all scans, in a total of 576 dynamics were acquired with the patients positioned and immobilized using their radiotherapy setup and immobilization device to simulate the GTV motion of a single RT fraction with ~4 minutes beam-on time. The segmentation of the GTV (Seg1) was manually delineated on the first dynamic by following the radiotherapy treatment plan while the subsequence dynamics were generated by rigidly transforming the Seg1. Each scan was also retrospectively downsampled into 4 fps groups ( A: ~0.76 fps, 144 dynamics, B: ~1 fps, 192 dynamics, C: ~1.5fps, 292 dynamics; D: ~3.0fps, 576 dynamics). For each fps group, the volume (PPVi) with the >i% probability that the GTV would be seen with PPVi was calculated. For each fps group, PPVs were generated with 21 probability thresholds (i), ranging between 0% and 100% in a step of 5%. For a fair comparison, statistical analysis was done on the normalized PPVi (PPVi divided by GTV). Intra-class correlation (ICC) and coefficient of variation (CV) were calculated to evaluate the inter-subject and inter-frame-rate reliability of the PPVs. ANOVA and Tukey’s HAD tests were applied where appropriate with the significant level set at 0.05.Results
For all patients, the tumors were located either within the liver or adjacent to the liver and were mainly following the respiratory motion (Table 1). A similar decreasing trend in the normalized PPVs with increasing i was observed for all choices of fps (Figure 1 and Table 2). Based on the 2-way ANOVA results, normalized PPVs were significantly influenced by the choice of i and were independent of the temporal resolution setting (probability: p<0.001, fps: p>0.99). It is consolidated with the excellent repeatability (ICC>0.88, two-way model, single agreement) noted among the fps for all choice i. Excellent inter-subject repeatability was noted (ICC=0.815) while more reliable PPVi was found between i=35 to i=50% with CV<10% (Figure 2). As illustrated in Figure 3, different decreasing PPV rates with increasing probability were observed for all choices of GTV size. More rapid decreasing rate in PPV was noted in larger GTVs (Lesions 2, 1 and 7), suggesting the PPV change might be GTV size dependent. Moderate decreasing rate in PPV was also noted in Lesion 5 but was less rapid in GTV of similar size (Lesion 6), where GTV location was likely the cause.Discussion
Based on our results, the PPV was least affected by the choice of fps and was most affected by the choice of probability threshold, GTV location, and GTV size. Accurate alignment between the on-board imaging and planning ITV is essential during the intra-fraction positional verification to avoid additional error throughout the patient radiotherapy treatment. To date, various alignment techniques had been proposed, where the choice of techniques has been reported to be related to the respiratory pattern [3]. As such, the stable PPV setting (i.e. PPV35% - PPV50%) observed in this study is potentially a simple and reliable tool for positional verification, though the inter-sessional reliability is yet to be investigated. It is worth noting that the lowest temporal resolution in this study was chosen to be 0.76 fps to ensure sufficient sample size for the PPV generation in each fps group, which was still faster than the typical respiratory cycle (0.3 Hz). Further study will be conducted to simulate the PPV change at a temporal resolution close to the Nyquist limit.Conslusion
The stable PPV was been identified and was found to be independent of the fps setting and tumor size. It may have an important role as the registration reference to minimize the registration error during daily positional verification.Acknowledgements
No acknowledgement found.References
[1] Yuan J, Wong OL, Zhou Y, et al. A fast volumetric 4D-MRI with sub-second frame rate for abdominal motion monitoring and characterization in MRI-guided radiotherapy.Quant Imaging Med Surg. 2019; 9(7):1303-1314.[2] Rabe Moritz, Thieke C, Düsberg M, et al. Real-time 4DMRI-based internal terget volume definition for moving lung tumors. Med Phys. 2020; 47(4): 1431-12.[3] Clements N, Kron T, Franich R, et al. The effect of irregular breathing patterns on internal target volumes in four-dimensional CT and cone-beam CT images in the context of stereotactic lung radiotherapy. Med Phys. 2013; 40(2): 021904Figures
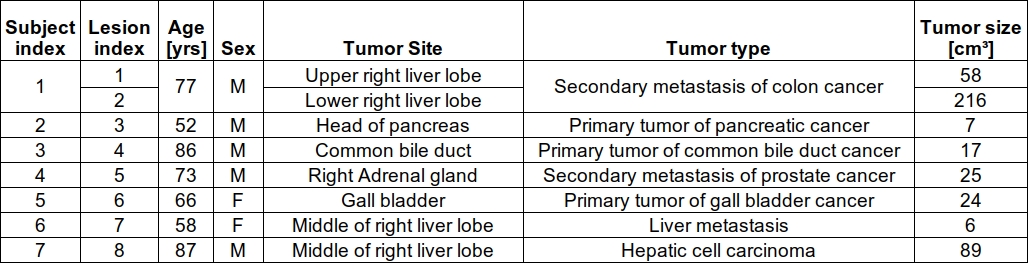
Table 1. Tumor characteristic including tumor location, tumor size and tumor type are listed.
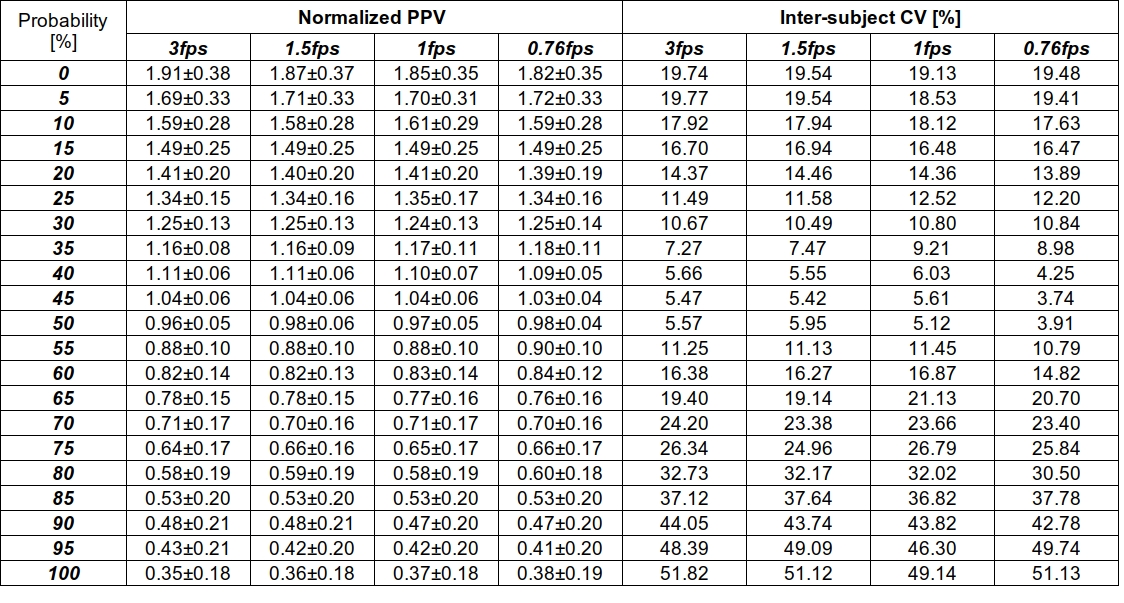
Table 2. The normalized PPV size and intra-sessional CV at various probability settings. The dice-similarity coefficient between the reference PPV (temporal resolution = 3fps) and that at each of the remaining temporal resolution settings (1.5fps, 1fps and 0.76fps) were also illustrated.
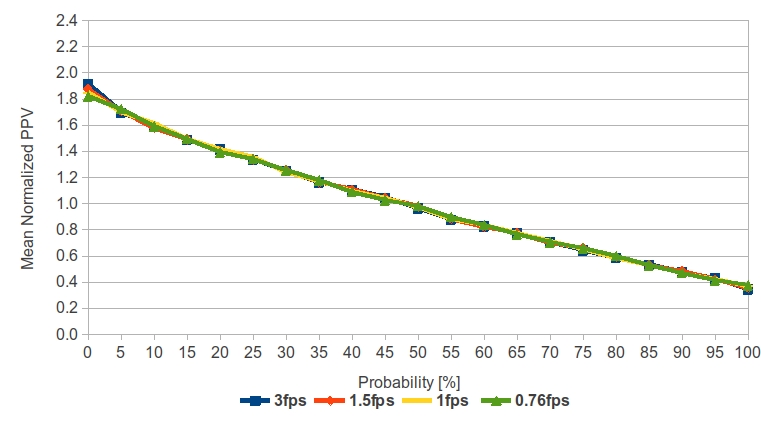
Figure 1: The normalized PPV as a function of probability threshold (i). For all fps settings, an overall decrease in the normalized PPV was observed with increasing i.
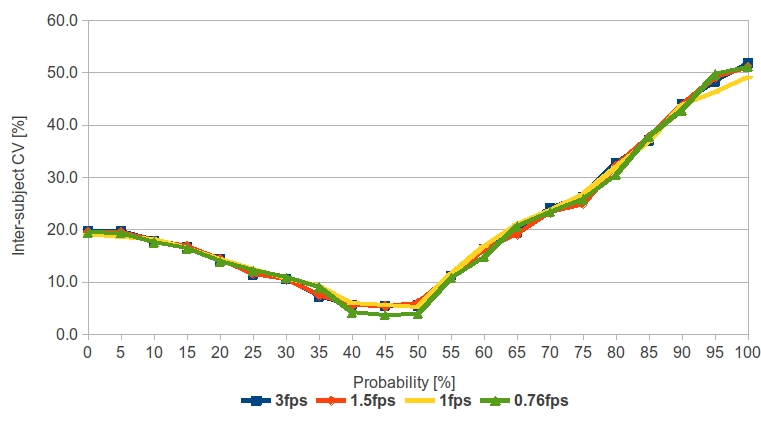
Figure 2: The inter-subject CV as a function of probability. The smallest inter-subject CV was found at probability between 35 – 50% with CV< 10%.
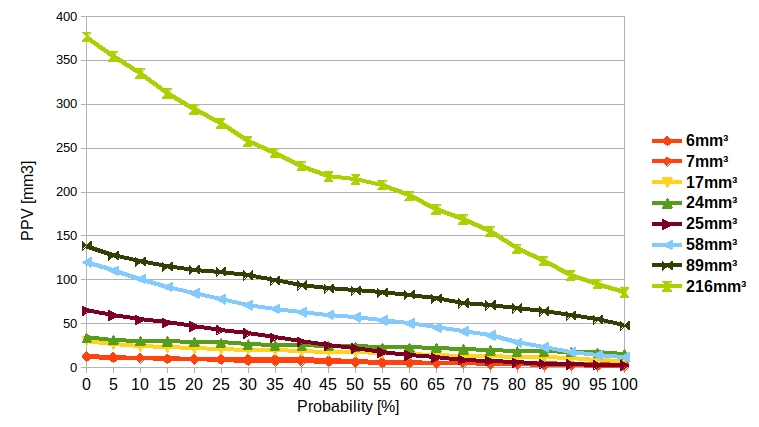
Figure 3: PPV size [mm3] at various probability thresholds (i). All GTVs exhibited different PPV decreasing rates as i increased. The rapid change in the PPV size was noted in large lesions.
DOI: https://doi.org/10.58530/2022/3762