3756
Focused ultrasound thalamotomy for the treatment of tremor impacts the cerebello-thalamo-cortical tremor network1Henan Provincial People’s Hospital & People Hospital of Zhengzhou University, Zhengzhou, China, 2Athinoula A. Martinos Center for Biomedical Imaging, Boston, MA, United States, 3Medical University of South Carolina, Charleston, SC, United States
Synopsis
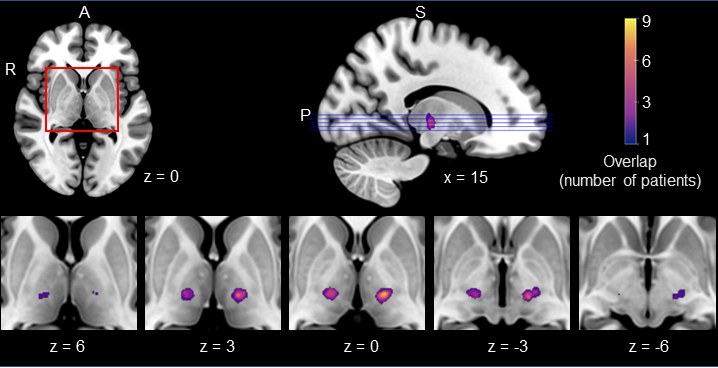
We used Magnetic Resonance-guided Focused Ultrasound to reduce hand tremor in 13 patients with Parkinson’s disease and essential tremor, by lesioning the ventral intermediate nucleus (VIM) of the thalamus. We also investigated the functional reorganization of the brain after the procedure. We observed a 67% reduction in target hand tremor following the procedure. The regions that showed above-average change in functional connectivity are part of the cerebello-thalamo-cortical tremor network, confirming that lesioning the VIM was successful in targeting this network. We also observed some normalization in the functional connectivity of the target hand motor region, congruent with tremor alleviation.
Introduction
Tremor is an involuntary symptom of disorders such as Parkinson’s disease and essential tremor that can be debilitating. Various lines of treatment exist, and brain ablation is sometimes necessary in severe cases. Magnetic Resonance-guided Focused Ultrasound (MRgFUS) is a non-invasive procedure that produces focal lesions in the brain while preserving surrounding tissue. Here, we used MRgFUS to lesion the ventral intermediate nucleus (VIM) of the thalamus, an important node in the cerebello-thalamo-cortical tremor network. We investigated MRgFUS’s efficacy in alleviating tremor in the most affected hand, and probed the functional organization of the brain before and after the intervention.Methods
Patients with Parkinson’s disease (n=10) and essential tremor (n=3) underwent the procedure (age range: 46-67; 2 women, 11 men). Forty-eight control participants, matched in age, sex, and global cognition, were included in the study (age range: 38-70; 22 women, 26 men). Symptom evaluation, neuropsychological testing, and neuroimaging were performed one or two days before the intervention, one day after the intervention, and again one month later. We assessed hand tremor using the CRST subitems for rest, posture, and action/intention tremor. We acquired extensive resting-state functional MRI data in each participant, which was used to characterize the subject-specific functional network organization of the brain1.Results
We observed a substantial and significant alleviation of tremor in the target hand (t(12)=7.21, p<0.001, 2-tailed). An FDR-corrected general linear regression, with within-individual variability in functional connectivity (FC) as a control factor, revealed no significant changes in the functional organization of the brain at the whole-brain level, one month after the intervention (p>0.05). Although not statistically significant, above-average changes in functional connectivity patterns were observed in the sensorimotor strip, lateral temporal cortex, anterior cingulate cortex, and occipital cortex. These regions mostly belonged to the motor, limbic, visual, and dorsal attention functional networks of the brain, and overlapped substantially with the regions functionally connected to the VIM (Dice overlap=0.47 for cortico-cortical FC and 0.53 for cortico-cerebellar FC). The FC of the brain’s hand regions was compared between patients and control participants, before and after the procedure. There was a non-significant normalization of the cortical target hand region (p>0.05), while the cerebellar target hand region showed significant normalization (t(12) = -1.90, p = 0.041, 1-tailed). The non-target hand regions, which served as control regions, exhibited no substantial or significant normalization (all p’s>0.05). In terms of adverse effects, one month after the procedure, 3/13 patients (23%) were experienced gait disturbances, and 5/13 patients (38%) experienced paresthesia.Discussion
Patients with PD and ET experienced a 67% improvement in tremor symptoms on average, as assessed with the CRST subitems. These alleviations are comparable to those observed in prior MRgFUS studies in which the VIM was lesioned, where improvements in target hand/side tremor ranging 47%-90% were observed2-6. There were no significant changes in FC at the whole-brain level, as expected due to the small size of the lesions and low sample size. The regions that exhibited some degree of change in their functional organization, however, are regions known to be part of the tremor network7, 8. The cortical target hand region’s patterns of FC with the cortex and with the cerebellum became more similar to controls’ FC patterns one month after the procedure, although these effects were statistically non-significant. The cerebellar target hand region, on the other hand, exhibited significant normalization. In contrast, the non-target hand regions did not show any substantial or significant normalization of their FC patterns. These findings are congruent with the fact that patients experienced a marked alleviation of tremor in the target hand, and virtually no change in the non-target hand.Conclusion
Our findings indicate that MRgFUS is a highly efficient treatment for tremor in both Parkinson’s disease and essential tremor. There is evidence that lesioning the VIM resulted in the reorganization of the cerebello-thalamo-cortical tremor network, and in the normalization of the brain’s target hand regions.Acknowledgements
This work was supported by NIH grants R01NS091604, P50MH106435, R01DC016765, and R01DC016915; and by the National Natural Science Foundation of China grants No. 81790652, 81720108021, National Key R&D Program of China No. 2017YFE0103600. L.Da. is supported by a Canadian Institutes of Health Research postdoctoral fellowship, FRN: MFE-171291.References
1. Wang D, Buckner RL, Fox MD, Holt DJ, Holmes AJ, Stoecklein S, et al. Parcellating cortical functional networks in individuals. Nature neuroscience 2015; 18(12): 1853-60.
2. Elias WJ, Huss D, Voss T, Loomba J, Khaled M, Zadicario E, et al. A pilot study of focused ultrasound thalamotomy for essential tremor. New England Journal of Medicine 2013; 369(7): 640-8.
3. Lipsman N, Schwartz ML, Huang Y, Lee L, Sankar T, Chapman M, et al. MR-guided focused ultrasound thalamotomy for essential tremor: a proof-of-concept study. The Lancet Neurology 2013; 12(5): 462-8.
4. Elias WJ, Lipsman N, Ondo WG, Ghanouni P, Kim YG, Lee W, et al. A randomized trial of focused ultrasound thalamotomy for essential tremor. New England Journal of Medicine 2016; 375(8): 730-9.
5. Bond AE, Shah BB, Huss DS, Dallapiazza RF, Warren A, Harrison MB, et al. Safety and efficacy of focused ultrasound thalamotomy for patients with medication-refractory, tremor-dominant Parkinson disease: a randomized clinical trial. JAMA neurology 2017; 74(12): 1412-8.
6. Fasano A, Llinas M, Munhoz RP, Hlasny E, Kucharczyk W, Lozano AM. MRI-guided focused ultrasound thalamotomy in non-ET tremor syndromes. Neurology 2017; 89(8): 771-5.
7. Zhang JR, Feng T, Hou YN, Chan P, Wu T. Functional connectivity of vim nucleus in tremor‐and akinetic‐/rigid‐dominant Parkinson's disease. CNS neuroscience & therapeutics 2016; 22(5): 378-86.
8. Al-Fatly B, Ewert S, Kübler D, Kroneberg D, Horn A, Kühn AA. Connectivity profile of thalamic deep brain stimulation to effectively treat essential tremor. Brain 2019; 142(10): 3086-98.
Figures
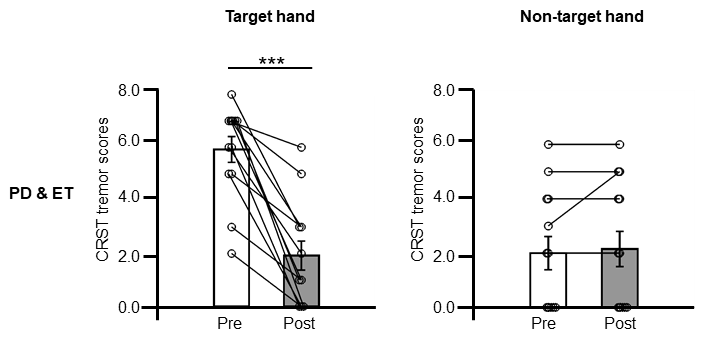
MRgFUS successfully alleviated tremor in the target hand. CRST tremor scores are shown for all 13 patients (PD and ET; top), for the target hand (left) and non-target hand (right). There was a significant decrease in average target hand CRST tremor scores from pre- to post-intervention (t(12) = 7.21, p < 0.001, 2-tailed), while, as expected, no significant decrease was found for the non-target hand (t(12) = -1.00, p = 0.34, 2-tailed). Error bars represent standard errors of the mean. The lines connect datapoints from the same participants.
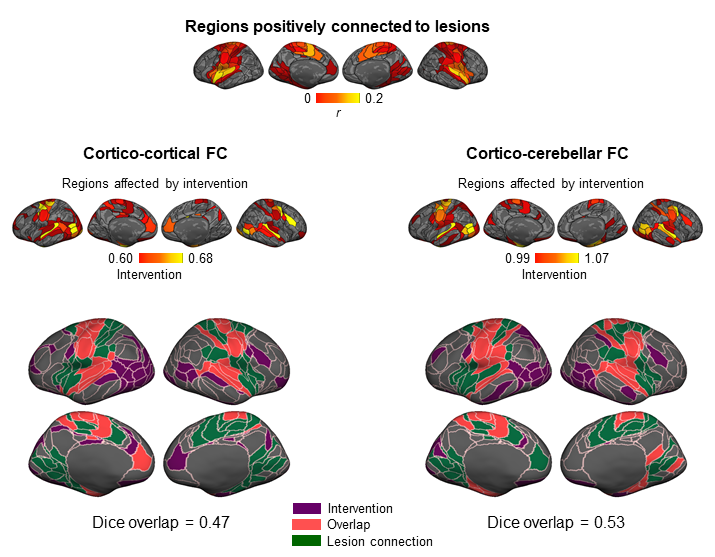
Regions functionally connected to the lesion sites exhibited a change in their functional connectivity following the intervention. The cortical maps shown on top depict the regions functionally connected to the ventral intermediate nucleus lesions. The middle panels show the regions that showed above-average changes in their functional connectivity (FC). The overlap between the regions connected to the lesion sites and those that demonstrated an intervention effect are shown on the bottom (Dice=0.47 for cortico-cortical FC, and 0.53 for cortico-cerebellar FC).