3727
Dilated perivascular spaces in neonates1The Catholic University of Korea, Seoul, Korea, Republic of, 2Division of Biomedical Engineering, Hankuk University of Foreign Studies, Yongin, Korea, Republic of
Synopsis
Perivascular spaces (PVS) are fluid-filled cavities around the blood vessels in the brain. In adults, dilated PVS (dPVS) is known to increase with age but dPVS in neonates is poorly understood. In this study, we performed both visual and volumetric evaluation of dPVS in neonates using T2-weighted images from the Developing Human Connectome project. We found that gender did not affect dPVS extent in neonates, preterm neonates had lower dPVS extent than term neonates, and dPVS fraction decreased with gestational age (GA) at MRI scan.
Introduction
Dilated perivascular spaces (dPVS) are visible on MRI and thought to reflect dysfunction in the fluid circulation of the glymphatic system. Glymphatic system in the brain is a system that plays an important role in waste clearance. In adults, dPVS is known to increase with advanced age and is considered an emerging biomarker for various diseases1,2.In contrast, dPVS in the young population is poorly understood. Some reports showed a very high prevalence of dPVS in children and other reports showed a higher incidence of dPVS in children with epilepsy3. In neonates, the glymphatic system may play a role in the development and pathogenesis of the brain. However, there is limited information on the severity and regional distribution of dPVS in neonates. Therefore, the objective of our study was to perform a visual and volumetric evaluation of dPVS in neonates.
Method
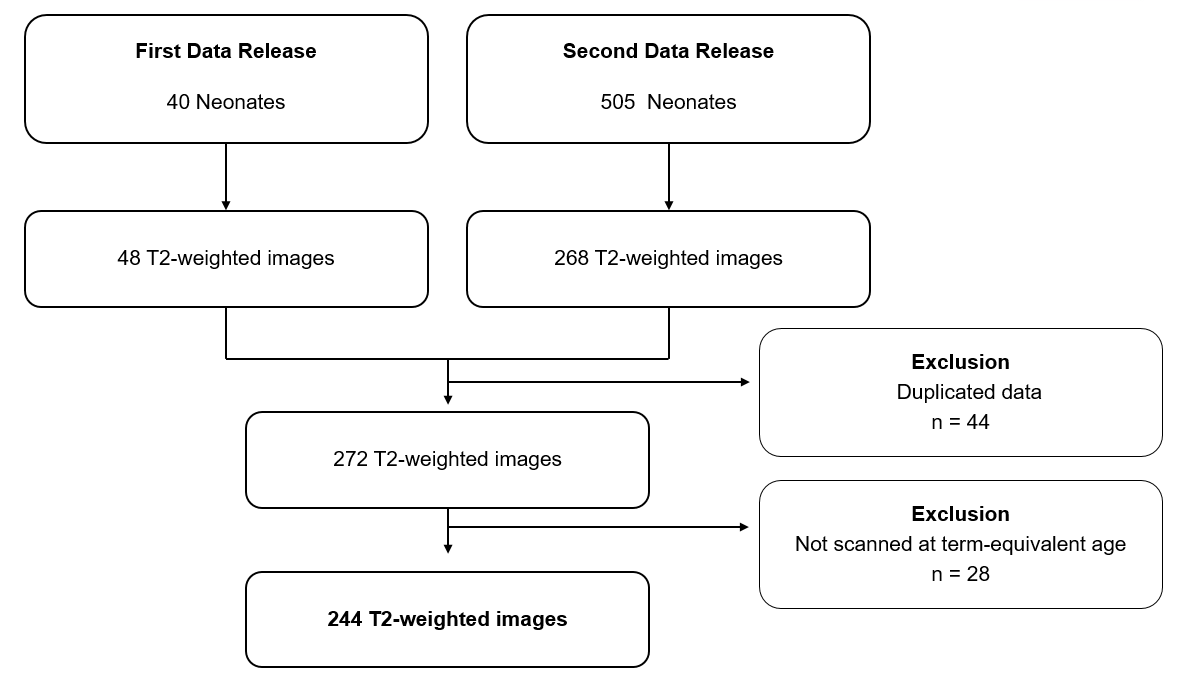
We collected 2D T2-weighted images of neonates from public data set, the Developing Human Connectome project (http://www.developingconnectome.org)4. We included images of both data release 1 and 2. After excluding duplicated cases and the cases that were obtained before term-equivalent age, total of 244 neonates’ images were included (Figure 1).The 2D turbo spin-echo T2-weighted images were acquired using a 3T scanner (Philips Achieva, Best, Netherlands) using the following scanning protocol: TR, 12 s; TE, 156 ms; voxel size, 0.8 x 0.8 x 1.6 mm3; and reconstruction size, 0.5 x 0.5 x 0.5 mm3.
One radiologist performed visual analysis of dPVS in basal ganglia (BGdPVS) and white matter (WMdPVS), using five-point scales: grade 0, 0 dPVS; grade 1, 1-10 dPVS; grade 2, 11-20 dPVS; grade 3, 21 – 40 dPVS; and grade 4 , > 40 dPVS. For BGdPVS, we excluded perforated substances at the level and below the anterior commissure.
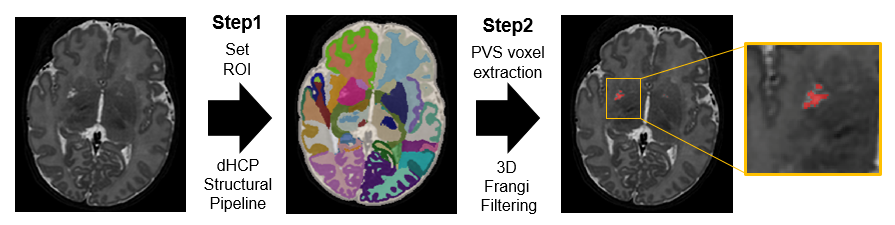
For volumetric analysis, we first segmented the brain regions using Developing Human Connectome project structural pipeline, and then segmented dPVS using Frangi filtering with experimentally determined thresholding value5. Fraction of dPVS was calculated by dividing dPVS volume by the region's brain volume (Figure 2).
We compared dPVS extent according to gender and GA at birth (preterm group, < 37 weeks; term group, ≥ 37 weeks) using Mann-Whitney test. We evaluated the association between GA and dPVS volume and GA and dPVS fraction using linear regression. Both GA at birth and GA at MRI scan were used for the analysis.
Result
A total of 244 neonates (median GA at birth, 39 weeks; 145 boys and 99 girls) were evaluated including 88 neonates in the preterm group (median GA at birth, 33 weeks) and 156 neonates in the term group (median GA at birth, 40 weeks). On demographic data comparison, there was no significant difference between the two groups regarding gender (P = 0.892) and GA at MRI scan (P = 0.172).On visual analysis, most neonates showed WMdPVS grade 0 (227/244) and all neonates showed BGdPVS grade 0 (90/244) or grade 1 (154/244). Preterm neonates showed lower BGdPVS visual grade compared to term neonates (median grade, 0 vs. 1, P < 0.001).
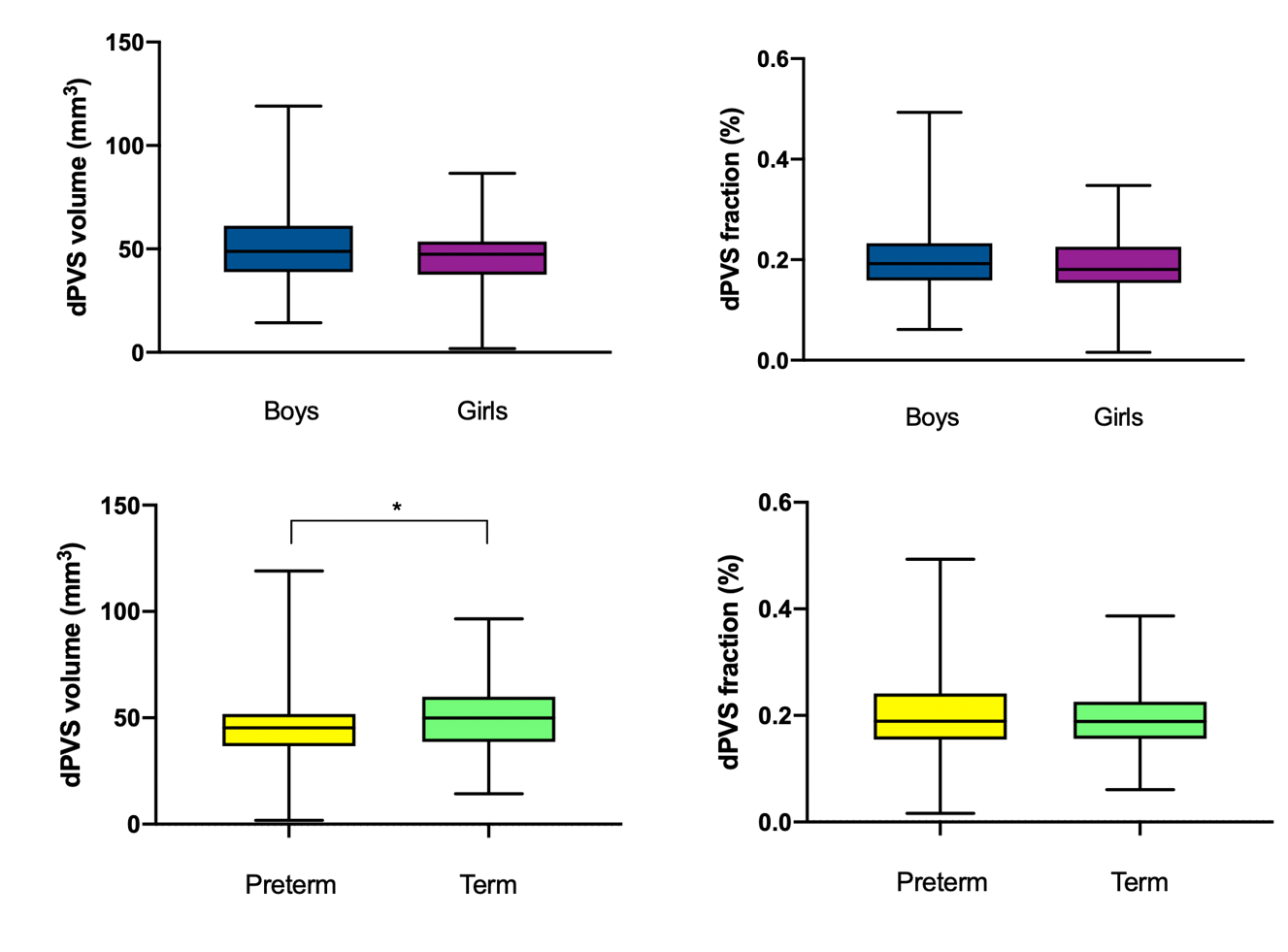
Since most neonates did not show WMdPVS, only BGdPVS were further evaluated for volumetric analysis. Overall median (interquartile range) of BGdPVS volume and fraction were 48.2 mm3 (37.8 mm3 – 59.0 mm3) and 0.189 % (0.155 %– 0.232 %), respectively. There was no significant difference of BGdPVS volume (P = 0.069) and fraction (P = 0.282) according to gender (Figure 3). When preterm and term groups were compared, BGdPVS volume in preterm neonates was significantly lower than that in term neonates (45.3 mm3 vs. 49.9 mm3, P = 0.040) (Figure 3). However, BGdPVS fraction did not show significant difference between the two groups (0.2 % vs. 0.2 %, P = 0.622) (Figure 3). When association with GA at birth was evaluated, there was a significant positive relationship between GA at birth and BGdPVS volume (coefficient = 0.603, P = 0.012). GA at MRI scan and BGdPVS fraction showed a negative relationship (coefficient = - 0.008, P < 0.001) (Figure 4).
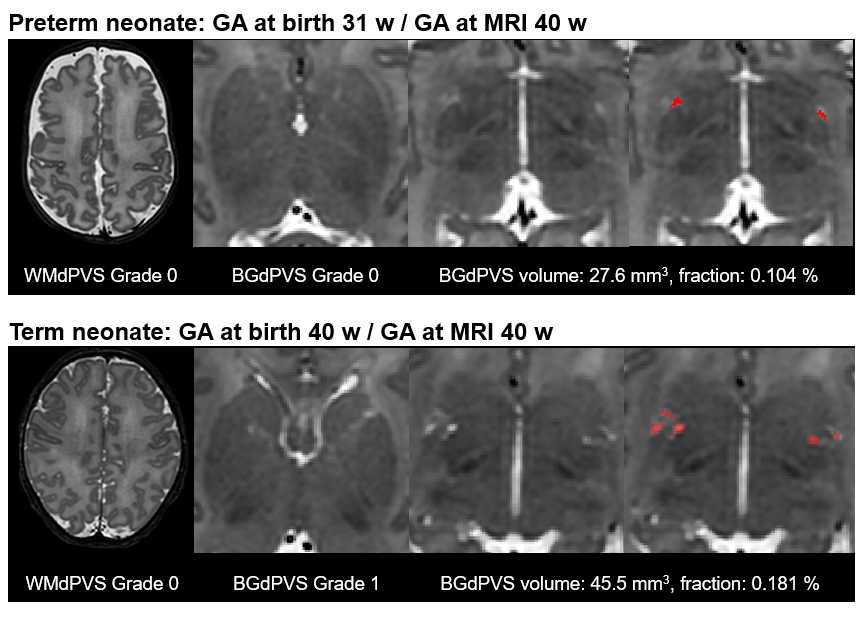
Representative cases are shown in Figure 5. A preterm neonate (upper row) showed lower visual grade and volume of BGdPVS compared to those of a term neonate (lower row). Both neonates did not show WMdPVS.
Discussion
Both visual grades and volume of dPVS increased with age in previous studies, however, a recent report showed dPVS decrease with age in a young population6. Our results showing lower dPVS extent in preterm neonates than that in term neonates needs careful interpretation. Since preterm neonates’ brains in term-equivalent age generally show underdevelopment compared to that in term neonates, lower dPVS extent in preterm neonates can also be interpreted as an underdeveloped glymphatic system in this group. Smaller dPVS fraction according to GA at MRI scan suggests that the regional brain volume increase exceeds the dPVS volume increase with age in neonates.Conclusion
In neonates, dPVS were rarely observed in the white matter but commonly observed in the basal ganglia. Gender did affect dPVS extent in neonates and preterm neonates showed lower dPVS extent than term neonates. We showed that dPVS extent, which reflects the glymphatic system in the brain, was affected by preterm birth.Acknowledgements
Hyun Gi Kim has received funding from the National Research Foundation of Korea (NRF-2021R1A2C1007831)References
1. Park YW, Shin NY, Chung SJ, et al. Magnetic Resonance Imaging-Visible Perivascular Spaces in Basal Ganglia Predict Cognitive Decline in Parkinson's Disease. Mov Disord. 2019;34:1672-1679.
2. Granberg T, Moridi T, Brand JS, et al. Enlarged perivascular spaces in multiple sclerosis on magnetic resonance imaging: a systematic review and meta-analysis. J Neurol. 2020;267:3199-3212.
3. Liu C, Habib T, Salimeen M, et al. Quantification of visible Virchow–Robin spaces for detecting the functional status of the glymphatic system in children with newly diagnosed idiopathic generalized epilepsy. 2020;78:12-17.
4. Hughes EJ, Winchman T, Padormo F, et al. A dedicated neonatal brain imaging system. 2017;78:794-804.
5. Frangi AF, Niessen WJ, Vincken KL, et al. Multiscale vessel enhancement filtering. International conference on medical image computing and computer-assisted intervention, 1998. Springer: 130-137.
6. Kim HG, Kim J, Shin NY. Life span changes of dilated perivascular spaces: A normal population-based study, RSNA 2020, Chicago
Figures