3717
Imaging evaluation of pediatric IgAN and HSPN based on ASL and mDIXON-Quant1Radiology, Beijing Children's Hospital, Capital Medical University, National Center for Children's Health, Beijing, China, 2Beijing Children's Hospital, Capital Medical University, National Center for Children's Health, Beijing, China, 3Philips Healthcare, Beijing, China
Synopsis
It is difficult to identify IgA nephropathy (IgAN) and Henoch Schonlein purpura nephritis (HSPN) due to their similar image features on conversional MR anatomic images. Arterial spin labeling (ASL) and mDIXON-Quant MR imaging can provide more data about perfusion and relaxation time to evaluate the functional state of kidney. In this study, we explore to different IgAN from HSPN in pediatric patients with nephropathy using ASL and mDIXON-Quant MR sequences, and hope to improve accuracy in differential diagnosis of IgAN and HSPN.
Introduction
Pediatric nephropathies are common diseases in children with chronic abdominal diseases. Without timely and effective treatment, it may progresse to chronic kidney diseases with poor prognoses1-2. As the two main kinds of pediatric nephropathy, the clinical characteristics and laboratory results of IgA nephropathy (IgAN) and Henoch Schonlein purpura nephritis (HSPN) are similar. Although the diagnosis can be confirmed by renal biopsy, puncture biopsy is invasive examination with poor repeatability and poor patient compliance, and is unable to further assess the patient’s condition3. As a functional sequence of Functional magnetic resonance imaging (fMRI) 4-8, arterial spin labeling (ASL) and mDIXON-Quant can be used to evaluate renal blood flow and renal oxygenation capacity, respectively. The purpose of this study is to investigate the feasibility in differentiating IgAN from HSPN using ASL and mDIXON-Quant.Methods
Twenty-five pediatric patients with nephropathy (IgAN, 12 cases; HSPN, 13 cases) for kidney examinations were performed on a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, the Netherlands) using 32 channel abdominal coil. The MR protocol consisted of T1WI, T2WI, ASL and mDIXON-Quant, the detailed information were shown in Table 1. The images of ASL and mDIXON-Quant were processed in Philips’s workstation (ISP, Philips Healthcare, the Netherlands). ROIs of renal cortex and medulla were delineated with manual contouring. Renal blood flow (RBF) and R2* values were measured on ASL and mDIXON-Quant, respectively. Independent Student's T test or Mann-Whitney U test were used to analyze the possible group differences between IgAN and HSPN. The ROC curve of the above parameters was ploted to analyze the diagnostic efficiency between IgAN and HSPN. P values < 0.05 were considered significant.Results
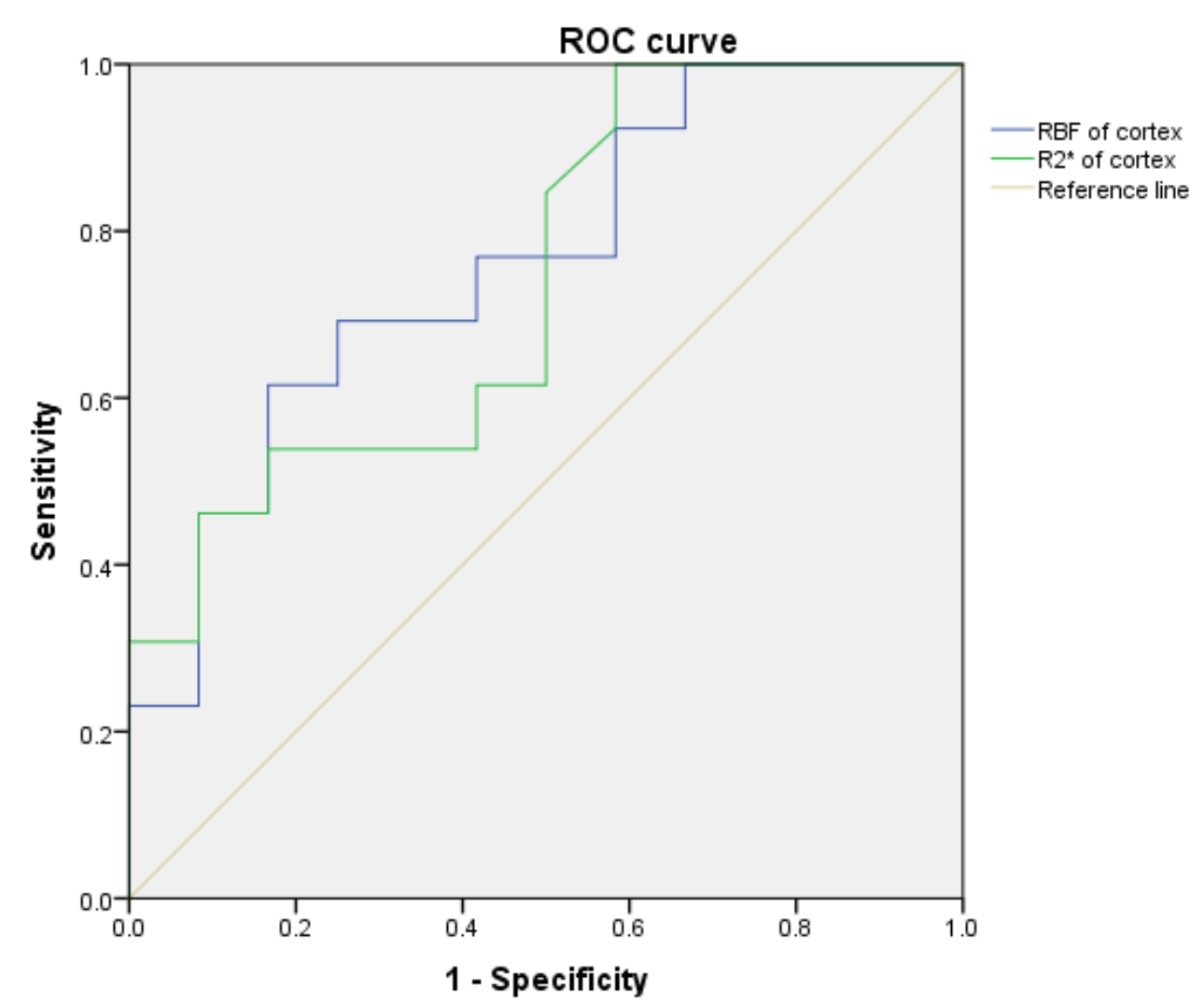
Corresponding parameter mapping of ASL and mDIXON-Quant were showed in Figure 1. The RBF and R2* values of renal cortex in HSPN group were higher, when compared with IgAN group (P=0.017 and 0.025 respectively) in Table 2 and 3. The area under the ROC cuvers (AUCs) of RBF of cortex and R2* of cortex were 76.3% and 74.0% for identify IgAN and HSPN, respectively (Table 4 and Figure 2). The sensitivity of the above parameters with feasible thresholds were 61.5% and 100%, the corresponding specificity were 83.3% and 41.7%.Discussion
Previous studies have shown that ASL and mDIXON-Quant are associated with renal perfusion and diffusion4,6-8. Higher RBF value of renal cortex in HSPN patients was found compared with those in IgAN based on ASL and mDIXON-Quant. These results were consistent with the reported literature9. Although the pathogenesis of IgAN and HSPN is similar, their pathological changes are different. Studies9 have shown that IgAN has more serious renal lesions than HSPN, and the incidence of renal insufficiency is higher. However, in this study, the degree of renal cortical hypoxia in patients with HSPN was higher than that in patients with IgAN, which is different from previous study9, and the results also means that the lesion degree of renal cortex in HSPN patients was higher than that in IgAN patients. We speculate that there may be associated with the number of cases and the data measurement method.Conclusions
ASL and mDIXON-Quant can significantly distinguish diagnosis of IgAN and HSPN. This result revealed that value of RBF and R2* may evaluate the progression and prognosis of pediatric nephropathy in the further study.Acknowledgements
No.References
[1] Rodrigues JC, Haas M, Reich HN. IgA Nephropathy. Clin J Am Soc Nephrol. 2017;12(4):677-686.
[2] Zheng X, Chen Q, Chen L. Obesity is associated with Henoch-Schönlein Purpura Nephritis and development of end-stage renal disease in children. Ren Fail. 2019;41(1):1016-1020.
[3] Corapi KM, Chen JL, Balk EM, Gordon CE. Bleeding complications of native kidney biopsy: a systematic review and meta-analysis. Am J Kidney Dis. 2012;60(1):62-73.
[4] Zhang JL, Rusinek H, Chandarana H, et al. Functional MRI of the kidneys. J Magn Reson Imaging. 2013;37(2):282-293.
[5] Zhang JL, Lee VS. Renal perfusion imaging by MRI. J Magn Reson Imaging. 2020;52(2):369-379.
[6] Zhang JL, Morrell G, Rusinek H, et al. New magnetic resonance imaging methods in nephrology. Kidney Int. 2014;85(4):768-778.
[7] Mahmoud H, Buchanan C, Francis ST, Selby NM. Imaging the kidney using magnetic resonance techniques: structure to function. Curr Opin Nephrol Hypertens. 2016;25(6):487-493.
[8] Neugarten J, Golestaneh L. Blood oxygenation level-dependent MRI for assessment of renal oxygenation. Int J Nephrol Renovasc Dis. 2014; 7:421-435.
[9] Calvo-Río V, Loricera J, Martín L, et al. Henoch-Schönlein purpura nephritis and IgA nephropathy: a comparative clinical study. Clin Exp Rheumatol. 2013;31(1 Suppl 75): S45-S51.
Figures
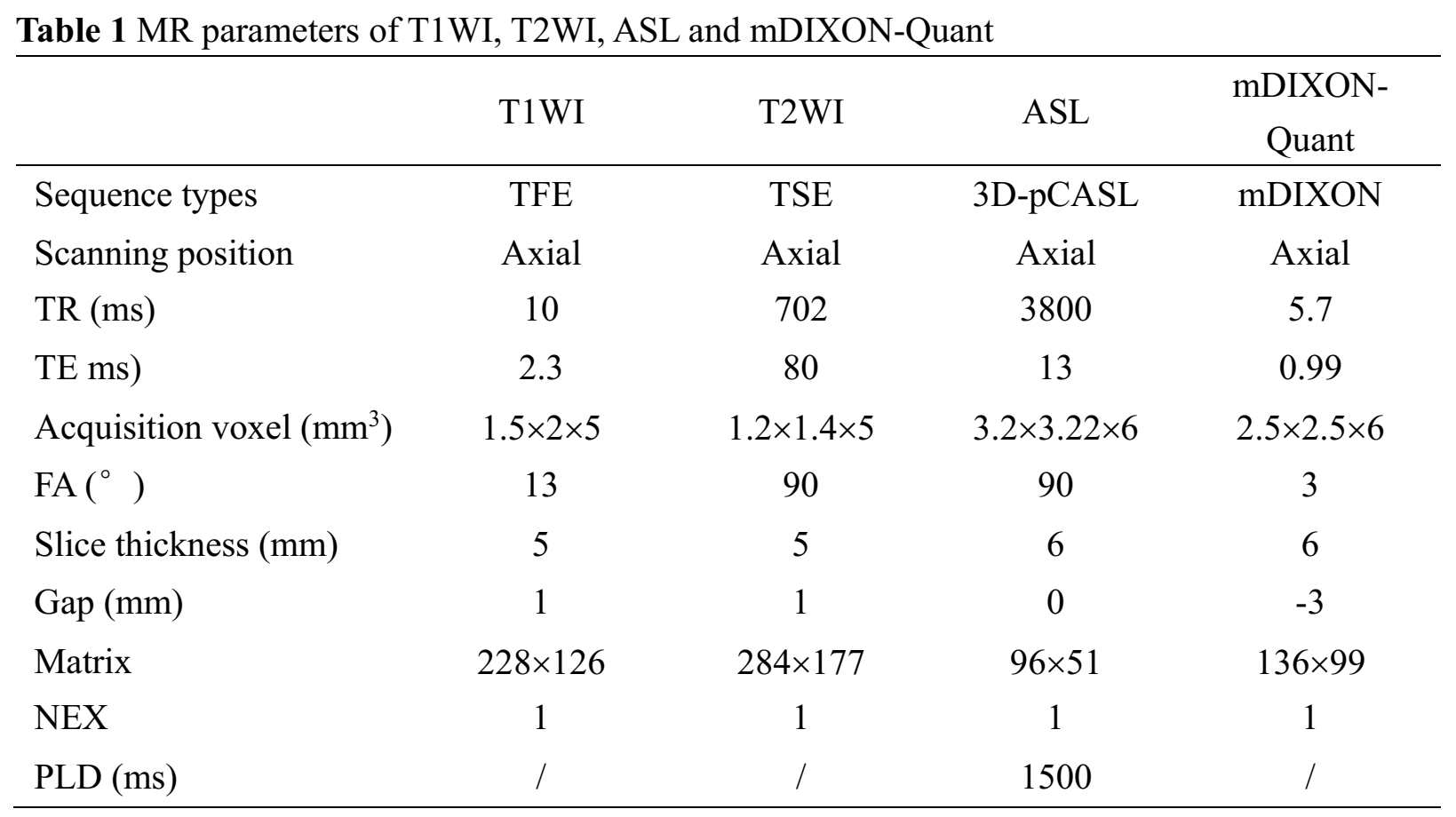
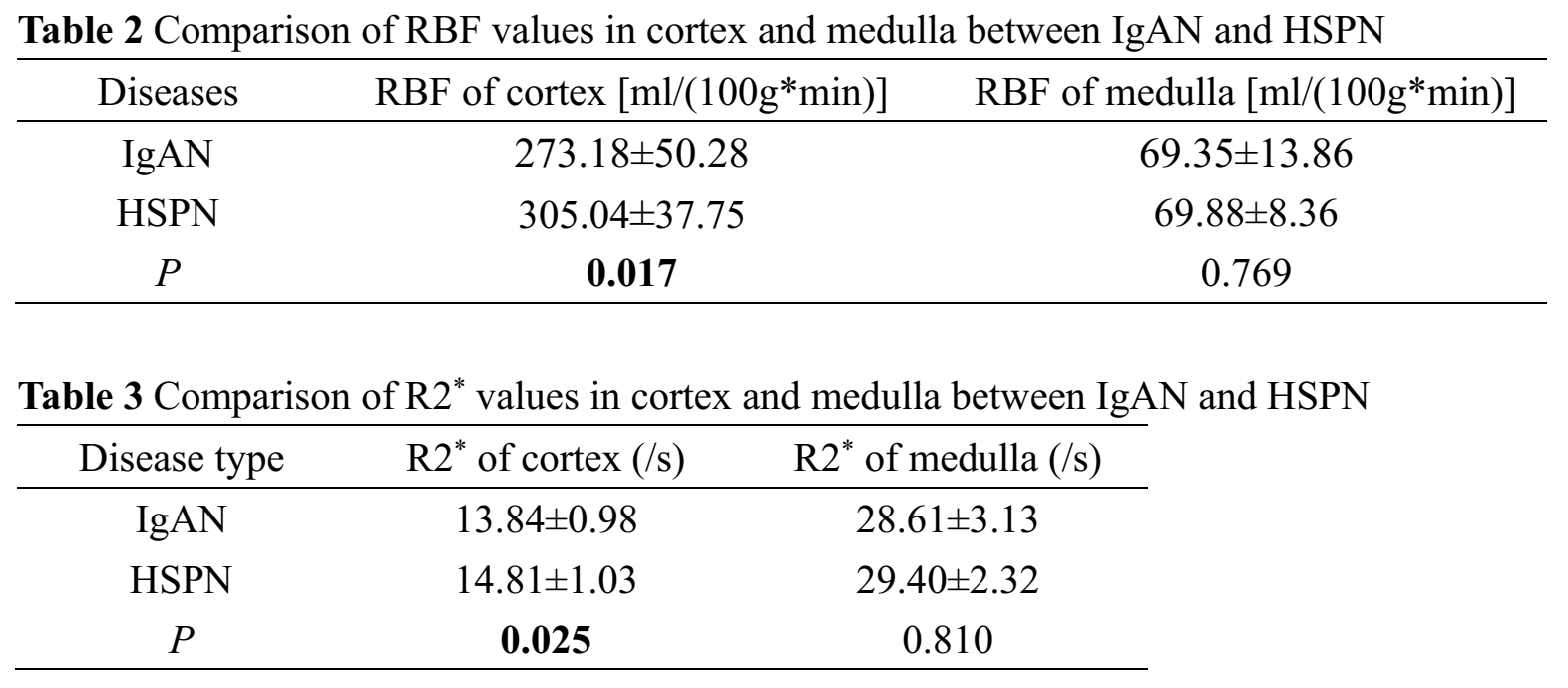
Table 2: Comparison of RBF values in cortex and medulla between IgAN and HSPN.
Table 3: Comparison of R2* values in cortex and medulla between IgAN and HSPN.

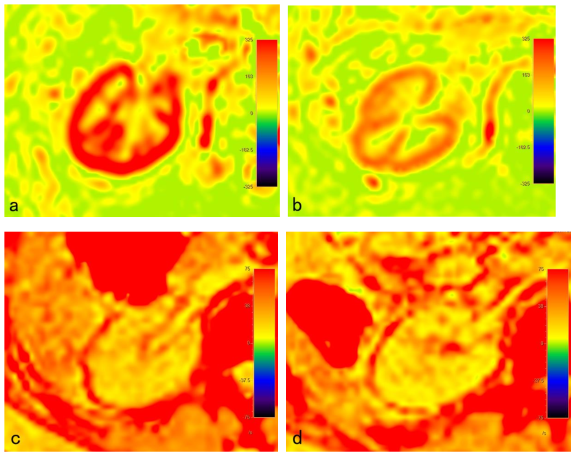
Figure 1. a. A 16.3 years old boy with HSPN. b. A 13.5 years old boy with IgAN. The RBF value of renal cortex in HSPN patient was significantly higher than that in IgAN, indicating that the blood perfusion was higher.
c. A 12.7 years old girl with HSPN. d. A 13.9 years old boy with IgAN. Hypoxia in renal cortex of HSPN patient was more common than that of IgAN patient.