3713
Accelerated high-resolution T2-weighted imaging for prostate with a deep learning constrained Compressed SENSE reconstruction1Philips Japan, Tokyo, Japan, 2Tokyo Metropolitan Police Hospital, Nakano, Japan, 3Philips Healthcare, Best, Netherlands
Synopsis
T2-weighted (T2W) imaging is used to depict prostate anatomy. However, T2W imaging with high spatial resolution, which is required by PI-RADSv2, is not always performed because of the long scan time. In this study, we investigated the use of Compressed SENSE AI (CS-AI) reconstruction to accelerate high-resolution T2W imaging of the prostate. The image quality of CS-AI reconstruction, conventional Compressed-SENSE (C-SENSE), and SENSE were compared qualitatively and quantitatively. Clinical cases demonstrated a significant noise reduction in accelerated CS-AI. CS-AI also showed a significantly higher contrast-to-noise ratio in CS-AI compared to SENSE and C-SENSE.
Introduction
MRI plays an important role in the diagnosis and staging of prostate cancer patients. In particular, high-resolution T2-weighted (T2W) imaging is used to depict prostate anatomy and assess extraprostatic extension (EPE)1. To standardize imaging protocols and reduce variability in multiparametric prostate MRI (mpMRI), the minimum technical standard for prostate MR imaging was established by Prostate Imaging Reporting and Data Systems (PI-RADS)2. However, recent reports indicated that there are variations among facilities in their adherence to the minimum technical standards for PI-RADSv23–6. Among acquisition parameters, adherence to frequency resolution (≤ 0.4 mm) and phase resolution (≤ 0.7 mm) in T2W turbo spin echo (TSE) imaging were particularly low3,6. This is because comprehensive mpMRI protocol with high-resolution imaging prolongs examination time to such an extent that it is not feasible in clinical practice. Although many scan acceleration techniques, such as parallel imaging7 and compressed sensing8 have been developed, the use of high acceleration factors may result in too much noise breakthrough.In this study, Compressed SENSE AI (CS-AI) reconstruction9,10 was used to acquire high-resolution T2W images while accelerating the scan compared to parallel imaging (SENSE). It is hypothesized that the image quality of high-resolution T2W imaging can be significantly improved while accelerating the scan by using the CS-AI reconstruction algorithm. The purpose of this study was to acquire accelerated high-resolution T2W images for the prostate using the CS-AI reconstruction and quantitatively compare the image quality with SENSE and conventional Compressed-SENSE (C-SENSE).
Methods
The study was approved by the local IRB, and written informed consent was obtained from all subjects. A total of 14 patients were examined on a 3.0T whole-body clinical system (Ingenia Elition X, Philips Healthcare) using a 32-channel phased-array coil. Multi-slice 2D T2W TSE sequence was acquired in the axial plane.The image quality was compared between three acceleration methods: SENSE, C-SENSE, and CS-AI. SENSE images were acquired with acceleration factor 2 and the scan time was 3:04 min. C-SENSE and CS-AI images were acquired with acceleration factor 3 and the scan time was 2:15 min. Following parameters were common to all examinations: FOV=200x200 mm2, slice thickness=3 mm, no intersection gap, 20 slices, in-plane acquisition resolution 0.4×0.6 mm2, in-plane reconstruction resolution 0.2×0.2 mm2, TR/TE=7386/98ms, number of signals averaged (NSA)=1.
The image quality was quantitatively evaluated by calculating the contrast-to-noise ratio (CNR). First, oval regions of interest (ROI) were placed on SENSE image in three areas; transitional zone (TZ), outer peripheral zone (PZ), and obturator internus muscle as a proxy for background (bg). The ROIs were then copied to C-SENSE and CS-AI images. The CNR was defined as:
$$CNR={ROI_{organ} - ROI_{bg} \above{1pt}\sqrt{\frac 1 2\times(SD_{organ}^2+SD_{bg}^2)}}$$
where ROIorgan and ROIbg are the averages of signal intensity measured in the prostate (i.e. TZ or PZ) and background ROIs, respectively, and SDorgan and SDbg are the standard deviations in the prostate and background ROIs, respectively. Paired t-tests were performed to determine statistical significance between scan acceleration techniques. P ≤ 0.05 was considered statistically significant.
The CS-AI model used in this study is the extension of the previously introduced AI-based reconstruction algorithm, Adaptive-CS-Net9,10. In CS-AI, the iterative optimization procedure in the C-SENSE reconstruction chain is unrolled for a fixed number of reconstruction blocks. Each block consists mainly of Unet-like architecture, which performs as a denoiser. The model was trained on more than 700,000 images, including 2D and 3D data, and multiple contrasts and anatomical areas.
Results and Discussions
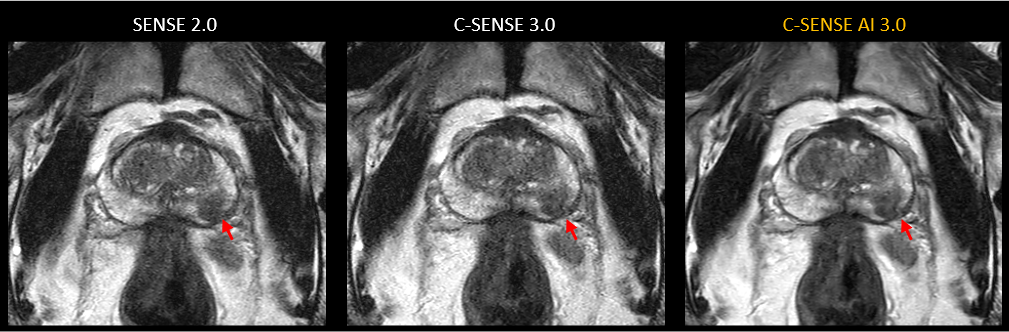
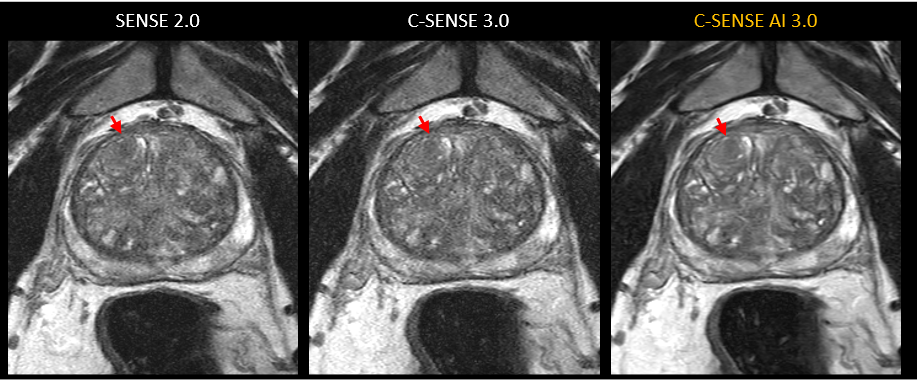
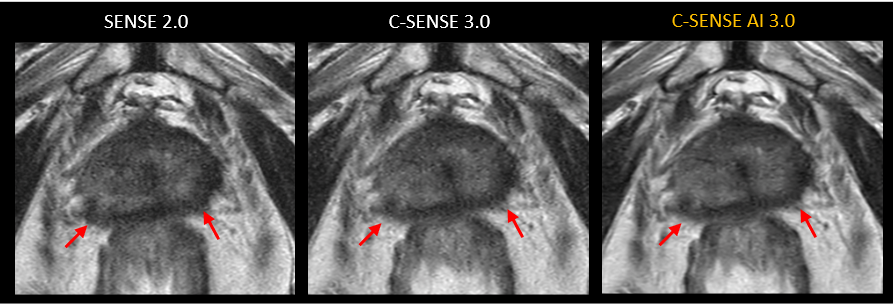
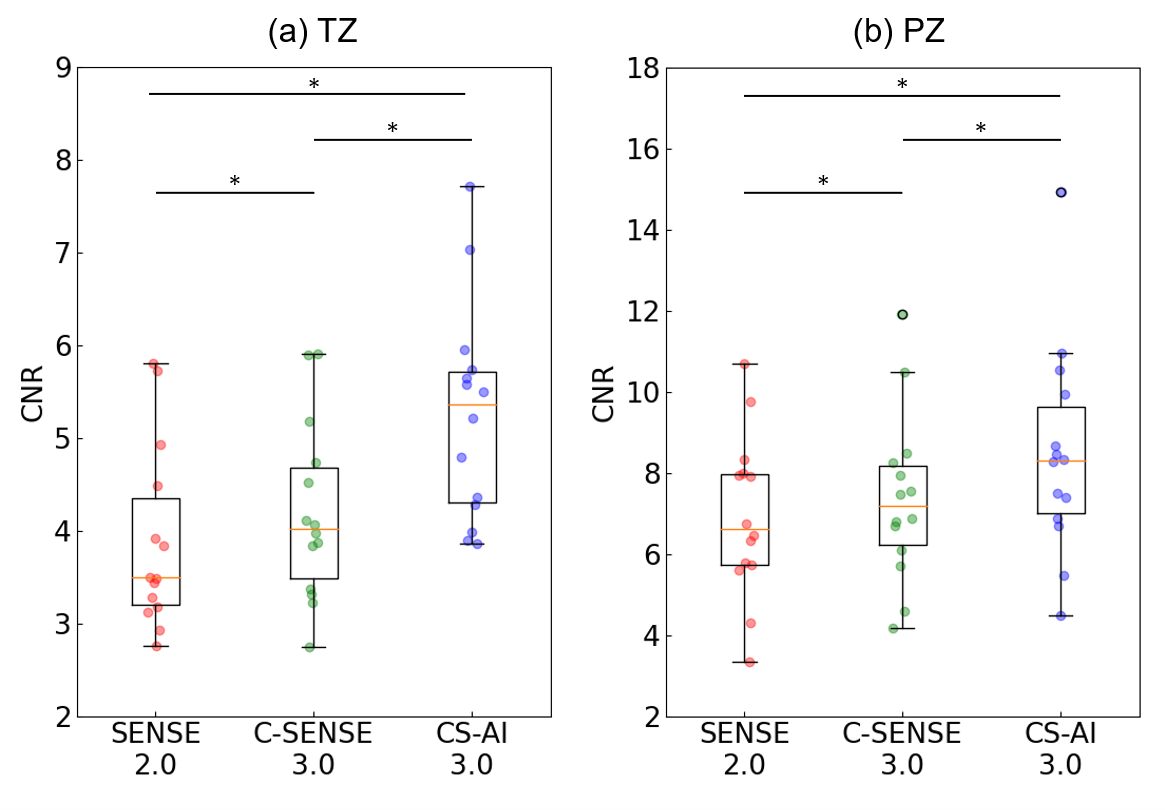
Figures 1 to 4 show comparison of SENSE (acceleration factor 2.0), C-SENSE (acceleration factor 3.0), and CS-AI (acceleration factor 3.0) for axial high-resolution T2W images. Overall, SENSE and C-SENSE images became very noisy and were not suitable for diagnosis. However, the CS-AI significantly reduced the noise and produced visually sharper images, which led to the better depiction of small structures. The contrast inside the TZ and the PZ improved visually on CS-AI.Figure 5 (a) and (b) show the CNR comparison between SENSE, C-SENSE, and CS-AI, measured on TZ and PZ, respectively. The average CNR were 3.89, 4.20, and 5.26 in the TZ, and were 6.93, 7.37, and 8.47 in the PZ for SENSE, C-SENSE, and CS-AI, respectively. The differences of the average CNR between three sequences were all statistically significant for both TZ (SENSE vs C-SENSE: p=0.003, SENSE vs C-SENSE: p<0.001, and C-SENSE vs CS-AI: p<0.001) and PZ (SENSE vs C-SENSE: p=0.004, SENSE vs C-SENSE: p<0.001, and C-SENSE vs CS-AI: p<0.001). It has to be noted that the CS-AI demonstrated superior image quality compared to SENSE despite having a higher acceleration factor, i.e. k-space undersampling rate. Scan time reduction in CS-AI compared to SENSE may have suppressed possible motion artifacts and improved the image quality. However, quantitative evaluation also showed CS-AI to have better image quality than C-SENSE, which was acquired at the same scan duration as CS-AI. These results suggest that the CS-AI can acquire high-resolution T2W images while significantly accelerating the scan and improving the image quality.
Conclusion
High-resolution T2W images for the prostate were acquired with SENSE and accelerated C-SENSE and CS-AI reconstruction. Clinical examples demonstrated significant noise reduction in accelerated CS-AI. The quantitative evaluation showed substantially higher CNR in CS-AI compared to SENSE and C-SENSE.Acknowledgements
No acknowledgement found.References
1. Israël B, Leest M van der, Sedelaar M, Padhani AR, Zámecnik P, Barentsz JO. Multiparametric Magnetic Resonance Imaging for the Detection of Clinically Significant Prostate Cancer: What Urologists Need to Know. Part2: Interpretation. Eur Urol. 2020;77(4):469-480. doi:10.1016/j.eururo.2019.10.024
2. Weinreb JC, Barentsz JO, Choyke PL, et al. PI-RADS Prostate Imaging – Reporting and Data System: 2015, Version 2. Eur Urol. 2016;69(1):16-40. doi:10.1016/j.eururo.2015.08.052
3. Esses SJ, Taneja SS, Rosenkrantz AB. Imaging Facilities’ Adherence to PI-RADS v2 Minimum Technical Standards for the Performance of Prostate MRI. Acad Radiol. 2018;25(2):188-195. doi:10.1016/j.acra.2017.08.013
4. Cuocolo R, Stanzione A, Ponsiglione A, et al. Prostate MRI technical parameters standardization: A systematic review on adherence to PI-RADSv2 acquisition protocol. Eur J Radiol. 2019;120(August):108662. doi:10.1016/j.ejrad.2019.108662
5. Burn PR, Freeman SJ, Andreou A, Burns-Cox N, Persad R, Barrett T. A multicentre assessment of prostate MRI quality and compliance with UK and international standards. Clin Radiol. 2019;74(11):894.e19-894.e25. doi:10.1016/j.crad.2019.03.026
6. Sackett J, Shih JH, Reese SE, et al. Quality of Prostate MRI: Is the PI-RADS Standard Sufficient? Acad Radiol. 2021;28(2):199-207. doi:10.1016/j.acra.2020.01.031
7. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: Sensitivity encoding for fast MRI. Magn Reson Med. 1999;42(5):952-962. doi:10.1002/(SICI)1522-2594(199911)42:5<952::AID-MRM16>3.0.CO;2-S
8. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007;58(6):1182-1195. doi:10.1002/mrm.21391
9. Pezzotti N, de Weerdt E, Yousefi S, et al. Adaptive-CS-Net: FastMRI with Adaptive Intelligence. arxiv. 2019;(NeurIPS). http://arxiv.org/abs/1912.12259
10. Pezzotti N, Yousefi S, Elmahdy MS, et al. An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction. IEEE Access. 2020;8:204825-204838. doi:10.1109/ACCESS.2020.3034287
Figures