3711
Feasibility of synthetic short TR and short TE DWI in prostate cancer1Philips Japan, Ltd., Tokyo, Japan, 2Department of Radiology, Kawasaki Medical School, Okayama, Japan, 3Philips Healthcare, Asia Pacific, Tokyo, Japan
Synopsis
Diffusion-weighted imaging (DWI) with shorter echo time (TE) could be exploited to improve diffusion contrast by minimizing T2 shine-through due to longer T2 in normal prostate. However, clinical magnetic resonance imaging (MRI) scanner has limitation in shortening TE in conventional DWI. It would be beneficial to generate additional DWI with short TE from DWIs with two different TE, in addition to short repetition time (TR) which improvement of diffusion contrast has been reported. The synthetic DWI with shorter TR (1000 ms) and TE (1 ms) tended to show better diffusion contrast than real-acquired DWI with conventional TR and TE.
Introduction
Multiparametric magnetic resonance imaging (mp-MRI) has been widely accepted in prostate MRI. However, there is a problem that 10-15% of clinically significant prostate cancer (PCa) are still missed using mp-MRI1-3. Therefore, diagnostic performance of prostate MRI needs to be improved.Recently, it has been reported that diffusion-weighted imaging (DWI) with shorter repetition time (TR) can improve diffusion contrast compared to conventional (long) TR4, utilizing the specific feature that T1 of PCa is lower than that of normal prostate tissue (NPT)5, 6. However, one challenge of short TR acquisition is low signal-to-noise ratio (SNR). Therefore, we have proposed to generate an additional DWI with shorter TR (e.g. 1000 ms) from DWIs with two different TR. Our preliminary results showed synthetic DWI with shorter TR tends to have better diffusion contrast compared to real-acquired DWI with long TR7.
It is also well known that T2 in PCa is shorter than NPT5, 6, 8. Although it is expected that shorter echo time (TE) DWI could be exploited to improve diffusion contrast by minimizing T2 shine-through due to longer T2 in NPT, standard clinical MRI scanner has limitation in shortening TE in conventional spin echo (SE) type DWI. Therefore, we explored the possibility of generating an additional DWI with shorter TE (e.g. 1 ms) from DWIs with two different TE (e.g. conventional and long TE such as 70 and 140 ms) in addition to DWI with shorter TR (Figure 1). We refer to this as synthetic short TR and short TE DWI (synDWI). The goal of this study is to investigate clinical feasibility of synDWI.
Methods
Our Institutional Review Board approved this retrospective study and waived the need for informed consent. Seven patients underwent mp-MRI on Ingenia Elition 3.0T (Philips Healthcare, Best, The Netherlands). Two DWI sequences were scanned with (1) long TR with dual echo and (2) short TR with single echo. The detailed imaging parameters are described in Figure 2. synDWI can be calculated on a pixel-by-pixel basis from DWIs with two different TR and two different TE, following the procedure below.The signal intensity (SI) of SE type DWI is given by
$$SI=\alpha\cdot PD\cdot (1-e^{-TR/T1})\cdot e^{-TE/T2}\cdot e^{-b\cdot D}\left(1\right)$$
where α is proportionality factor. The T1 value can be determined dividing equations 2 and 3 in b0 image, keeping TE and b constant, and the T2 value can be determined dividing equations 2 and 4 in b0 image, keeping TR and b constant:
$$SI\>in\>DWI\>with\>long\>TR\>and\>short\>TE=\alpha\cdot PD\cdot (1-e^{-long\>TR/T1})\cdot e^{-short\>TE/T2}\cdot e^{-b\cdot D}\left(2\right)$$
$$SI\>in\>DWI\>with\>short\>TR\>and\>short\>TE=\alpha\cdot PD\cdot (1-e^{-short\>TR/T1})\cdot e^{-short\>TE/T2}\cdot e^{-b\cdot D}\left(3\right)$$
$$SI\>in\>DWI\>with\>long\>TR\>and\>long\>TE=\alpha\cdot PD\cdot (1-e^{-long\>TR/T1})\cdot e^{-long\>TE/T2}\cdot e^{-b\cdot D}\left(4\right)$$
Next, the [α ∙ PD ∙ diffusion term] factor can be calculated using the SI, rewriting equation 2 as
$$\alpha\cdot PD\cdot e^{-b\cdot D}=SI\>in\>DWI\>with\>long\>TR\>and\>short\>TE/\left[(1-e^{-long\>TR/T1})\cdot e^{-short\>TE/T2}\right]\left(5\right)$$
Finally, SI in DWI at b-values of 1000 and 2000 s/mm2 (DWI1000 and DWI2000) with any TR and any TE can be calculated according to equation 1.
synDWI1000 and synDWI2000 with TR of 1000, 2000, 4000 and 6000 ms were calculated. At each TR, synDWI1000 and synDWI2000 were generated with TE of 1, 50, 75, 100, 150, and 200 ms. Contrast ratio (CR) in synDWI at TE of 75ms with TR of 1000, 2000, 4000, and 6000 ms were compared. Next, CR in synDWI with TE of 1, 50, 75, 100, 150, and 200 ms using the TR with the highest CR were compared. Moreover, CR and visual score were compared between synDWI with the combination of TR and TE with the highest CR, and real-acquired DWI with TR of 6000ms and TE of 70 ms.
- CR=(SIPCa-SINPT)/(SIPCa+SINPT)
where SIPCa and SINPT are the average signal intensity in PCa and NPT. - Visual score for comparison of contrast between PCa and NPT was conducted by a radiologist with twenty-four years of experience in MRI. It was graded using a 5-point scale.
Results and Discussion
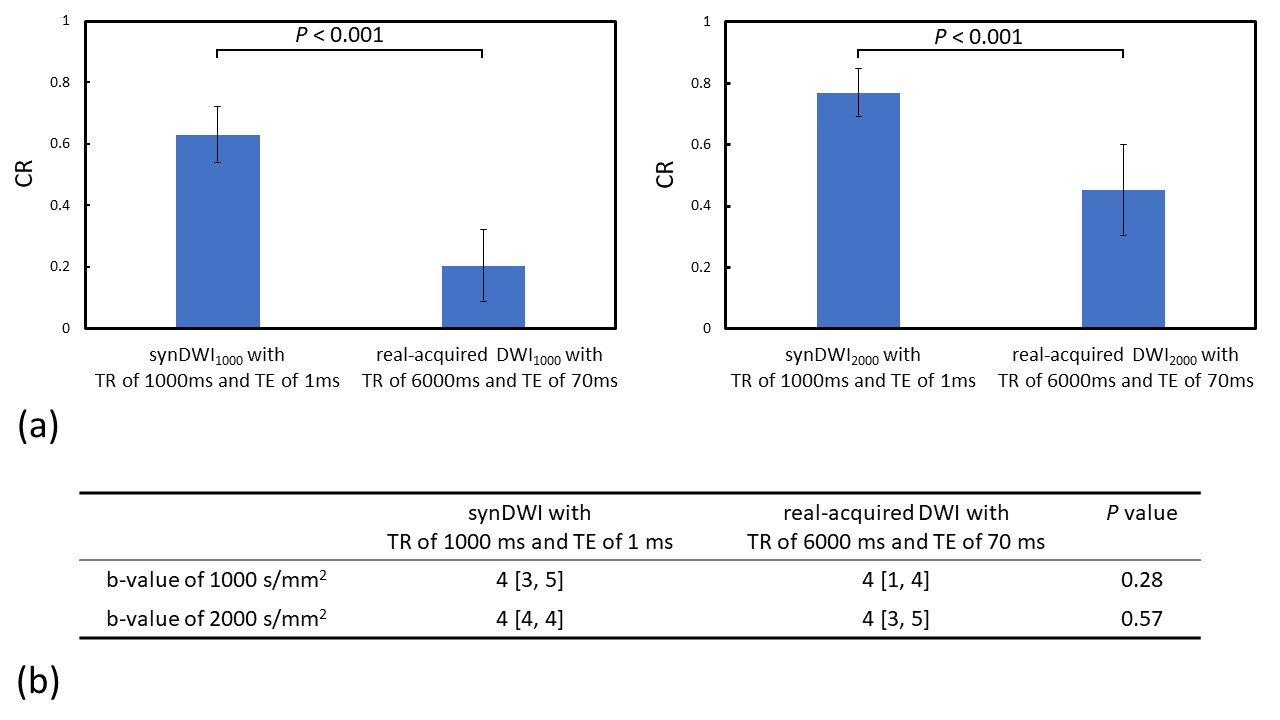
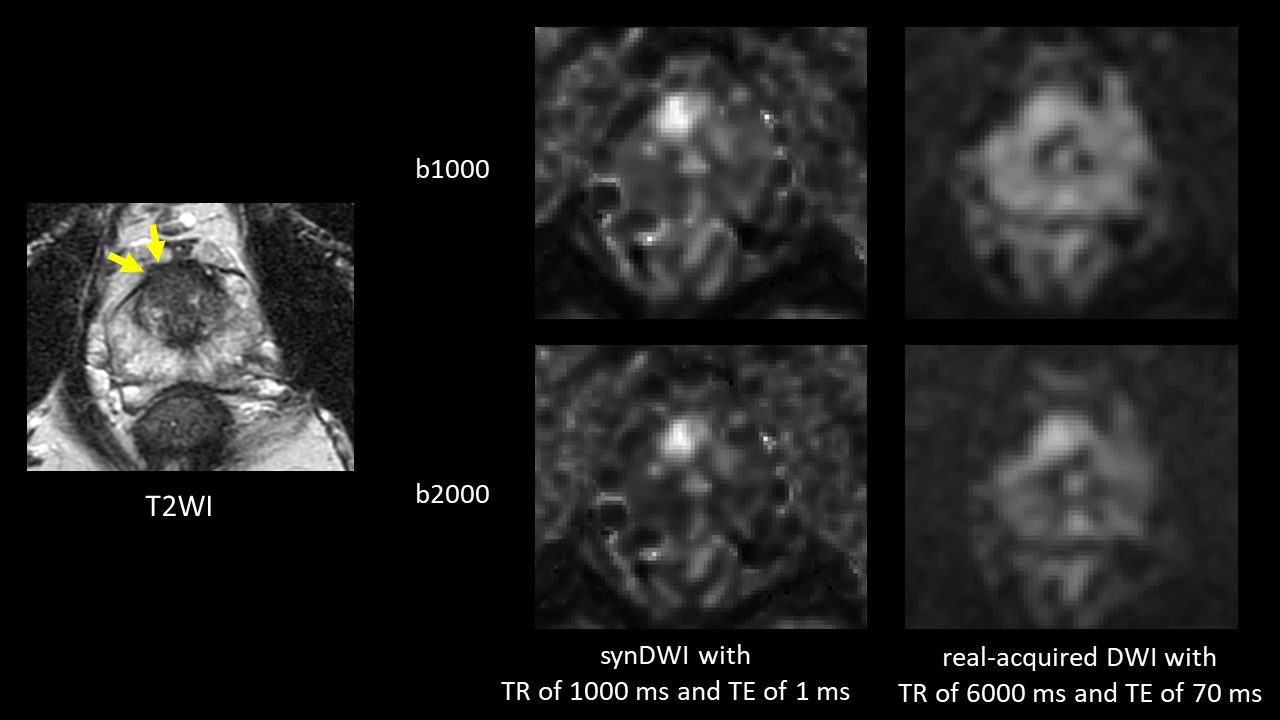
CR in synDWI for both b-values showed significantly higher value in shorter TR (P < 0.001 for both b-values, Figure 3a) and shorter TE (P < 0.001 for both b-values, Figure 3b). The combination of TR of 1000 ms and TE of 1 ms showed the highest CR. CR in synDWI for both b-values with TR of 1000 ms and TE of 1 ms was significantly higher than that of real-acquired DWI for both b-values with TR of 6000 ms and TE of 70 ms (P < 0.001 for both b-values, Figure 4a). Although visual score in synDWI for both b-values with TR of 1000 ms and TE of 1 ms tended to show higher value than that of real-acquired DWI for both b-values with TR of 6000 ms and TE of 70 ms, there was no significant difference (P = 0.28 for b1000 and P = 0.56 for b2000, Figure 4b). These results indicated that shorter TR and shorter TE had improved clinical value of DWI, probably thanks to shorter T1 and shorter T2 in PCa compared to NPT. Figure 5 shows representative clinical case with PCa.Conclusion
Our preliminary results show that synDWI with shorter TR of 1000 ms and shorter TE of 1 ms tended to have better diffusion contrast compared to real-acquired DWI with conventional TR and TE.Acknowledgements
No acknowledgement found.References
- Kido A, Tamada T, Kanomata N, et al. Multidimensional analysis of clinicopathological characteristics of false‑negative clinically significant prostate cancers on multiparametric MRI of the prostate in Japanese men. Jpn J Radiol 2019; 37: 154-64.
- Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. Lancet 2017; 389: 815-22.
- Schoots IG, Roobol MJ, Nieboer D, et al. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: a systematic review and meta-analysis. Eur Urol 2015; 68: 438-50.
- Ueda Y, Tamada T, Yoshida K, et al. Short TR DWI in prostate. Proceedings of the 28th Annual Meeting of ISMRM, 2020 #2423.
- Shiradkar R, Panda A, Leo P, et al. T1 and T2 MR fingerprinting measurements of prostate cancer and prostatitis correlate with deep learning-derived estimates of epithelium, lumen, and stromal composition on corresponding whole mount histopathology. Eur Radiol 2021; 31: 1336-46.
- Panda A, Obmann VC , Lo WC, et al. MR fingerprinting and ADC mapping for characterization of lesions in the transition zone of the prostate gland. Radiology 2019; 292: 685-94.
- Ueda Y, Tamada T, Obara M, et al. Synthetic DWI in prostate. Proceedings of the 29th Annual Meeting of ISMRM, 2021 #4087.
- Chatterjee A, Devaraj A, Mathew M, et al. Performance of T2 Maps in the Detection of Prostate Cancer. Acad Radiol 2019; 26: 15-21.
Figures
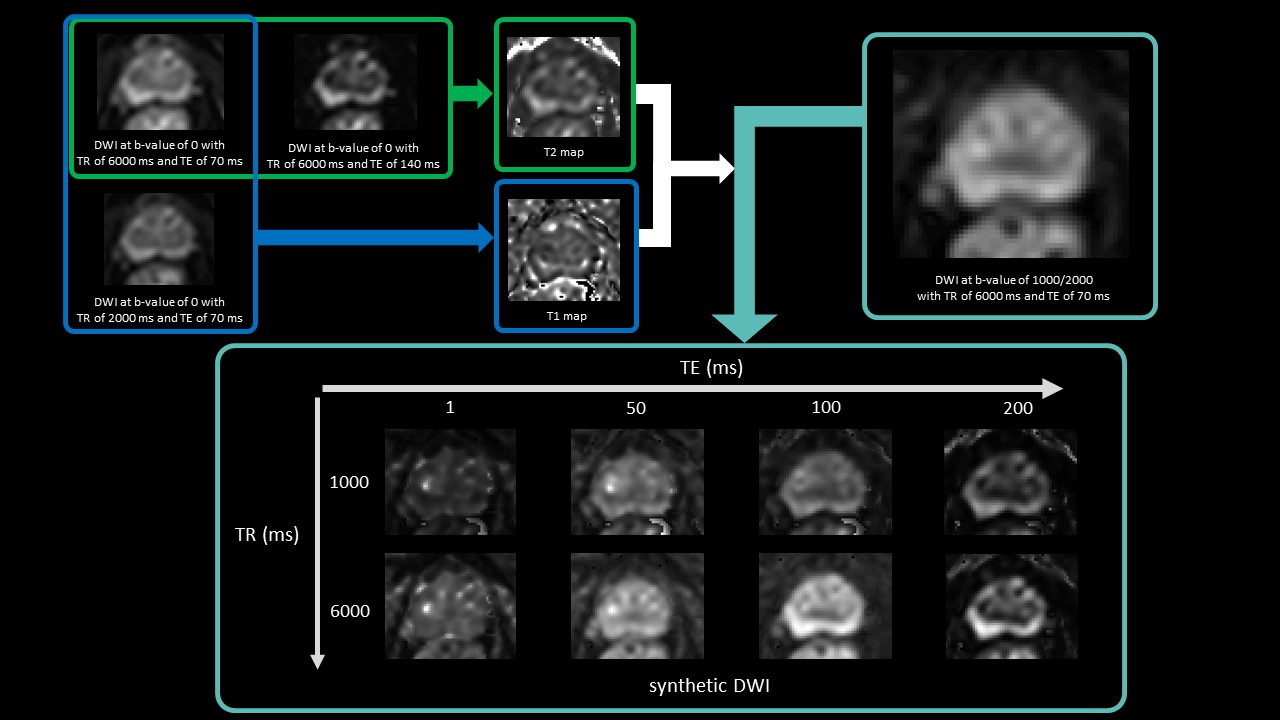
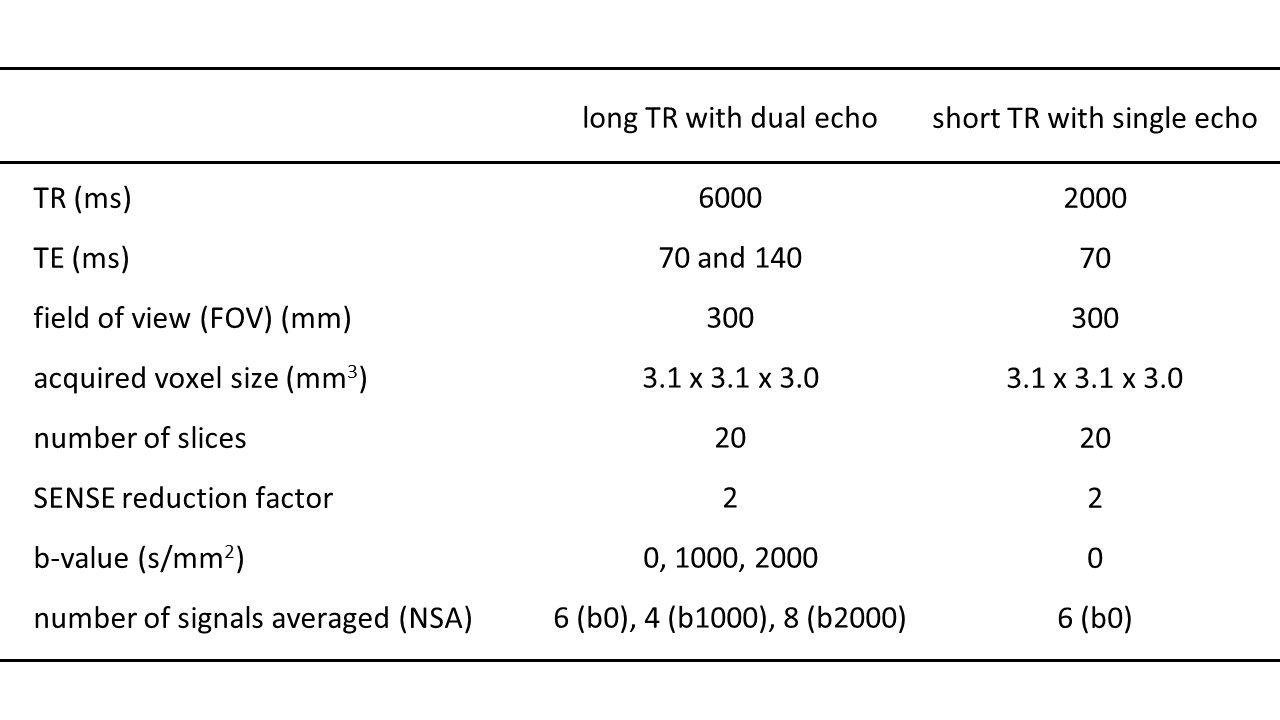
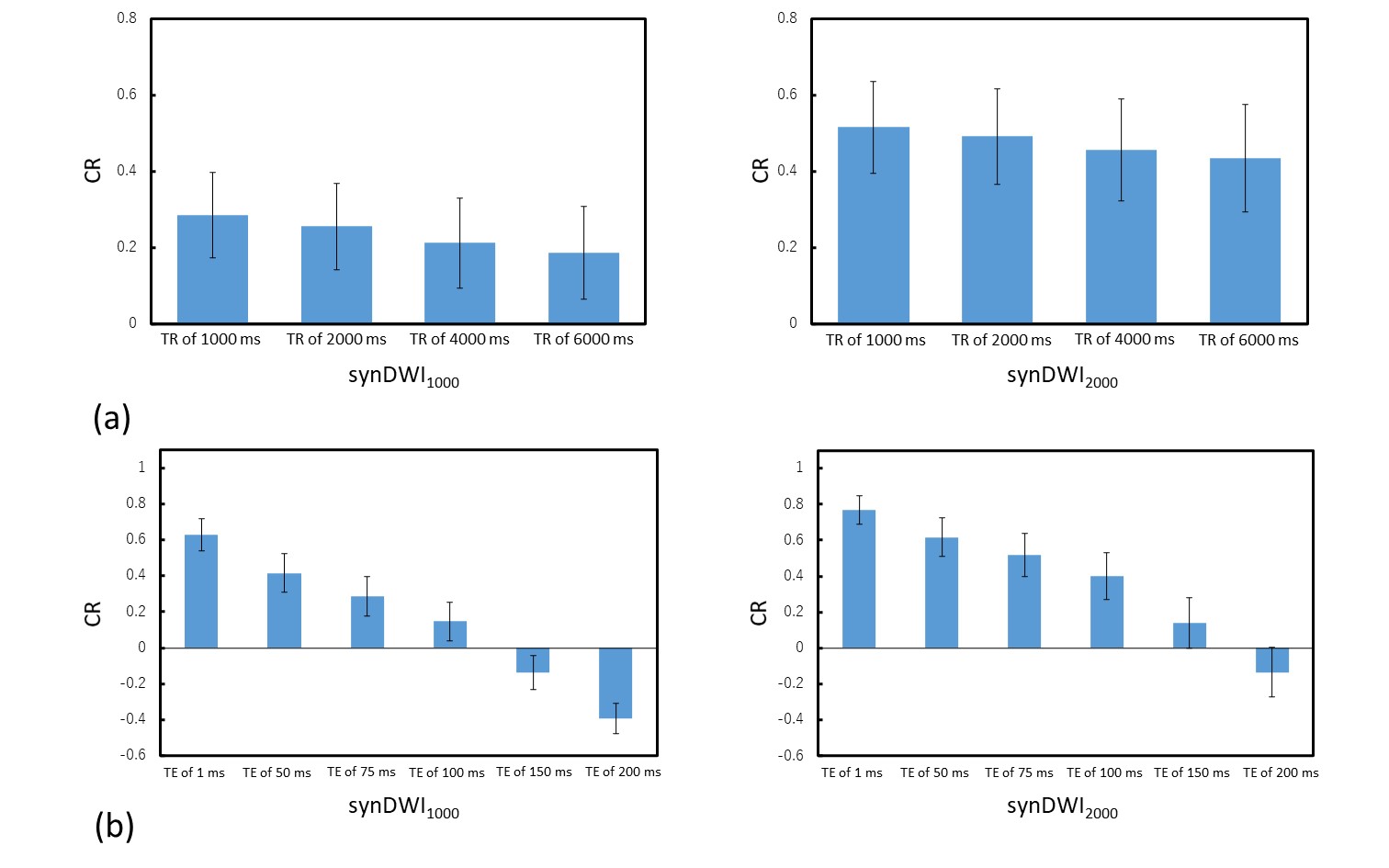
Figure 3. Comparison of contrast ratio (CR) among (a) synDWI at TE of 75 ms for both b-values with TR of 1000, 2000, 4000, and 6000 ms, and (b) synDWI at TR of 1000 ms for both b-values with TE of 1, 50, 75, 100, 150, and 200 ms. DWI at b-values of 1000 and 2000 s/mm2 are denoted as DWI1000 and DWI2000, respectively. Repeat measures ANOVA showed significant variation in CR of synDWI for TR (a) and TE (b) (P < 0.001 for both), and post-testing using Bonferroni multiple comparisons test showed significant difference in all pairs (P < 0.01 for comparison of TR [a] and P < 0.001 for comparison of TE [b]).