3664
Automatic segmentation of bladder cancer on MRI using a convolutional neural network and reproducibility of radiomics features.1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan, 2Department of Radiology, Japanese Red Cross Osaka Hospital, Osaka, Japan, 3Department of Urology, Kyoto University Graduate School of Medicine, Kyoto, Japan
Synopsis
This multi-center retrospective study performed automatic segmentation of bladder cancer (BC) on MRI with a convolutional neural network and evaluated the reproducibility of radiomics features. Of the total 170 patients, 140 were used to train our U-net model and 30 were used to evaluate the segmentation performance of the model. Our U-net model achieved a median Dice similarity coefficient of 0.811 in the test dataset and most of the automatically extracted radiomics features showed high reproducibility (median intraclass correlation coefficient: 0.83-0.86). Our model would lead to efficient medical image analysis of BC using the radiomics approach.
Introduction
MRI plays a very important role in deciding the treatment of bladder cancer (BC) 1. In recent years, medical image analysis using the radiomics approach has been attracting attention, and it has been reported that radiomics can be used to predict the staging of bladder cancer, including muscle layer invasion 2-5. For this type of research, tumor segmentation is necessary, but manual segmentation is labor-intensive and lacks objectivity. If highly accurate automatic tumor segmentation can be achieved, many regions of interest (ROI) can be created with less effort. Although there have been a few studies of automated segmentation of BC on MRI, these studies were conducted at a single institution with a small number of patients and lack the generalization performance required in actual clinical practice 6,7. To overcome this weakness, this study included a large number of BC patients at multiple institutions and MR images of multiple vendors. Our purpose was to perform the automatic segmentation of BC on MRI with high generalization performance. In addition, we examined the reproducibility of radiomics features extracted from manually and automatically segmented BC.Methods
This multi-center retrospective study included 170 patients with BCs who underwent bladder MRI between January 2016 and June 2020. MR examinations were performed using 3.0 T and 1.5 T MR units of multiple vendors (Siemens, Philips, and GE). All studies included DWIs with b-values of 0 and 1000 s/mm2 and apparent diffusion coefficient (ADC) maps. The 170 patients were randomly divided into two groups: 140 for training the modified U-net model and 30 for testing the segmentation performance of our U-net model. One board-certified radiologist manually segmented the BCs on each slice of the axial DWIs using a 3D slicer (https://www.slicer.org/) referring to other sequences and pathological information, and another board-certified radiologist confirmed the validity of the regions of interest (ROI) in all cases. These ROIs were regarded as the gold standard for segmentation.DWIs with b-values of 0 and 1000 s/mm2 and ADC maps were used as the 3-channel input data for our U-net model. As image preprocessing, the MR images were resized to 128 × 128 pixels, and signal intensity normalization was performed. We performed hyperparameter tuning of our U-net model for the segmentation of BCs with five-fold cross-validation using four-fifths of the patients for training and one-fifth for validation (Figure 1). The number of epochs, batch sizes, and initial learning rate were set to 30, 56, and 0.001, respectively. The Adam optimizer was used to train our U-net model with Dice loss as the cost function. Our model was built using TensorFlow (version 2.5.0) and trained on a Linux workstation (Ubuntu 18.04) with an NVIDIA GeForce RTX3090 GPU with 24 GB memory. For segmentation of BCs in the test datasets, we used an ensemble model of the five U-net models trained based on the training sets of cross-validation. The performance of the segmentation accuracy was evaluated with the Dice similarity coefficient (DSC).
After the segmentation of BC, radiomics features of BC were calculated using Pyradiomics software (version 3.0.1) from the volume-of-interest on ADC map with manual and automatic segmentation by our U-net model. The following radiomics features were calculated: first-order features (n=18), shape-based features (n=14), and features with gray-level co-occurrence matrix (GLCM) (n=24), gray-level run-length matrix (GLRLM) (n=16), gray-level size zone matrix (GLSZM) (n=16), neighboring gray-tone difference matrix (NGTDM) (n=5), and gray-level dependence matrix (GLDM) (n=14).
Statistical analyses were performed using a commercially available software package (JMP, version 15.2.0). Regarding the clinical characteristics of the training and test sets, age was compared using t-test, and gender, grade, and muscle invasion were compared using chi-square test. The reproducibility of radiomics features was evaluated using the intraclass correlation coefficient (ICC), which was calculated using pingouin package (version 0.3.8). ICC values were interpreted as follows: <0.5, poor; 0.5–0.75, moderate; 0.75–0.9, good; >0.9, excellent.
Results
The patients’ characteristics are presented in Table 1. There was no significant difference in age, gender, histological grade, or muscle invasion between training and test sets. The DSCs for the five training and validation sets were as follows: 0.836/0.778, 0.828/0.785, 0.813/0.798, 0.819/0.782, and 0.819/0.801, respectively. The median value [interquartile range] of the DSCs for the test set were 0.811 [0.699, 0.881]. Representative cases of automatic segmentation for test cases are presented in Figure 2. The median value and interquartile range of the ICC values of the radiomics features obtained by manual and automatic segmentation are presented in Table 2. All of the first-order and shape-based features except major axis length showed moderate-excellent reliability. Most of the higher-order features also showed moderate-excellent reliability.Discussion
We have achieved highly accurate automatic segmentation of BCs on multi-center and multi-vendor MRI using our modified U-net. The radiomics features obtained with our model showed high reliability for first-order, shape-based, and higher-order features. Our model would make it possible to prepare a large number of ROIs for BCs on MR images with less effort, which leads to efficient medical image analysis using the radiomics approach and/or deep learning methods for the staging and risk stratification of BCs.Acknowledgements
This research was supported by Bayer research grant of the Japanese Radiological Society.References
1. Panebianco V, Narumi Y, Altun E, et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System). Eur Urol 2018;74(3):294-306.
2. Wang H, Hu D, Yao H, et al. Radiomics analysis of multiparametric MRI for the preoperative evaluation of pathological grade in bladder cancer tumors. Eur Radiol 2019;29(11):6182-6190.
3. Wang H, Xu X, Zhang X, et al. Elaboration of a multisequence MRI-based radiomics signature for the preoperative prediction of the muscle-invasive status of bladder cancer: a double-center study. Eur Radiol 2020;30(9):4816-4827.
4. Zheng Z, Xu F, Gu Z, et al. Combining Multiparametric MRI Radiomics Signature With the Vesical Imaging-Reporting and Data System (VI-RADS) Score to Preoperatively Differentiate Muscle Invasion of Bladder Cancer. Front Oncol 2021;11:619893.
5. Zheng Z, Xu F, Gu Z, et al. Integrating multiparametric MRI radiomics features and the Vesical Imaging-Reporting and Data System (VI-RADS) for bladder cancer grading. Abdom Radiol (NY) 2021;46(9):4311-4323.
6. Bandyk MG, Gopireddy DR, Lall C, Balaji KC, Dolz J. MRI and CT bladder segmentation from classical to deep learning based approaches: Current limitations and lessons. Comput Biol Med 2021;134:104472.
7. Liu Y, Zheng H, Xu X, et al. The invasion depth measurement of bladder cancer using T2-weighted magnetic resonance imaging. Biomed Eng Online 2020;19(1):92.
Figures
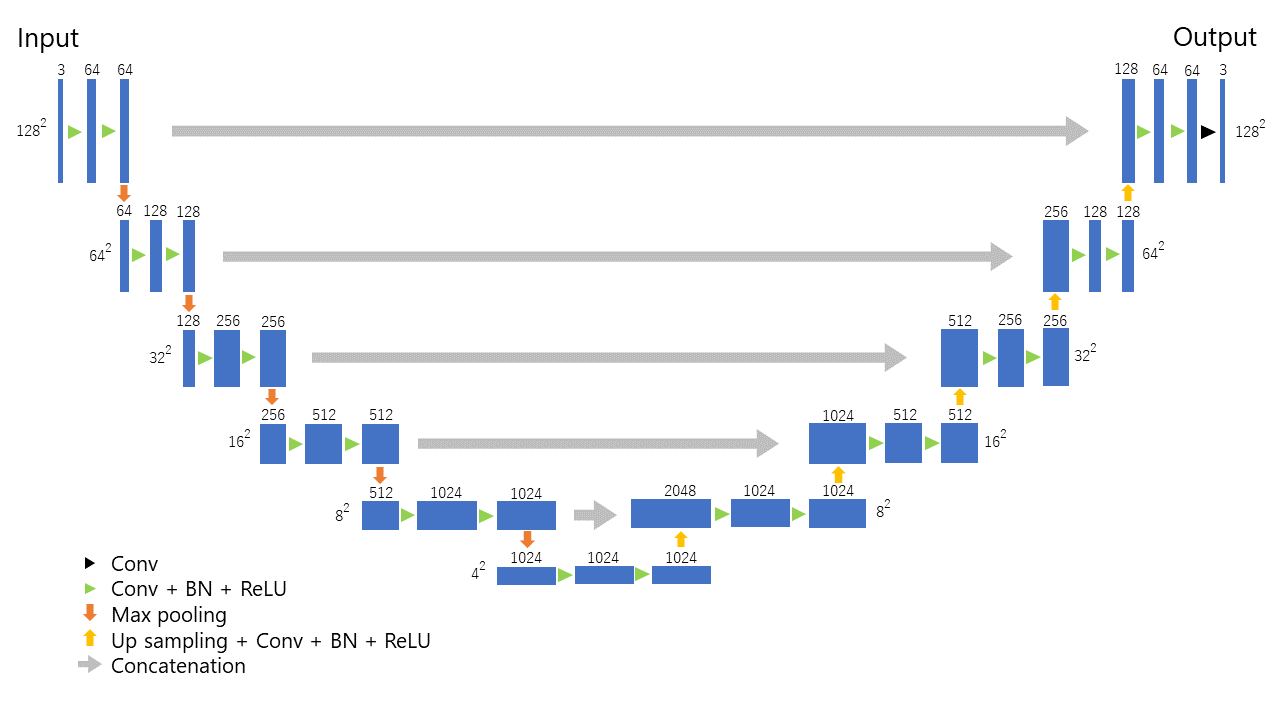
Figure 1. Our U-net architecture for the segmentation of bladder cancer.
Conv: convolution, BN: batch normalization, ReLU: Rectified Linear Unit.
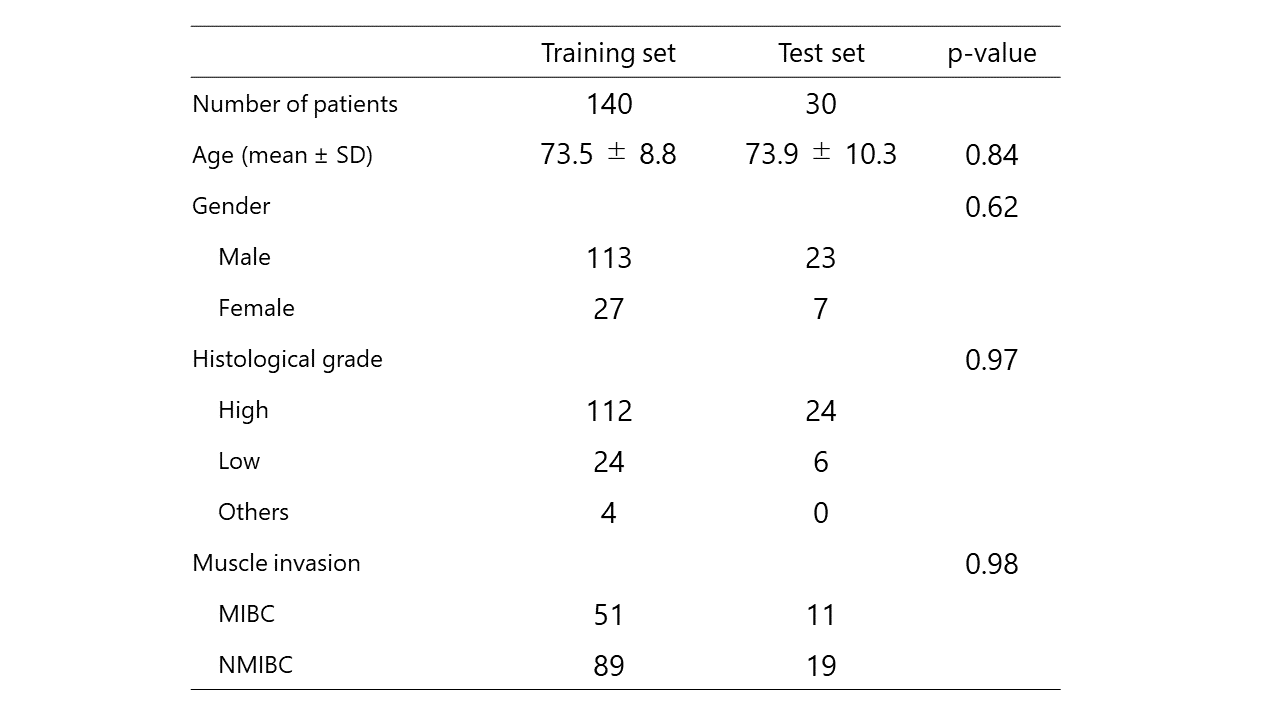
Table 1. Clinical characteristics of the training and test set.
SD: standard deviation, MIBC: muscle-invasive bladder cancer, NMIBC: non-muscle-invasive bladder cancer.
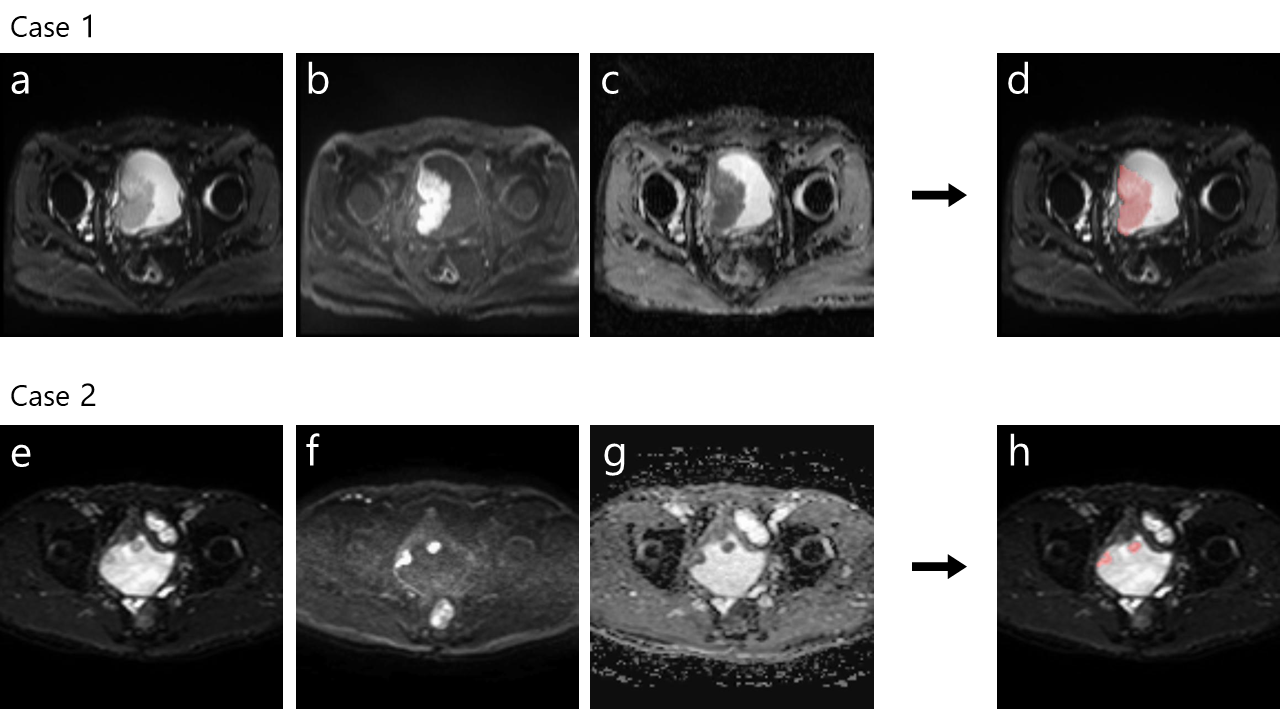
Figure 2. Two representative cases of automatic segmentation of bladder cancer (Case 1: a-d, Case 2: e-f). The DSCs for case 1 and case 2 were 0.946 and 0.819, respectively. Accurate segmentation was performed even for large and multiple lesions.
a, e: diffusion-weighted image (b=0 s/mm2)
b, f: diffusion-weighted image (b=1000 s/mm2)
c, g: apparent diffusion coefficient map
d, h: results of automatic segmentation of bladder cancer overlaied on diffusion-weighted image (b=0 s/mm2)
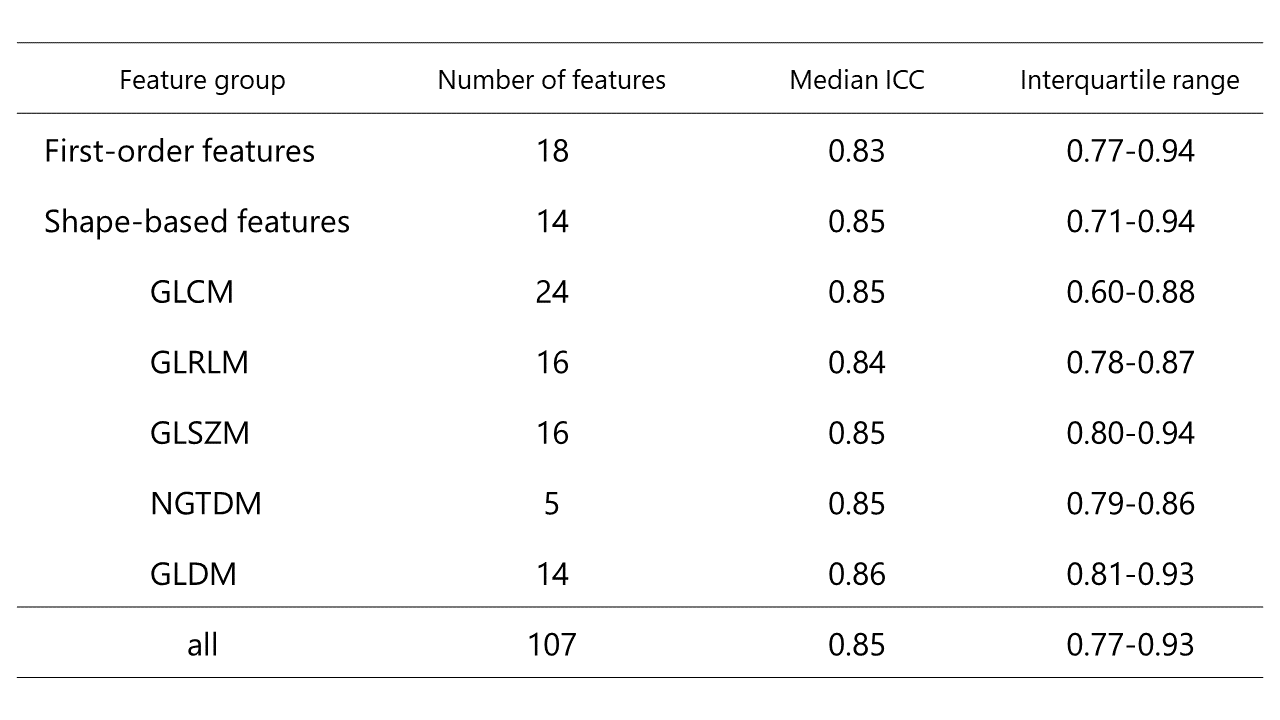
Table 2. The median and interquartile range for the intraclass correlation coefficient (ICC) values per feature group.
GLCM: gray-level co-occurrence matrix
GLRLM: gray-level run-length matrix
GLSZM: gray-level size zone matrix
NGTDM: neighboring gray-tone difference matrix
GLDM: gray-level dependence matrix