3632
The feasibility of contrast-enhanced 3D T1WI reconstructed with Compressed SENSE Artificial Intelligence in evaluation of brain metastases1Radiology, The First Hospital of Jilin Universty, Changchun, China, 2Ultrasound, The First Hospital of Jilin Universty, Changchun, China, 3Philips Healthcare, Beijing, China
Synopsis
Contrast-enhanced (CE) 3D T1-weighted scanning has been used more frequently with better spatial resolution and thinner section than 2D T1-weighted images for early detection and response assessment of brain metastases. To further improve the image scanning sequence, a new reconstruction algorithm, Compressed-SENSE Artificial Intelligence (CS-AI) was applied experimentally to achieve a balance between shortened scan time and improved image quality. This study aims to investigate the feasibility of contrast-enhanced 3D T1-weighted MRI reconstructed with Compressed SENSE Artificial Intelligence (CS-AI) by comparing with 3D T1-weighted images reconstructed with Compressed SENSE(CS), and to find out the optimal acceleration factor(AF).
Introduction
Brain metastases (BM) as secondary brain neoplasms are the most common type of brain tumors in adults1-2. Early detection of brain metastases has become an important determinant of both survival time and quality of life for cancer patients. Contrast-enhanced 3D T1-weighted scanning shows higher sensitivity than 2D T1-weighted enhanced scanning for the detection of small brain metastases and has been used more frequently for the evaluation of brain metastases3-4. However, the long acquisition time of 3D sequence limits its use in clinical settings. Compressed SENSE (CS) has been validated as an efficient acceleration technique which may reduce the acquisition time and artifact of pulsation. More recently, deep learning framework have been combined with CS to overcome these challenges by learning optimal reconstruction parameters from the data itself and showed superior performance5.Purpose
The purpose of this study was to acquire highly accelerated 3D T1-weighted imaging using the Compressed-SENSE Artificial Intelligence (CS-AI) framework reconstruction and to evaluate the image quality of CS-AI with different high acceleration factors (AF) compared with CS technique.Methods
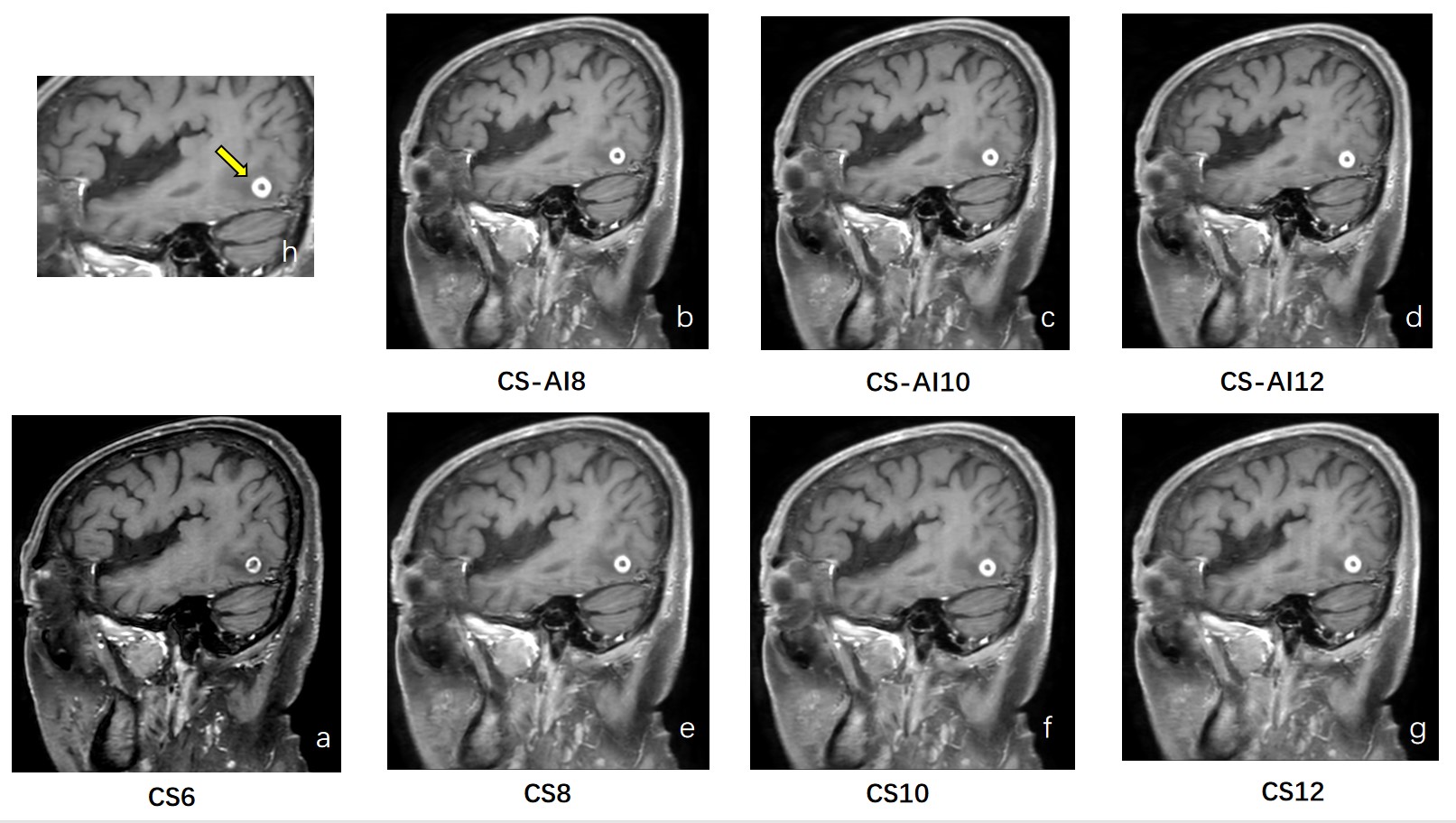
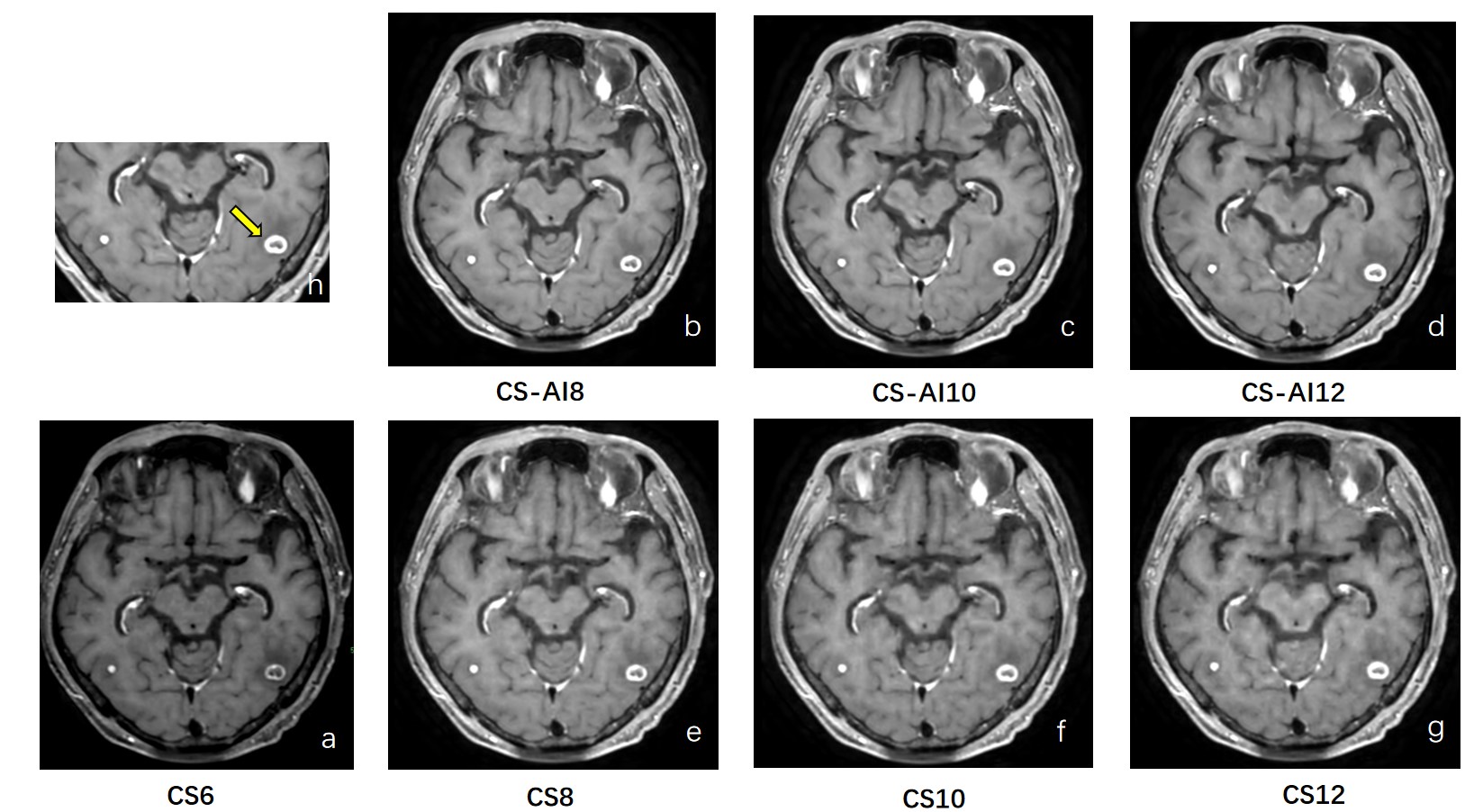
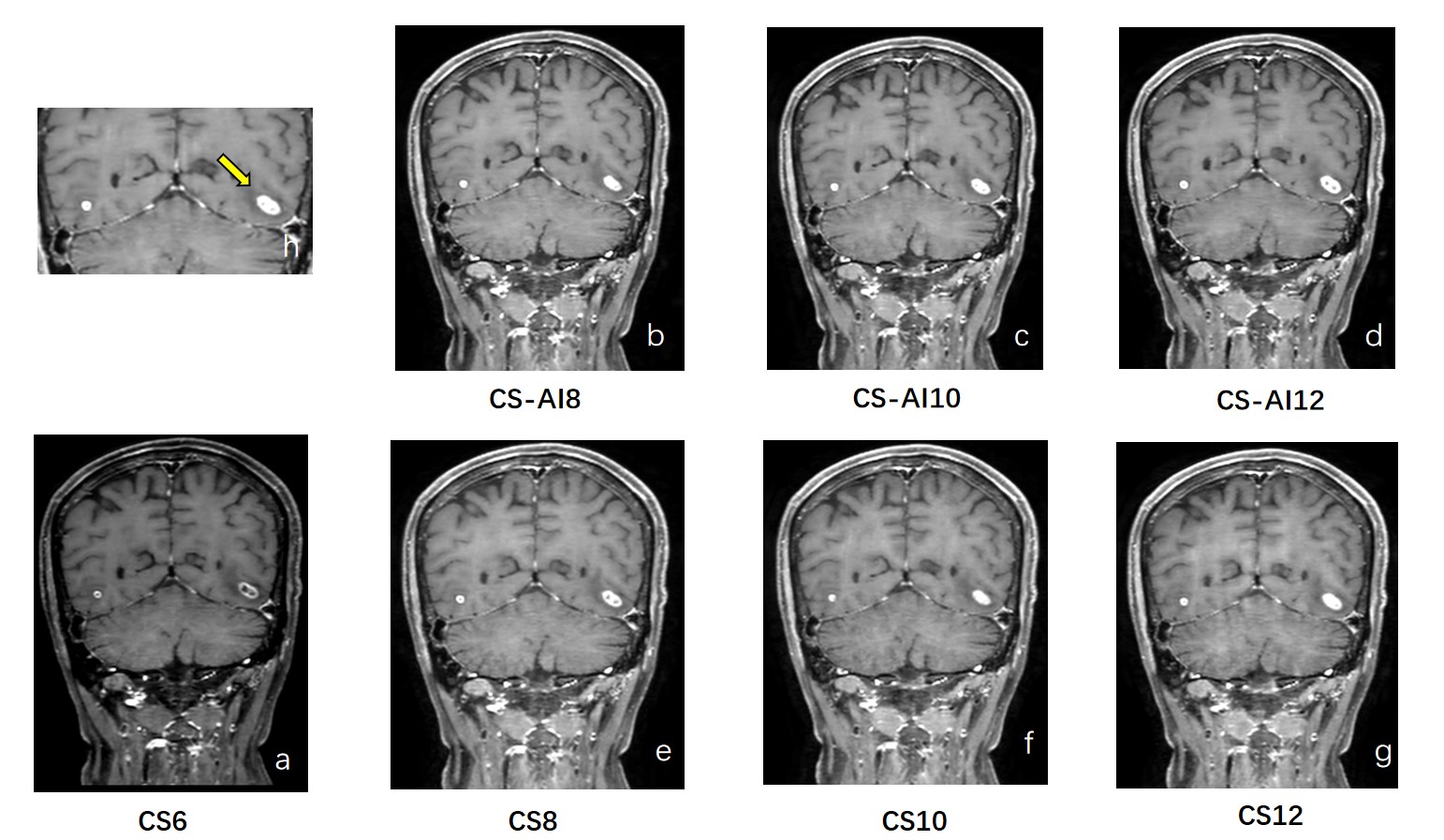
This study was approved by the institutional review board of the first hospital of Jilin University, and written informed consent was obtained from all subjects. A total of 14 patients who were suspected of metastatic lesions were examined on a 3.0T MR system (Ingenia Elition X, Philips Healthcare). All patients received different customized 3D T1-weighted sequences which included different AF sequences utilizing CS (CS6, CS8, CS10, CS12) and CS-AI technology (CS-AI8, CS-AI10, CS-AI12) in random order. Among them, CS6 is a commercially available standard sequence and is shown as a reference. The parameters for 3D T1-weighted were: TR=600ms; TE=28ms; FOV=250×250mm, 327 slices, voxel size=0.99×1.00×1.10mm. The total scanning time of post-contrast 3D TI-weighted reconstructed with CS6, CS/CS-AI-8, CS/CS-AI-10, CS/CS-AI12 were 3:34min, 2:42min, 2:10min and 1:49min, respectively. Quantitative image analysis was performed by two radiologists with more than 5 years of experience. (Figure1-3) ROIs were placed on lesions and white matters. Based on the ROIs, Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were analyzed for objective evaluation with the following formula:$$SNR_{lesion}=\frac{SI_{lesion}}{SD_{lesion}}$$ [1]
$$CNR_{lesion-white matter}=\frac{|SI_{lesion}-SI_{white matter}|}{\sqrt{SD_{lesion}^{2}+SD_{white matter}^{2}}}$$ [2]
One-way repeated-measures analysis of variance (ANOVA) and post hoc Tukey test were used for statistical analysis by Graphpad 9.0. Values of P < 0.05 were considered statistically significant.
Results and Discussion
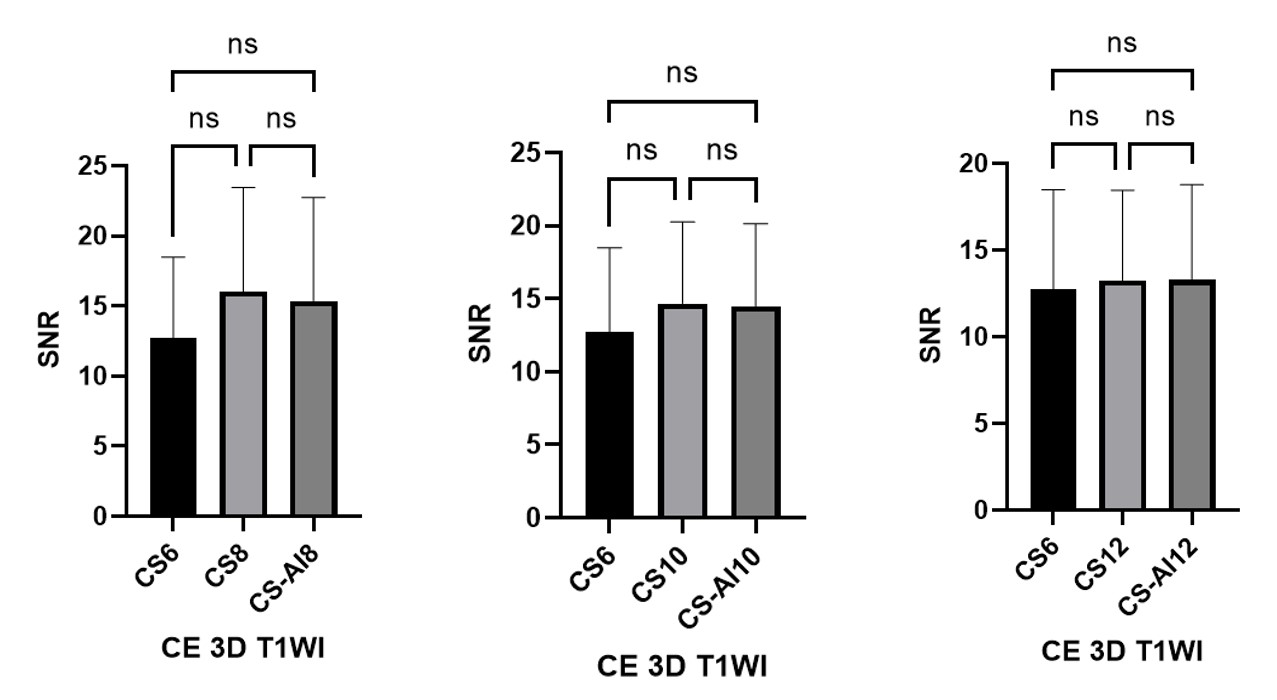
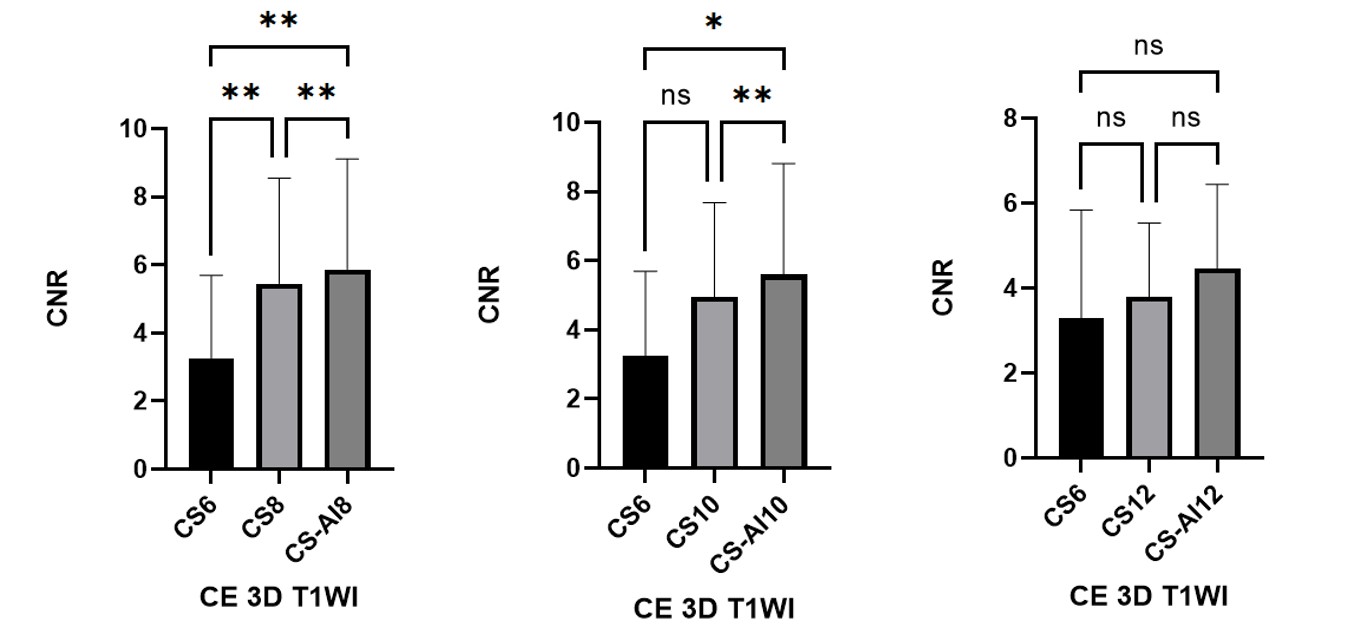
There was no significant difference of SNRs observed between CS-AI and CS for any AF(all P>0.05) (Figure4). The CNRs of CS-AI8 and CS-AI10 were significantly higher than those acquired with reference CS6 (P<0.05), and no significant difference was found in CNR between CS-AI12 and reference CS6 (P>0.05). Moreover, the CNR values of CS-AI8 and CS-AI10 were higher than that of CS scans at the same AF(Both P<0.05). Additionally, the image quality of CS-AI with AF 8 was similar to 10. It showed degradation of image quality with AF 12 due to insufficient noise removal, while the image quality with AF 8 and 10 showed better performance (Figure5). AF 8 has slight advantage in the presentation of lesion details, whereas AF 10 can save more time.Conclusion
3D T1-weighted sequence reconstructed with CA-AI at 3.0 T in detection of brain metastases may provide an effective, alternative reconstruction approach to CS. We suggest that acceleration factor 10 is more suitable for clinical application with the optimal image quality and shortened time.Acknowledgements
No acknowledgement found.References
1. Kaufmann TJ, Smits M, Boxerman J, et al. Consensus recommendations for a standardized brain tumor imaging protocol for clinical trials in brain metastases. Neuro Oncol. 2020;22(6):757-772. doi:10.1093/neuonc/noaa030
2. KakedaS,KorogiY,HiaiY,etal. Detection of brain metastasis at 3T: comparison among SE, IR-FSE and 3D-GRE sequences. Eur Radiol2007;17:2345–51 CrossRef Medline
3. Kim D, Heo YJ, Jeong HW, Baek JW, Han JY, Lee JY, Jin SC, Baek HJ. Usefulness of the Delay Alternating with Nutation for Tailored Excitation Pulse with T1-Weighted Sampling Perfection with Application-Optimized Contrasts Using Different Flip Angle Evolution in the Detection of Cerebral Metastases: Comparison with MPRAGE Imaging. AJNR Am J Neuroradiol. 2019 Sep;40(9):1469-1475. doi: 10.3174/ajnr.A6158. Epub 2019 Aug 1. PMID: 31371358; PMCID: PMC7048452.
4.Langer CJ, Mehta MP. Current management of brain metastases, with a focus on systemic options. J Clin Oncol 2005;23:6207–19CrossRef Medline
5.Knoll F, et al. Advancing machine learning for MR image reconstruction with an open competition: Overview of the 2019 fastMRI challenge. MagnReson Med. 2020;(January):mrm.28338.
Figures