3582
Compact 3T brain MRI for patients with abandoned leads of cardiac implantable electronic devices
Lydia J Bardwell Speltz1,2, Yunhong Shu1, Robert E Watson1, Joshua D Trzasko1, Erin Gray1, Maria Halverson1, Joseph Arant1, John Huston III1, Thomas KF Foo3, and Matt A Bernstein1
1Department of Radiology, Mayo Clinic, Rochester, MN, United States, 2Mayo Clinic Graduate School of Biomedical Sciences, Mayo Clinic, Rochester, MN, United States, 3GE Global Research, Niskayuna, NY, United States
1Department of Radiology, Mayo Clinic, Rochester, MN, United States, 2Mayo Clinic Graduate School of Biomedical Sciences, Mayo Clinic, Rochester, MN, United States, 3GE Global Research, Niskayuna, NY, United States
Synopsis
Patients with abandoned pacemaker leads require special attention during MR exams due to the risk of lead tip heating from RF energy deposition. The electromagnetic fields on the compact 3T (C3T) scanner fall off rapidly caudal to the head, and therefore present a reduced risk of lead tip heating during brain imaging. We compared the images from a whole-body 1.5T scanner and a high-performance C3T scanner. The C3T images show substantial improvements in image quality and greater cortical detail. This work establishes the feasibility of C3T brain MRI with a 32-channel receive coil for patients with abandoned leads.
Introduction
Many patients undergoing MRI exams have abandoned (i.e., retained) leads from cardiac implantable electronic devices (CIED) such as pacemakers. A 10-year study performed at our institution showed that 8.4% of CIED patients who received a MR exam had retained leads in place.1 CIEDs are common with around 1.2-1.4 million implanted annually.2 Retained leads have a greater risk of lead tip heating compared to leads that are attached to a generator3 and therefore require special attention during a MR exam. Unlike many modern CIEDs, there are currently no abandoned leads labeled MR conditional. Guidance from the Heart Rhythm Society4 is to generally avoid MR exams when abandoned leads are present. However, the clinical practice at our institution routinely performs these exams in properly triaged patients at 1.5T under the supervision of a medical physicist and advanced cardiovascular life support (ACLS)-certified nurse, after obtaining informed consent. The primary patient safety concern with abandoned leads is RF-related lead tip heating.4-5 While MRI studies of patients with abandoned leads have been reported3, these have all been performed at 1.5T, to our knowledge.The compact 3T (C3T) scanner was developed under NIH funding as a technology demonstrator.6 Its smaller size enables high-performance gradients: simultaneous slew rate of 700T/m/s and gradient amplitude of 80mT/m with a higher peripheral nerve stimulation threshold than whole-body gradients.7-8 The gradient coil has an inner diameter of 42cm, allowing for exams of the head, extremities, and infants. A major advantage of the C3T for patients with implanted devices is the electromagnetic fields drop off much more rapidly caudal to the head due to the smaller scanner size. Therefore, abandoned CIED leads are subjected to less RF energy which reduces the risk of lead tip heating. In this work, we performed a safety assessment for scanning a subject with abandoned leads, and then compared the whole-body 1.5T and C3T image quality.
Methods
Under an IRB-approved protocol, an 82-year-old male subject with abandoned leads was identified from the clinical MRI schedule. A board-certified medical physicist performed a safety assessment for C3T brain scanning based on the subject’s medical record, including a chest x-ray (Figure 1). Our previously-reported safety assessment tool9 was used to determine the magnitude of the relevant electromagnetic fields at the location of the abandoned leads. The particular focus of this assessment is the rapid falloff of the amplitudes of the B19 and electric fields10 caudal to the head. Notably, the B1 amplitude was reduced by approximately 80% at the location of the abandoned leads compared to its value at the brain (Figure 2). Similar reduction in the amplitude of electric field E is expected from the simulations based on several digital human body models (HBM).10 The safety assessment tool also provides the main magnetic field (B0), spatial field gradient, and gradient strength information. The result of the MR safety assessment was a brain exam of this subject could be safely performed on the C3T scanner, and he was subsequently enrolled in the study after providing written informed consent.The subject had abandoned leads (A96527, St. Jude, TN) and received a series of five 1.5T imaging exams for tumor assessment and follow-up exams from 10-Aug-2016 through 2-Nov-2021. Immediately following the clinical gadolinium-enhanced 1.5T brain exam on 2-Nov-2021, the C3T exam was performed. The C3T imaging protocol matched the clinical exam while ensuring at least equivalent image quality compared to 1.5T. As with the 1.5T clinical exam, the C3T research exam was supervised by a MR physicist and the subject monitored by an ACLS certified nurse.
Results
Figure 3 shows the comparison of the axial T2 FSE images performed on the whole-body 1.5T scanner and the C3T scanner. Imaging parameters at 1.5T include: TR: 4634ms, TE: 98ms, ETL: 8, NEX: 2, 256x256, and scan time: 5:38, using an 8-channel brain coil (Invivo, Orlando FL). Imaging parameters for the C3T were: TR: 5304ms, TE: 97ms, ETL: 12, NEX: 2, 320x320, and scan time: 2:34 using a 32-channel receive coil (Nova Medical, Wilmington, MA). Note the acquisition time was 54% less for the C3T exam. Figure 4 shows the comparison of the sagittal post-gadolinium cube T1 images performed on the whole-body 1.5T scanner and the C3T scanner. Imaging parameters for the 1.5T were: TR: 552ms, TE: 12ms, ETL: 22, NEX: 1, 256x256, and scan time: 5:30. Imaging parameters for the C3T were: TR: 602ms, TE: 11ms, ETL: 24, NEX: 0.5, 256x256, and scan time: 4:08.Discussion and Conclusion
3T imaging has become the clinical standard for brain imaging, but it is unavailable for many patients with implanted devices due to MR safety concerns. While whole-body 3T imaging with the use of a transmit/receive (T/R) coil is feasible from a MR safety perspective, this option incurs a large signal-to-noise penalty and precludes parallel imaging. This study demonstrates how subjects with abandoned CIED leads can be safely scanned at 3T with a compact scanner, using a 32-channel brain coil. Compared to the whole-body 1.5T scanner images, substantial reduction in acquisition time was achieved with the C3T, as well as improvements in image quality including better distinction of the gray/white matter interface and cortical detail.Acknowledgements
This work was supported by research grant: NIH R01EB010065 and U01 EB024450.References
- Padmanabhan D, Kella DK, Mehta R, Kapa S, Deshmukh A, Mulpuru S, Jaffe AS, Felmlee JP, Jondal ML, Dalzell CM, Asirvatham SJ, Cha YM, Watson RE Jr, Friedman PA. Safety of magnetic resonance imaging in patients with legacy pacemakers and defibrillators and abandoned leads. Heart Rhythm. 2018 Feb;15(2):228- 233. doi: 10.1016/j.hrthm.2017.10.022. Epub 2017 Oct 16. PMID: 29045806.
- Perez AA, Woo FW, Tsang DC, Carrillo RG. Transvenous Lead Extractions: Current Approaches and Future Trends. Arrhythm Electrophysiol Rev. 2018 Aug;7(3):210-217. doi: 10.15420/aer.2018.33.2. PMID: 30416735; PMCID: PMC6141917.
- Schaller RD, Brunker T, Riley MP, Marchlinski FE, Nazarian S, Litt H. Magnetic Resonance Imaging in Patients With Cardiac Implantable Electronic Devices With Abandoned Leads. JAMA Cardiol. 2021 May 1;6(5):549-556. doi: 10.1001/jamacardio.2020.7572. PMID: 33595595; PMCID: PMC7890450.
- Indik JH, Gimbel JR, Abe H, Alkmim-Teixeira R, Birgersdotter-Green U, Clarke GD, Dickfeld TL, Froelich JW, Grant J, Hayes DL, Heidbuchel H, Idriss SF, Kanal E, Lampert R, Machado CE, Mandrola JM, Nazarian S, Patton KK, Rozner MA, Russo RJ, Shen WK, Shinbane JS, Teo WS, Uribe W, Verma A, Wilkoff BL, Woodard PK. 2017 HRS expert consensus statement on magnetic resonance imaging and radiation exposure in patients with cardiovascular implantable electronic devices. Heart Rhythm. 2017 Jul;14(7):e97-e153. doi: 10.1016/j.hrthm.2017.04.025. Epub 2017 May 11. PMID: 28502708.
- Yang E, Suzuki M, Nazarian S, Halperin H. Magnetic Resonance Imaging Safety in Patients with Cardiac Implantable Electronic Devices. Trends Cardiovasc Med. 2021 Aug 9:S1050-1738(21)00085-2. doi: 10.1016/j.tcm.2021.08.001. Epub ahead of print. PMID: 34384880.
- Foo TKF, Laskaris E, Vermilyea M, Xu M, Thompson P, Conte G, Van Epps C, Immer C, Lee SK, Tan ET, Graziani D, Mathieu JB, Hardy CJ, Schenck JF, Fiveland E, Stautner W, Ricci J, Piel J, Park K, Hua Y, Bai Y, Kagan A, Stanley D, Weavers PT, Gray E, Shu Y, Frick MA, Campeau N, Trzasko J, Huston J, Bernstein MA. Lightweight, compact, and high performance 3T MR system for imaging the brain and extremities, Magn Reson Med 2018 80, 2232-2245.
- In MH, Shu Y, Trzasko JD, Yarach U, Kang D, Gray EM, Huston J, Bernstein MA. Reducing PNS with minimal performance penalties via simple pulse sequence modifications on a high-performance compact 3T scanner. Phys Med Biol. 2020 Jul 31;65(15):15NT02. doi: 10.1088/1361-6560/ab99e2. PMID: 32503007; PMCID: PMC7571537.
- Lee SK, Mathieu JB, Graziani D, Piel J, Budesheim E, Fiveland E, Hardy CJ, Tan ET, Amm B, Foo TK, Bernstein MA, Huston J 3rd, Shu Y, Schenck JF. Peripheral nerve stimulation characteristics of an asymmetric head-only gradient coil compatible with a high-channel-count receiver array. Magn Reson Med. 2016 Dec;76(6):1939-1950. doi: 10.1002/mrm.26044. Epub 2015 Dec 2. PMID: 26628078; PMCID: PMC4889567.
- Bardwell Speltz L, Shu, Y In MH, M N, Gray E, Lanners D, Hua Y, Watson R, Huston III J, Foo T, Bernstein M. Compact 3T MRI for patients with implanted devices: Software tool to display MR fields at a specified location. Proceedings of the Virtual Meeting of the International Society for Magnetic Resonance in Medicine 2021; 2298.9.
- Tarasek MR, Shu Y, Kang D, Tao S, Gray E, Huston J 3rd, Hua Y, Yeo DTB, Bernstein MA, Foo TK. Average SAR prediction, validation, and evaluation for a compact MR scanner head-sized RF coil. Magn Reson Imaging. 2021 Oct 16;85:168-176. doi: 10.1016/j.mri.2021.10.011. Epub ahead of print. PMID: 34666159.
Figures

Figure 1: Anterior-Posterior view chest x-ray, indicating the
location of the abandoned leads for the subject.
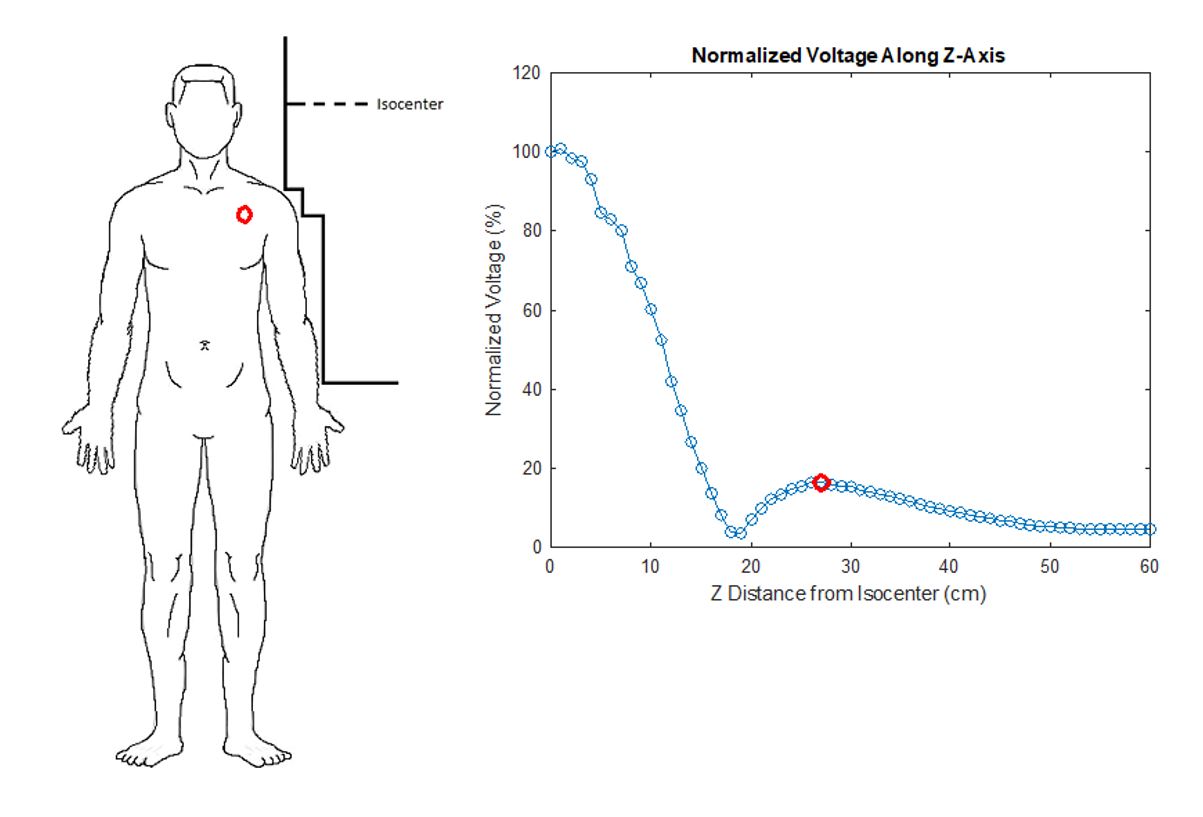
Figure 2: Subject with the location of abandoned leads indicated
by a red circle (left) and the RF plot (right) indicating the reduction of B1+
amplitude by approximately 80% at the superior location of the leads.
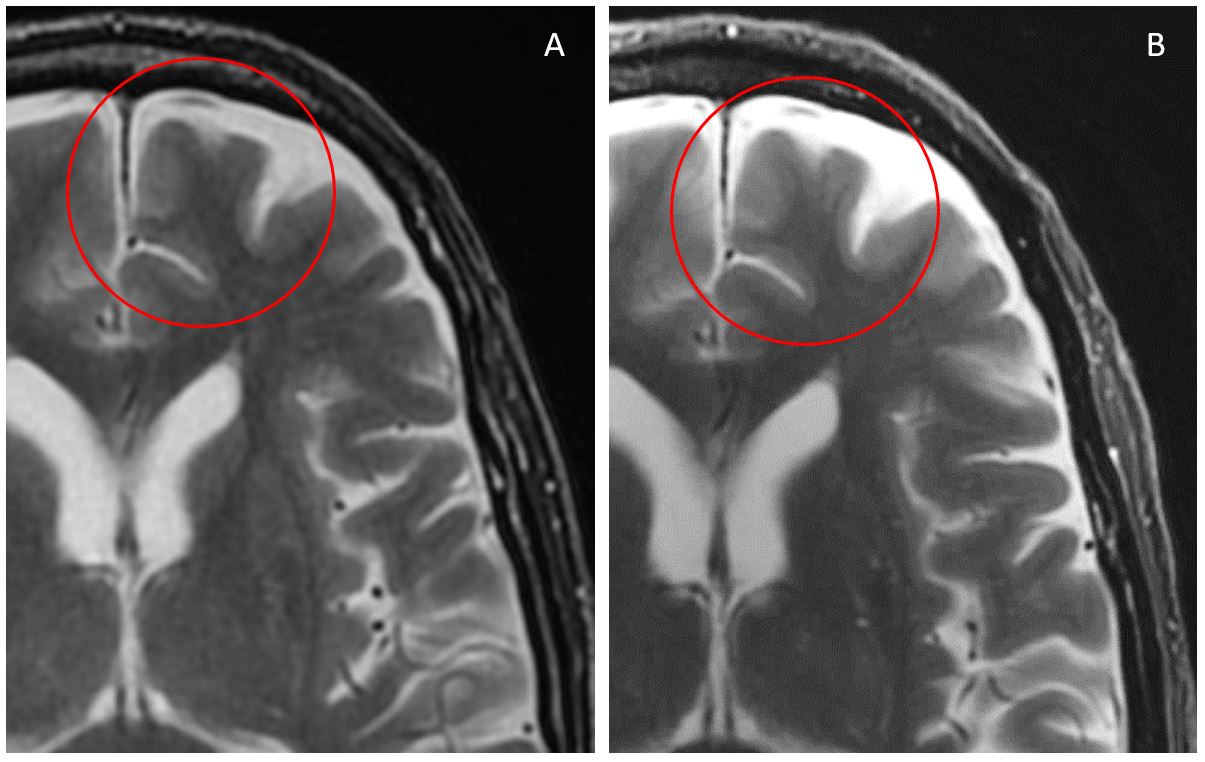
Figure 3: Axial T2 FSE performed on the whole-body 1.5T (A) and
C3T (B) scanner. Note the improved
distinctness of the gray / white interface and cortical detail (ovals) on the C3T
image vs. that on the 1.5T image.
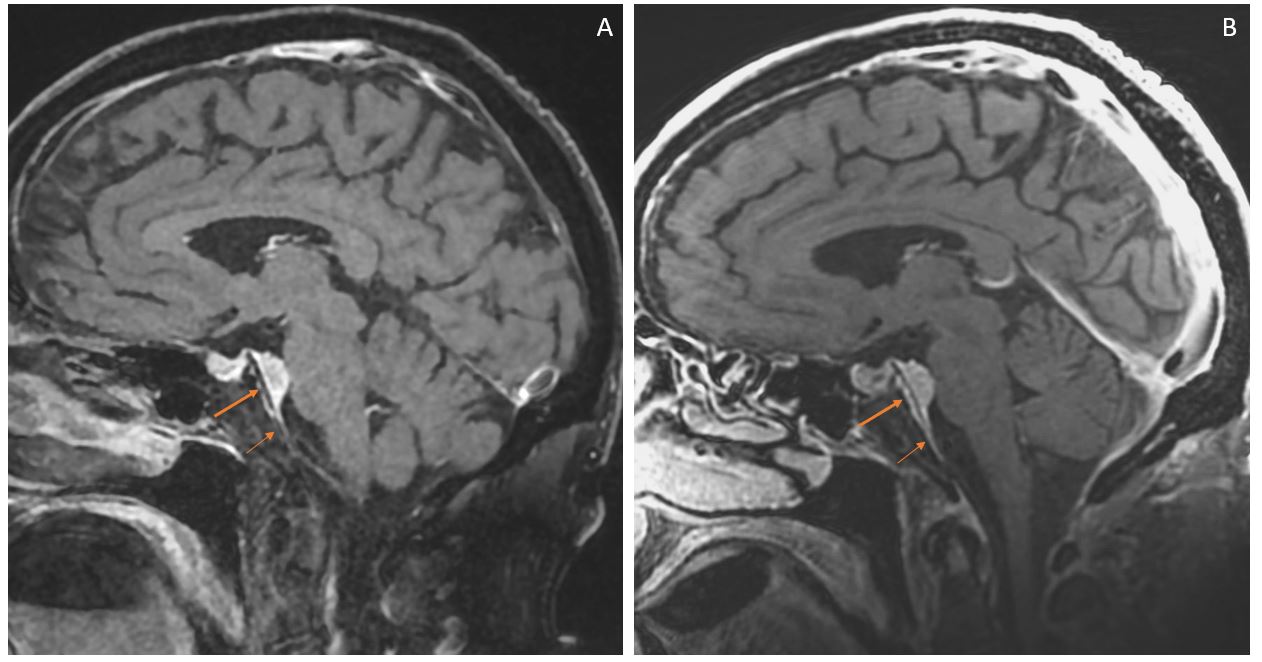
Figure 4: Sagittal post-gadolinium Cube T1 performed on a whole-body
1.5T (A) and C3T (B) scanner. An
enhancing meningioma (arrows) along the clivus contacts the pons. Note the
improved signal and increased distinctness of the associated dural tail
extending inferior to the main mass (small arrows) on the C3T image. There is
some expected signal dropout at the imaged upper cervical spine with C3T image
(B) vs 1.5T (A) due to coil configurations.
DOI: https://doi.org/10.58530/2022/3582