3561
Imaging Gas Exchange Using Hyperpolarized 129Xe as a Better Predictor of Endobronchial Valve Outcome
Hooman Hamedani1, Faraz Amzajerdian1, Stephen Kadlecek1, Ryan Baron1, Kai Ruppert1, Ian Duncan1, Mostafa Ismail1, Yi Xin1, Tahmina Achekzai1, Luis Loza1, and Rahim Rizi1
1University of Pennsylvania, Philadelphia, PA, United States
1University of Pennsylvania, Philadelphia, PA, United States
Synopsis
Bronchoscopic lung volume reduction (LVR) using endobronchial valves has proven effective at improving lung function and quality of life in certain severely emphysematous patients. Successful lung volume reduction of the target lobe shifts ventilation and perfusion to the healthier ipsilateral lobe and improves breathing mechanics. Functional imaging with spatially-resolved metrics using inhaled hyperpolarized 129Xe (HXe) may provide a deeper understanding of the physiology underlying clinical benefit.
Introduction
If successful, endobronchial valve treatment (Zephyr EBV, Pulmonx Corporation) causes full lobar atelectasis, shifting volume, ventilation and perfusion to healthier lung regions—thus reducing hyperinflation and improving breathing mechanics. Yet a significant number of patients for whom valve placement appears successful—e.g., improving objective clinical measures of flow and residual volume (FEV1 and RV)—do not report subjective dyspnea and quality of life gains. We hypothesize that this discrepancy can be primarily attributed to: 1) failure to effectively redistribute ventilation to the healthier lung, 2) failure to redistribute perfusion to take advantage of successfully achieved ventilation shifts, 3) worse than expected gas exchange properties of the non-targeted tissue. Here, we show the superior diagnostic power of multiparametric measurements of both ventilation and gas exchange using multibreath Hyperpolarized (HP) Xenon Transfer Contrast (XTC) MRI [1].Methods
Imaging was performed in a 1.5T Siemens scanner using an 8-channel 129Xe coil, with approval from Institutional Review Board. We previously introduced a multi-breath imaging scheme in which subjects inhale/exhale freely while HP gas is injected into a breathing line. Subjects breathe through a mouthpiece, while a constant ~50 mL of HP-Xe or air is injected into the line right before inhalation. 6 ad libitum normoxic wash-in breaths of hyperpolarized gas are followed by 4 washout breaths of room air; this ten-breath wash-in/washout series is repeated five more times with additional series encoding gas dissolution and uptake using the Xenon polarization Transfer Contrast (XTC). HXe images were then co-registered with an affine transformation and added together to produce a lung atlas. The lobar estimation was derived using a 2D deformable b-spline registration framework; for HXe, anatomical 1H MRI to CT-MR registration is used first; lobar EE CT segmentation is then applied to all warped images to yield lobar totals of regional minute and residual volumes (TV, FRC). We define the gas exchange rate in terms of the rate at which inverted spins re-enter the gas phase during the time (XTC), TR, between saturation pulses:$$X = (1 - f_{RBC}^{1/N})* FRC/TR$$
Results and Discussion
5 subjects were imaged in a 1.5T Siemens scanner using an 8-channel 129Xe coil, 3 of whom underwent both pre- and post-EBV imaging. Figure 1 shows functional maps (regional TV and X) pre- and post-intervention. A 67-year-old man with severe emphysema due to alpha-1 antitrypsin deficiency and progressive dyspnea, a 58-year-old female former smoker with progressively worsening symptoms due to COVID complications, and a 62-year-old COPD patient on triple therapy with severe cough (a candidate for lung transplantation), underwent endobronchial lung volume reduction. Both of our imaging markers are improved in the ipsilateral lobe in two subjects, with improvements in breathing mechanics as well as slightly improved overall lung function. FEV1 improved in these two subjects by 14% and 29%, respectively, while their St. George questionnaire scores (SGRQ) dropped 20% on average. Both imaging and clinical markers correlate with reported subjective improvements in these subjects, showing effectively redistributed ventilation and gas exchange to the healthier lung.In the third subject, on the other hand, although FEV1 improved from 0.59 to 0.77L, forced vital capacity (FVC) increased from 1.86 to 2.13L, and residual volume decreased from 5.6 to 4.2L, subjective SGRQ remained essentially the same (57 to 54%). What is more, although improvement was observed in their pulmonary function test (PFT) metrics, neither ventilation nor gas exchange changed substantially in the ipsilateral lobe (upper left lobe), likely due to the non-targeted lung’s severe centribular emphysema. The subject had a resting SpO2 between 92-95% during their first visit, but SpO2 stayed below 92% during their second visit. Additionally, their percent predicted DLCO (Diffusing Capacity of the Lungs for Carbon Monoxide) was 25.9% at their post-EBV imaging visit (DLCO measurement was not perform pre-procedure due to COVID restrictions).
Conclusion
Simultaneously imaging ventilation and gas exchange in the same lobe pre- and post-EBV placement may produce a more comprehensive picture of the lung’s response to this intervention, potentially helping to develop new strategies to expand the population of eligible candidates.Acknowledgements
No acknowledgement found.References
[1] Amzajerdian, Faraz, et al (2020). Measuring pulmonary gas exchange using compartment‐selective xenon‐polarization transfer contrast (XTC) MRI. MRM 85(5), 2709-2722.Figures
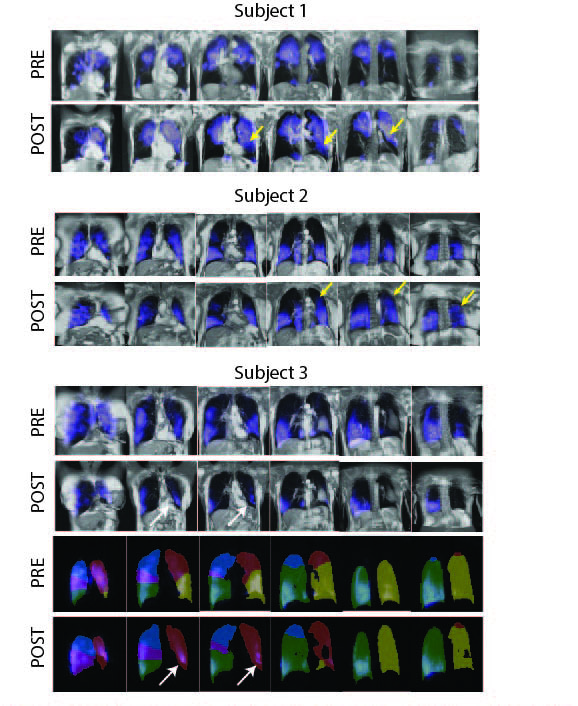
Figure 1. Pre- and post-EBV gas exchange maps in three subjects. The first two subjects represent new regions of both ventilation and gas exchange in non-targeted lobes (yellow arrows). In third subject, the occlusion of left lower lobe did not result in increased ventilation and gas exchange of the already severely emphysematous lobe (white arrow).
DOI: https://doi.org/10.58530/2022/3561