3502
Compressed sensing for motion-robust real-time fetal cardiac imaging1Radiology, Phoenix Children's Hospital, Phoenix, AZ, United States, 2Philips, Best, Netherlands, 3University of Arizona, Phoenix, AZ, United States
Synopsis
We examined undersampled real-time bSSFP reconstructions for fetal cardiac imaging. Two compressed sensing reconstructions, ICTGV and L plus S, were compared to k-t SENSE with respect to spatial and temporal blurring with and without fetal motion. Results with a digital fetal cardiac MRI phantom demonstrated ICTGV was able to capture expansion and contraction of the fetal heart even during periods of fetal motion while k-t SENSE and L plus S were not. Digital phantom results were confirmed on a 1.5T MRI scanner with implementation of ICTGV and acquisitions demonstrating pulsation of the fetal heart during periods of fetal motion.
INTRODUCTION
Random fetal motion, large maternal anatomy, and small fetal cardiac anatomy place high demands on spatial and temporal resolution of fetal imaging. Highly undersampled 2D Cartesian real-time imaging with balanced steady-state free precession (bSSFP) sequences has been used to capture the dynamics of the fetal heart1,2. Further, slice-to-volume (SVR) super-resolution reconstruction has been shown to effectively correct for motion between frames of a real-time sequence or between acquisitions2,3. However, SVR may not recover individual image frames if they are corrupted by artifact. In this work we examined robustness to image artifacts from fetal motion for three highly undersampled real-time Cartesian reconstruction schemes: k-t SENSE4, L plus S5, and ICTGV6. k-t SENSE relies on a regular undersampling pattern4, while L plus S and ICTGV utilized a quasi-random undersampling pattern7. Simulation of fetal motion and image acquisition was performed with a digital fetal cardiac MR (CMR) phantom for image quality comparison8. Simulation results were confirmed by implementing compressed sensing reconstructions on a 1.5T Philips scanner and imaging a normal fetal heart for a volunteer patient.METHODS
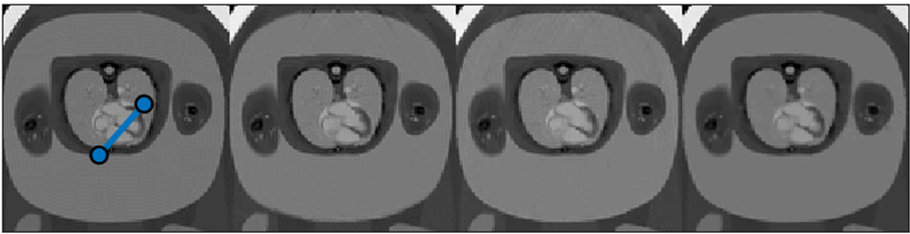
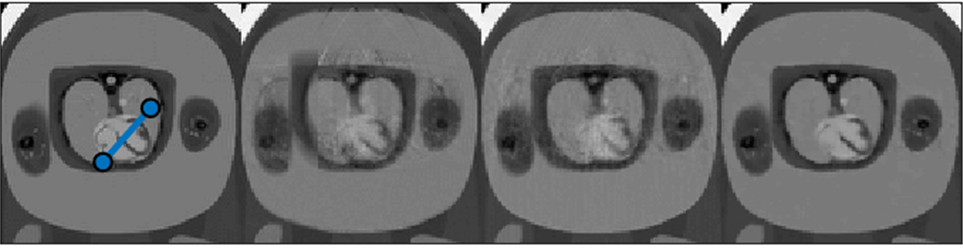
Two-dimensional bSSFP realt-time image formation in transverse, sagittal, and coronal orientation with a 24-element set of coils was simulated under two different motion conditions: 1) A stationary fetus. 2) Fetal motion due to random movements plus displacement from maternal breathing. A fetal heart rate of 140 beats per minute was simulated for both motion conditions. Spatial resolution ranged from 1.88 to 2.17 mm in-plane with a 6.0 mm slice thickness. Two-dimensional k-space was sampled according to an eight-fold regular undersampling pattern for k-t SENSE and separate training and high-resolution acquisitions were simulated. Twenty lines of k-space per image frame were simulated for the acquisition stage and an additional 10 lines of center k-space were acquired for the training stage. Simulated k-space was also sampled according to a VISTA pseudo-random eight-fold undersampling pattern and images were reconstructed with two compressed sensing algorithms: L + S or ICTGV. Twenty lines of k-space per image frame were acquired for compressed sensing algorithms. No training data was necessary for compressed sensing reconstruction . A TR of 3.5 ms was modeled for all acquisitions. Simulation parameters resulted in a temporal resolution of 70 ms per frame and a total acquisition time of 4.9 seconds for compressed sensing acquisitions and 7.4 seconds for k-t SENSE. Simulation reconstruction quality was assessed by measuring the average structural similarity index measure (SSIM) between ground truth images and reconstructions, considering a 3.2 cm square ROI containing the fetal heart. Additionally, VISTA dynamic scans were implemented on a Philips 1.5T scanner and reconstructed with ICTGV. 2D bSSFP real-time imaging was performed for a 32-week gestational age fetus with a normal heart. Acquistion parameters were as follows: TR=3.6 ms, 8-fold undersampling, 65 ms temporal resolution, 6 mm slice thickness, 4 mm slice spacing, and a scan duration of 4.2 seconds per slice. Image quality was assessed for its ability to capture the expansion and contraction of the chambers of the fetal heart.RESULTS
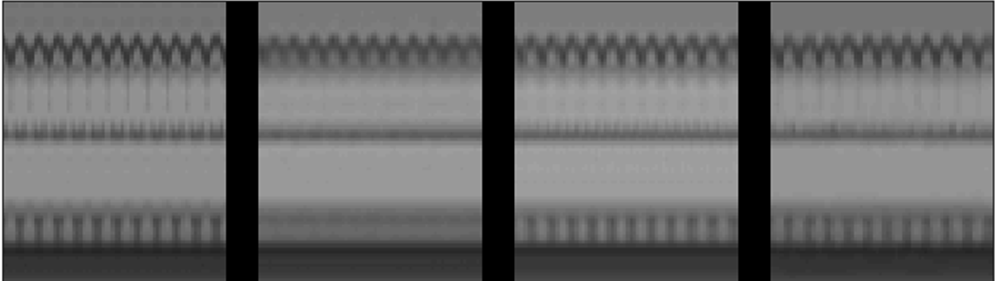
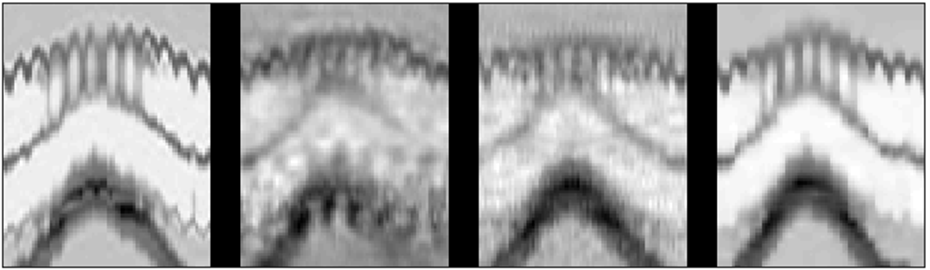
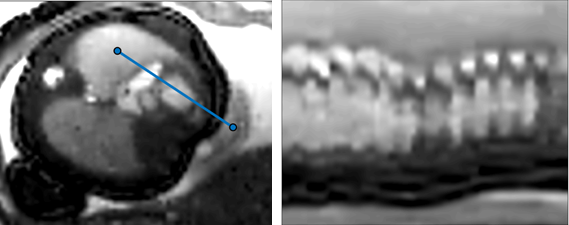
Without motion SSIM ranged from 0.93 to 0.98 depending on the reconstruction. In the presence of motion, image quality rapidly degraded for k-t SENSE and L plus S reconstructions but not ICTGV reconstructions. SSIM ranged from 0.52 to 0.70 for k-t SENSE, 0.72 to 0.81 for L plus S, and 0.90 to 0.94 for ICTGV. In figures 3 and 4 spatial and temporal blurring may be seen in both the k-t SENSE images and the L plus S images. Meanwhile in the M-mode trace of the ICTGV image in figure 4, the pulsation of the fetal heart is still visible. A single frame of an ICTGV reconstruction and an accompanying M-mode trace is demonstrated for a Philips 1.5T scanner (figure 5). We remark that the pulsation of the heart is evident with the actual reconstruction. Furthermore, this acquisition happened to occur during a period of fetal motion. We remark that in the real scan ICTGV evidently captures the expansion and contraction of the fetal heart even in the presence of motion.DISCUSSION
Since random fetal motion is always a possibility during acquisition of fetal images, robustness to motion is a key feature of any reconstruction algorithm designed for fetal imaging. Little variation in SSIM was observed under ideal motion-free simulation conditions. However, ICTGV was found to perform significantly better in the presence of fetal motion. Actual ICTGV images demonstrate that real-time images acquired at a frame rate of 65 ms can capture the dynamics of the fetal heart, and minor imperfections in the pulse sequence due to eddy currents do not corrupt the acquisition. Comparing ICTGV and k-t SENSE acquisitions the ICTGV acquisition had the further advantage that no additional training or low-resolution data was required. At high undersampling factors where each frame of k-space is only reconstructed from 20 lines or fewer, avoiding acquisition of a separate low-resolution scan can significantly shorten imaging time.CONCLUSION
Due to its robustness to random motion, ICTGV has great potential for fetal imaging applications. Further work will combine this acquisition with slice-to-volume registration and super-resolution reconstruction for anatomic and flow imaging.Acknowledgements
No acknowledgement found.References
1. van Amerom JF, Lloyd DF, Price AN, Kuklisova Murgasova M, Aljabar P, Malik SJ, Lohezic M, Rutherford MA, Pushparajah K, Razavi R, Hajnal JV. Fetal cardiac cine imaging using highly accelerated dynamic MRI with retrospective motion correction and outlier rejection. Magn Reson Med. 2018 ;79(1):327-38.
2. van Amerom JF, Lloyd DF, Deprez M, Price AN, Malik SJ, Pushparajah K, van Poppel MP, Rutherford MA, Razavi R, Hajnal JV. Fetal whole‐heart 4D imaging using motion‐corrected multi‐planar real‐time MRI. Magn Reson Med. 2019;82(3):1055-72.
3. Roberts TA, van Amerom JF, Uus A, Lloyd DF, van Poppel MP, Price AN, Tournier JD, Mohanadass CA, Jackson LH, Malik SJ, Pushparajah K. Fetal whole heart blood flow imaging using 4D cine MRI. Nat Commun. 2020;11(1):1-3.
4. Tsao J, Boesiger P, Pruessmann KP. k‐t BLAST and k‐t SENSE: dynamic MRI with high frame rate exploiting spatiotemporal correlations. Magn Reson Med. 2003;50(5):1031-42.
5. Otazo R, Candes E, Sodickson DK. Low‐rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. Magn Reson Med. 2015; 73(3):1125-36.
6. Schloegl M, Holler M, Schwarzl A, Bredies K, Stollberger R. Infimal convolution of total generalized variation functionals for dynamic MRI. Magn Reson Med. 2017;78(1):142-55.
7. Ahmad R, Xue H, Giri S, Ding Y, Craft J, Simonetti OP. Variable density incoherent spatiotemporal acquisition (VISTA) for highly accelerated cardiac MRI. Magn Reson Med 2015;74(5):1266-78.
8. Roy CW, Marini D, Segars WP, Seed M, Macgowan CK. Fetal XCMR: a numerical phantom for fetal cardiovascular magnetic resonance imaging. J Cardiovasc Magn Reson. 2019 ;21(1):1-2.
Figures