3464
Radiomics to Predict Pathological Complete Response in Patients with Triple Negative Breast Cancer1University of Washingon, Seattle, WA, United States, 2University of Washington, Seattle, WA, United States, 3Vanderbilt University, Nashville, TN, United States
Synopsis
Radiomics is an advancing field of medical image analysis based on extracting large sets of quantitative features that can be used for outcome modeling for clinical decision support. Our study investigated the value of radiomics features extracted from pre-treatment dynamic contrast-enhanced MRI for the prediction of neoadjuvant chemotherapy response in patients with triple-negative breast cancer. In a retrospective cohort of 103 TNBC patients, radiomics-based models using post-contrast images and kinetics maps were moderately predictive of pathologic response, and lesion size and shape features were the most consistent predictors across all image types.
Introduction
Triple-negative breast cancer (TNBC) is an aggressive subtype of breast cancer associated with poorer patient prognosis compared to non-TNBC subtypes1,2. TNBC patients with locally advanced disease are often treated with neoadjuvant chemotherapy (NAC). Because only 27-51% of TNBC patients achieve pCR3,4, there is a need to improve pCR prediction to guide treatment selection and optimize patient outcomes. New immunotherapy agents hold promise to dramatically improve outcomes in some women but come with serious side effects and variable response rates5; thus, identification of new biomarkers to better select responders to these novel treatments is imperative. Radiomics analysis applied to dynamic contrast-enhanced (DCE) MRI data has shown utility for prediction of disease-free survival in TNBC patients6,7. The purpose of our study was to evaluate the performance of radiomics-based models derived from pre-treatment DCE-MRI for the prediction of NAC response in TNBC.Methods
Subjects:Women with locally advanced TNBC who underwent pre-treatment breast MRI and NAC at our institution from 2005-2019 were retrospectively identified for this study. Pathology at surgery established the NAC response, with pCR defined as no residual invasive cancer present within the breast.MRI Acquisition: Patients were imaged with a 1.5T GE Signa (GE Healthcare, Waukesha, WI) or 3T Philips Achieva (Philips Healthcare, Best, the Netherlands) clinical scanner with a dedicated breast coil. DCE-MRI was acquired with a fat suppressed, 3D fast gradient echo sequence with one pre-contrast and at least three post-contrast acquisitions, with the first centered at 1.5-2 minutes, and last at 6-8 minutes after injection of a gadolinium-based MR contrast agent (0.1mmol/kg-body weight gadodiamide or gadoteridol). Images were acquired with in-plane resolution 0.5-1mm and slice thickness 1.3-2.2mm.
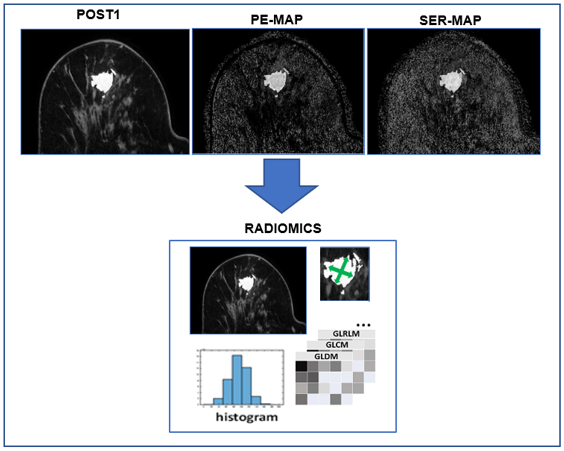
Radiomics Analysis: Lesion regions-of-interest (ROIs) were segmented from DCE-MRI subtraction images (post-contrast minus pre-contrast) using fuzzy c-means clustering. Radiomics analysis was performed on the first post-contrast MRI (Post1) and calculated parameter maps of percent enhancement (PE) and signal enhancement ratio (SER), which provide measures of early and late phase contrast kinetics, respectively8. Prior to feature extraction, voxels were isotropically resampled, image intensity values within each ROI were scaled using the minimum and maximum values, and ROI gray levels were discretized. Radiomic feature extraction was performed using 3D Slicer (3D Slicer v4.11.0, https://www.slicer.org) and pyradiomics9 software. For each lesion and image type (Post1, PE, SER), a total of 108 standardized radiomics features were generated of the following categories: (1) first-order voxel gray level histogram statistics, (2) 3-D ROI shape-based descriptors, and (3) texture features.
Statistical Analysis: Univariate associations of select features with NAC outcome were evaluated using Wilcoxon rank sum test. Radiomic features’ intercorrelations were assessed with Pearson correlation coefficient, and only those with r<0.95 were retained for further analysis. Three predictive models were fit and evaluated using radiomics features derived from 1) Post1, 2) PE maps and 3) SER maps. Predictive performance of these features was assessed with logistic regression models with regularization using least absolute shrinkage and selection operator (LASSO). Optimal LASSO shrinkage parameter was selected using 5-fold cross-validation. An average cross-validation area under the receiver operating characteristic curve (AUCCV) was used to assess the predictive performance of each competing model. Throughout, p<0.05 was considered statistically significant.
Results
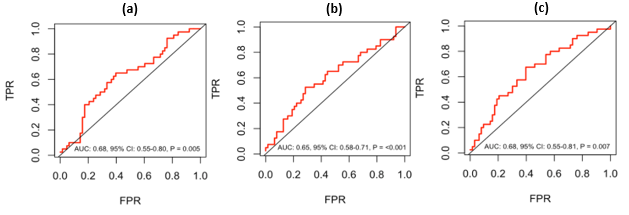
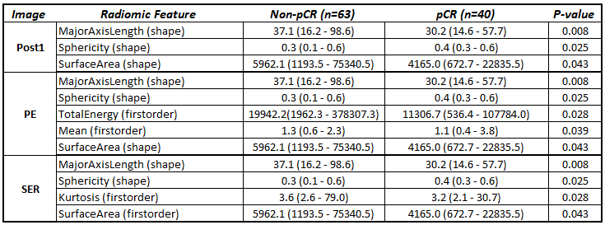
103 women with TNBC were retrospectively identified for this study (median age: 49, range 26 – 79 years), of which 40 (39%) achieved pCR. After evaluating intercorrelations of the initial 108 radiomic features, 29, 38 and 44 features were retained for further analysis of the of the Post1, PE, and SER radiomics features, respectively. The final cross-validated and LASSO-regularized models resulted in 14, 12 and 14 selected features from Post1, PE, and SER radiomics, respectively. All features with univariate associations of p<0.05 are shown in Table 1, with shape and size related features consistently demonstrating high significance across the three image types. All three models showed moderate performance for prediction of pCR from baseline DCE-MRI (Post1: AUCCV = 0.68, p = 0.005; PE: AUCCV = 0.65, p < 0.001; SER: AUCCV = 0.68, p = 0.007, Table 2).Discussion and Conclusion
Radiomics models derived from pre-treatment DCE-MRI provided modest value to predict pCR in women with TNBC undergoing standard-of-care NAC. Comparable performance was obtained from early post-contrast images, PE, and SER maps. Although PE and SER offer internal image normalization, radiomics analysis of a single DCE-MRI volume is more straightforward and does not require coregistration to correct for patient motion. Radiomics shape and size features were the primary drivers of model performance across the three models, which is consistent with established clinical markers (e.g., tumor size and stage); these quantitative parameters provide a potentially more automated and reproducible measure. Furthermore, integration of radiomics models with established pathology-based markers such as tumor-infiltrating lymphocytes (TILs) concentration10, tumor stage, grade, and Ki-67 may provide iterative value for pCR prediction.Acknowledgements
This research was funded by NIH/NCI P30 CA015704 and R01CA248192.References
1. Liedke C., et al. Response to Neoadjuvant Therapy and Long-Term Survival in Patients with Triple-Negative Breast Cancer. JCO 26, 2008: 1275-1281
2. Li X., Yang J, Peng L., Sahin A.A.,et al. Triple-negative breast cancer has worse overall survival and cause-specific survival than non-triple-negative breast cancer. Breast Cancer Res Treat. 2017 Jan;161(2):279-287
3. Golshan, M. et al. Breast Conservation After Neoadjuvant Chemotherapy for Triple-Negative Breast Cancer: Surgical Results From the BrighTNess Randomized Clinical Trial. JAMA Surg155, e195410 (2020).
4. von Minckwitz, G. et al. Definition and Impact of Pathologic Complete Response on Prognosis After Neoadjuvant Chemotherapy in Various Intrinsic Breast Cancer Subtypes. Journal of Clinical Oncology 30, 1796–1804 (2012).
5. Schmid P, Cortes J, Pusztai L, McArthur H, et al. KEYNOTE-522 Investigators. N Engl J Med. 2020 Feb 27; 382(9):810-821.
6. Kim S., Kim M.J., Kim E-K., Yoon J.H., et al. MRI Radiomic Features: Association with Disease-Free Survival in Patients with Triple-Negative Breast Cancer. Scientific Reports 2020 Feb; 10(1):3750
7. Wu J., Li X., Teng X., Rubin DL., et al. Magnetic resonance imaging and molecular features associated with tumor-infiltrating lymphocytes in breast cancer. Breast Cancer Res. 2018 Sep 3;20(1):101
8. Xiao, J., Rahbar, H., Hippe, D.S. et al. Dynamic contrast-enhanced breast MRI features correlate with invasive breast cancer angiogenesis. npj Breast Cancer 7, 42 (2021).
9. Griethuysen, J. J. M., Fedorov, A., Parmar, et al. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Research, 2017; 77(21), e104–e107
10. Gao Z.H., Li C.X., Liu M., Jiang J.Y.. Predictive and prognostic role of tumour-infiltrating lymphocytes in breast cancer patients with different molecular subtypes: a meta-analysis. BMC Cancer. 2020 Nov 25;20(1):1150
Figures