3445
Synergistic Combination of Golden-angle Radial Sampling and Dual-Subspace Modeling for Rapid and Robust High Spatiotemporal Resolution MRA1USC Stevens Neuroimaging and Informatics Institute, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 2Department of Neurology, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States
Synopsis
This study proposes a rapid and robust ASL-based time-resolved MRA technique with high spatiotemporal resolution termed Dual-Subspace MRA (DS-MRA), which employs subspace modeling from both temporal and control/label dimensions as sparsity constraints to improve the robustness of image reconstruction with under-sampled golden-angle radial dynamic MRA. The performance of DS-MRA was compared with conventional iGRASP and 5-dimensional GRASP. Our preliminary data suggests that DS-MRA outperforms conventional GRASP reconstructions with less residual streaking artifacts and noise, especially at higher acceleration rates.
Purpose
ASL-based dynamic MR angiography (ASL-dMRA) has demonstrated good potential in characterizing dynamic flow patterns in various cerebrovascular diseases1–3. Both high spatial and temporal resolutions are desired in clinical applications, which leads to lengthened scan time especially using conventional multi-phase segmented cartesian acquisition 4–7. Recently, a stack-of-stars golden-angle radial acquisition has been proposed in ASL-dMRA, which dramatically reduces the scan time by 3-fold 3,8. Different from contrast-enhanced dynamic MRI, the label and control measurements in ASL-dMRA generate an additional dimension which can be modeled as sparsity constraint to improve the performance of image reconstruction. In this study, we propose a dual-subspace reconstruction framework budded Dual-Subspace MRA (DS-MRA) by employing subspace modeling from both temporal and control/label dimensions as sparsity constraints to improve the performance of under-sampled dynamic MRA reconstruction with golden-angle radial sampling.Method
Theory: iGRASP is a conventional temporal constraint-based compressed sensing model for golden-angle radial acquisition (Fig 1(a)) 9. Based on the standard GRASP, we explored a new 5-dimensional GRASP (5D-GRASP) that exploits the sparsity along both temporal and phase dimensions (label and control measurements are jointly concatenated as a phase dimension) (Fig. 1(b)). 5D-GRASP takes advantage of additional sparsity property in label/control MRA data, leading to more accurate image reconstruction.Subspace model is a novel way of exploiting the low-rank property, having its roots in globally low-rankness of dynamic MRI, based on the hypothesis that a dynamic image series can be represented in a lower dimensional subspace when the corresponding temporal basis is known in advance 9,10. We incorporated the subspace model into the previous compound constraint including sparsity regularization in both temporal and phase dimensions (Fig 1(b)), as shown in Figure 1(c).
Figure 2 indicates the detailed reconstruction framework of Dual-Subspace MRA, which is constructed by two steps: low-resolution subspace image reconstruction and high-resolution image restoration. Temporal basis and corresponding coefficients are learned based on low-spatial-resolution reconstructed image series. Subsequently, full-resolution image series (5D image set: x-y-slice-t-phase) are restored based on pre-learned dominant components in subspace.
MRI data acquisition: The MRA experiments were carried out on a 3 T Prisma MR scanner (Siemens AG Medical Solutions, Erlangen, Germany) using a 20-element head coil array. Dynamic MRA data were acquired using pulsed ASL prepared TrueFISP sequence with 3D stack-of-stars golden-angle radial sampling scheme 3,8. The imaging parameters included: FOV=256×256×48 mm3, TR/TE = 4.86/2.43 ms, 32 slices, flip angle = 25°, bandwidth = 814 Hz/pixel, number of readout points in each spoke 512, oversampling ratio 2, number of spokes 500, resulting in a spatial resolution of 1×1×1.5 mm3.
Dynamic MRA images were reconstructed using iGRASP, 5D-GRASP and Dual-Subspace methods. All image reconstructions were implemented in Matlab (R2019b; the Mathworks, Natick, MA, USA), for off-line reconstruction on a Linux server (CentOS, Intel(R) Core (TM) i9-7920X CPU @ 2.90 GHz and 128-GB RAM).
Maximum intensity projection (MIP) images were generated using the subtraction of reconstructed control and label images to delineate the blood flow dynamics.
The time courses of three ROIs in middle cerebral artery and posterior cerebral artery were extracted to evaluate the temporal fidelity of flow dynamics. CG-SENSE-based reconstruction was used as the reference, which reconstructed images frame-by-frame without involving any temporal correlation of dMRA 7,11.
Results & Discussion
Figure 3 shows the reconstructed images using iGRASP, 5D-GRASP, and DS-MRA. The proposed Dual-subspace scheme outperformed the conventional iGRASP and improved 5D-GRASP methods with lower noise level and fewer streaking artifacts. The conventional iGRASP exhibits the highest noise level. This supports the hypothesis that better performance can be achieved by employing the additional sparsity property along label/control dimension in ASL-based MRA data. The time courses of three ROIs indicated that the proposed scheme does not induce apparent temporal blurring.Figure 4 shows the MIP image of a single frame. One can appreciate that the proposed Dual-subspace model results in better image quality than the other investigated approaches, including higher SNR, lower noise level, and fewer streaking artifacts. More importantly, DS-MRA generates better reconstructed images without any detail loss. When comparing the restoration of small blood vessels, it can be clearly seen that the proposed Dual-subspace model preserves small details more clearly (see green arrows). When looking into the areas in green boxes, there are some blurring in 5D-GRASP. In iGRASP, some small details were almost submerged by noise and under-sampling induced artifacts. DS-MRA remained the best performance with higher acceleration rate. This suggests that DS-MRA can further improve the under-sampling rate of dMRA. Due to the superior performance of the proposed dual-subspace strategy with higher acceleration rates, it may also have clinical potential for real-time imaging.
Further studies will focus on the optimization of the algorithm to replace current time-consuming conjugate gradient approach, for example, FISTA12. In addition, the dual-subspace model with novel trajectory like rotating golden angle in partition direction would further improve the efficiency of k-space coverage.
Conclusion
The proposed Dual-subspace approach is a dual constraints subspace model for high spatiotemporal ASL-dMRA. Compared to conventional iGRASP-type techniques, it offers better image quality, including higher SNR and fewer streaking artifacts. Therefore, it has a latent advantage of better temporal resolution due to higher reconstruction accuracy.Acknowledgements
This work was supported by NIH grants K25 AG056594, R01NS118019, RF1AG072490, and BrightFocus foundation A20201411S.
References
1. Yan L, Wang S, Zhuo Y, et al. Unenhanced dynamic MR angiography: High spatial and temporal resolution by using true FISP-based spin tagging with alternating radiofrequency. Radiology. 2010;256(1):270-279.
2. Yu S, Yan L, Yao Y, et al. Noncontrast dynamic MRA in intracranial arteriovenous malformation (AVM): Comparison with time of flight (TOF) and digital subtraction angiography (DSA). Magn Reson Imaging. 2012;30(6):869-877.
3. Song HK, Yan L, Smith RX, et al. Noncontrast enhanced four-dimensional dynamic MRA with golden angle radial acquisition and K-space weighted image contrast (KWIC) reconstruction. Magn Reson Med. 2014;72(6):1541-1551.
4. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: Sensitivity encoding for fast MRI. Magn Reson Med. 1999;42(5):952-962.
5. Griswold MA, Jakob PM, Heidemann RM, et al. Generalized Autocalibrating Partially Parallel Acquisitions (GRAPPA). Magn Reson Med. 2002;47(6):1202-1210.
6. Chen Z, Xia L, Liu F, et al. An improved non-Cartesian partially parallel imaging by exploiting artificial sparsity. Magn Reson Med. 2017;78(1):271-279.
7. Chen Z, Kang L, Xia L, et al. Technical Note: Sequential combination of parallel imaging and dynamic artificial sparsity framework for rapid free-breathing golden-angle radial dynamic MRI: K-T ARTS-GROWL. Med Phys. 2018;45(1):202-213.
8. Zhou Z, Han F, Yu S, et al. Accelerated noncontrast-enhanced 4-dimensional intracranial MR angiography using golden-angle stack-of-stars trajectory and compressed sensing with magnitude subtraction. Magn Reson Med. 2018;79(2):867-878.
9. Feng L, Wen Q, Huang C, Tong A, Liu F, Chandarana H. GRASP-Pro: imProving GRASP DCE-MRI through self-calibrating subspace-modeling and contrast phase automation. Magn Reson Med. 2020;83(1):94-108.
10. Cao X, Wang K, Liao C, et al. Efficient T2 mapping with blip-up/down EPI and gSlider-SMS (T2-BUDA-gSlider). Magn Reson Med. 2021;86(4):2064-2075.
11. Pruessmann KP, Weiger M, Börnert P, Boesiger P. Advances in sensitivity encoding with arbitrary k-space trajectories. Magn Reson Med. 2001;46(4):638-651.
12. Beck A, Teboulle M. A Fast Iterative Shrinkage-Thresholding Algorithm. Soc Ind Appl Math J Imaging Sci. 2009;2(1):183-202.
Figures
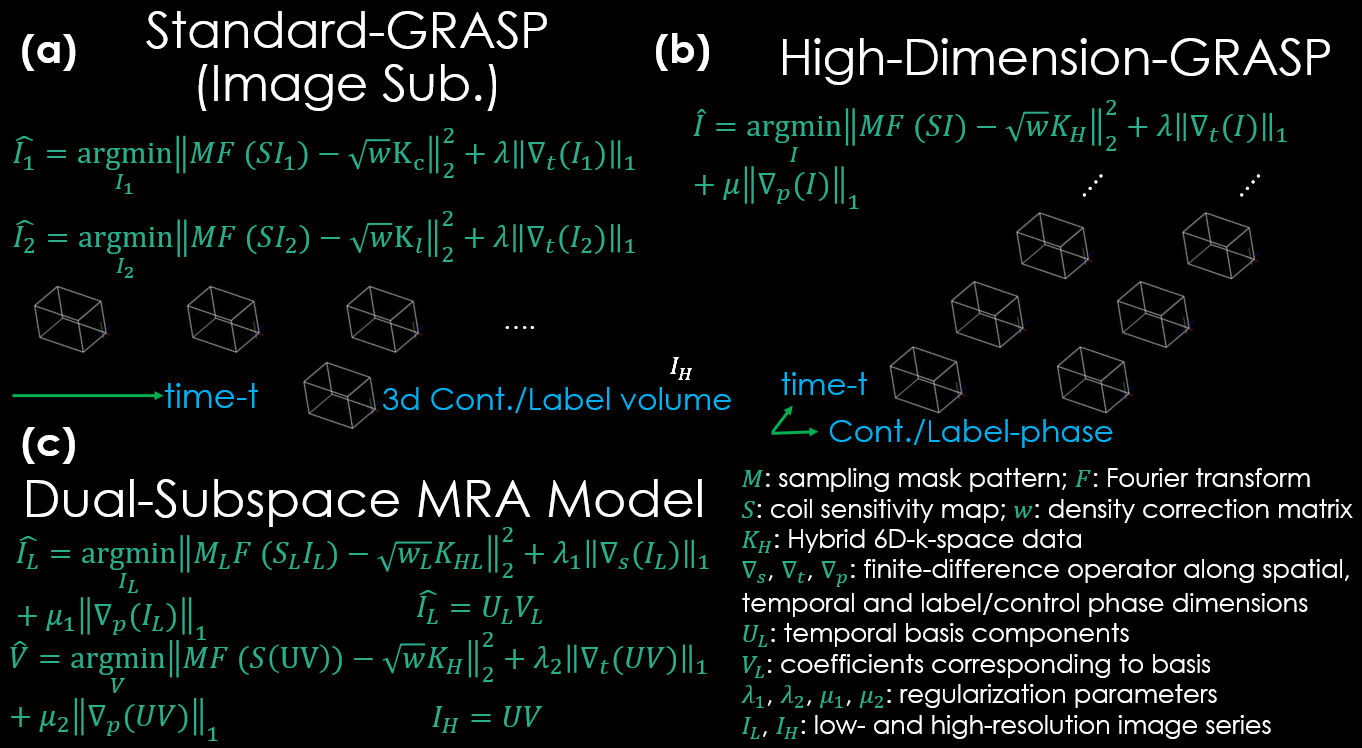
FIG. 1. Comparison of the reconstruction models. (a) conventional iGRASP. (b) 5D-GRASP. (c) Dual-subspace MRA.
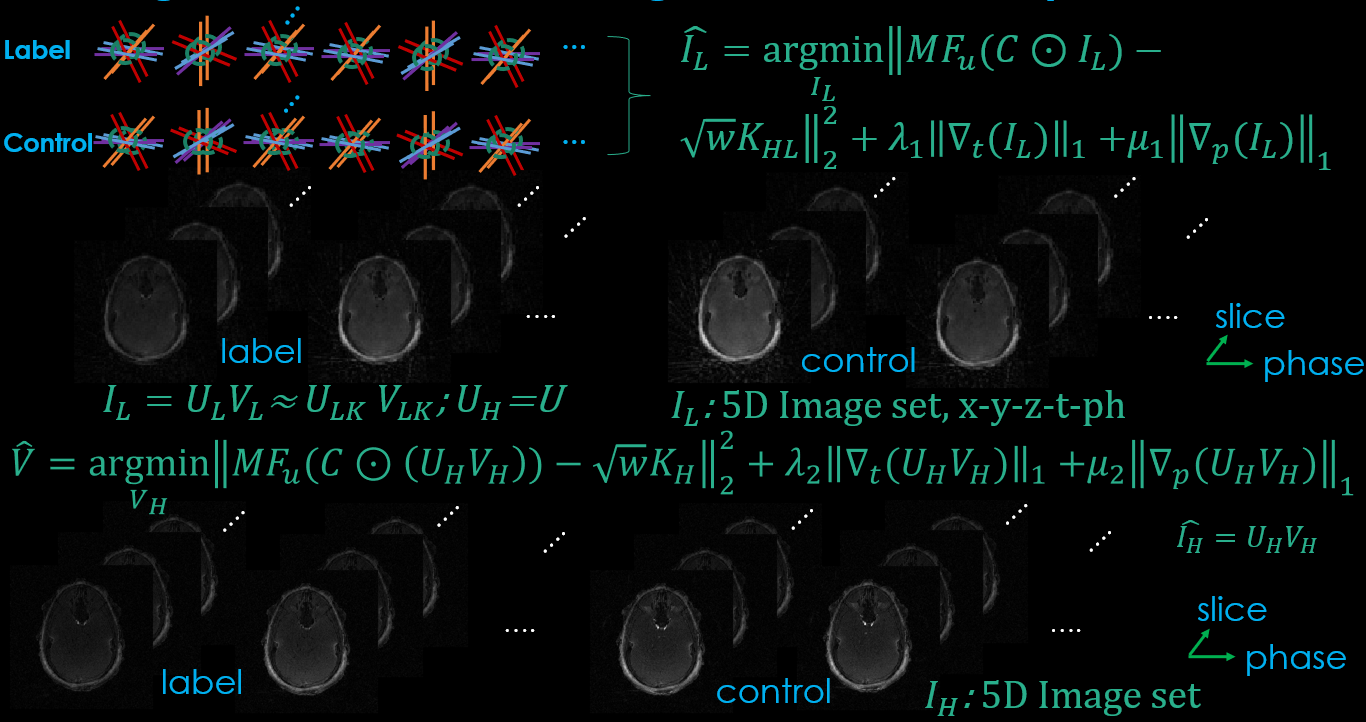
FIG. 2. Detailed image reconstruction framework of the proposed Dual-subspace MRA. The size of low-resolution image series is 96 x 96.
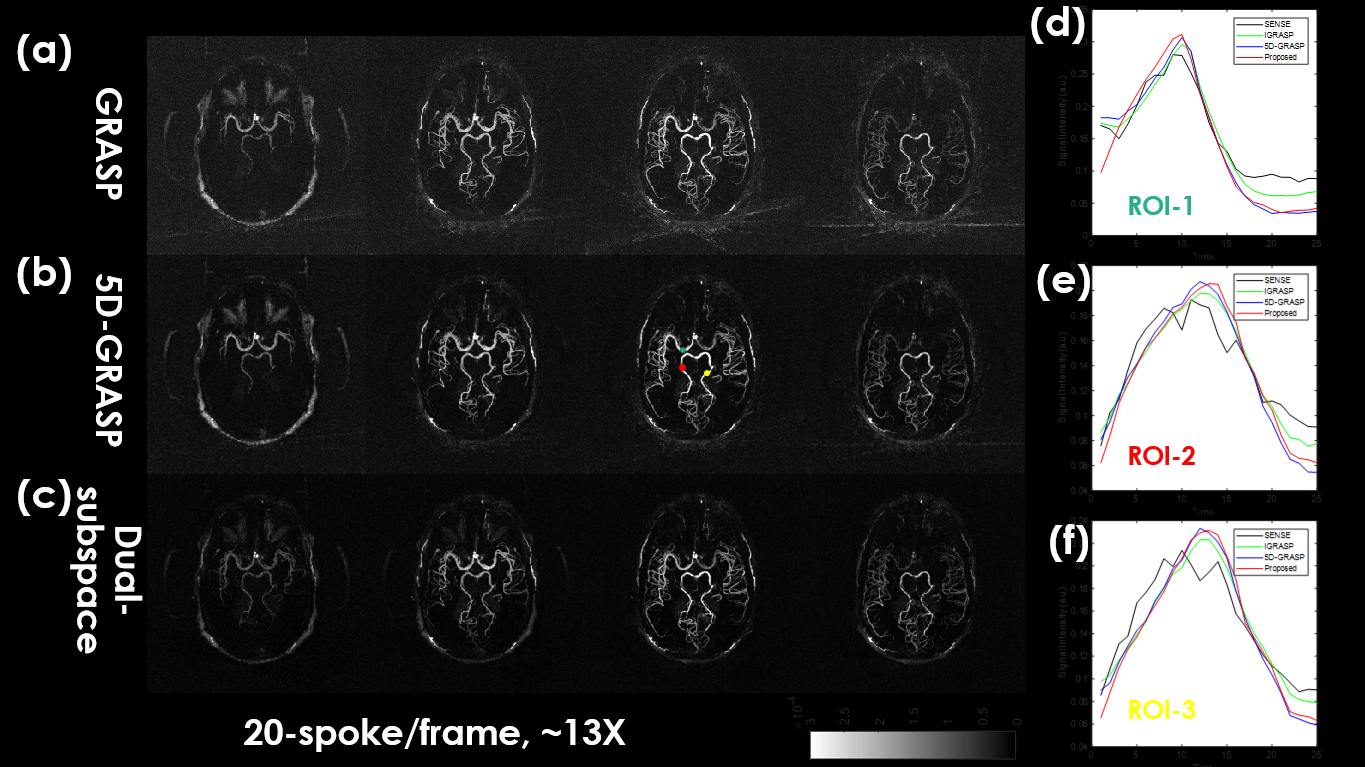
FIG. 3. The comparison of reconstructed images among different approaches for in vivo dynamic MRA dataset. (a) Image reconstruction of conventional iGRASP. (b) Image reconstruction of 5D-GRASP. (c) Image reconstruction of the proposed Dual-subspace MRA. (d)-(f) The comparison of signal-intensity time courses of three ROIs (displayed in third column of 5D-GRASP reconstruction).
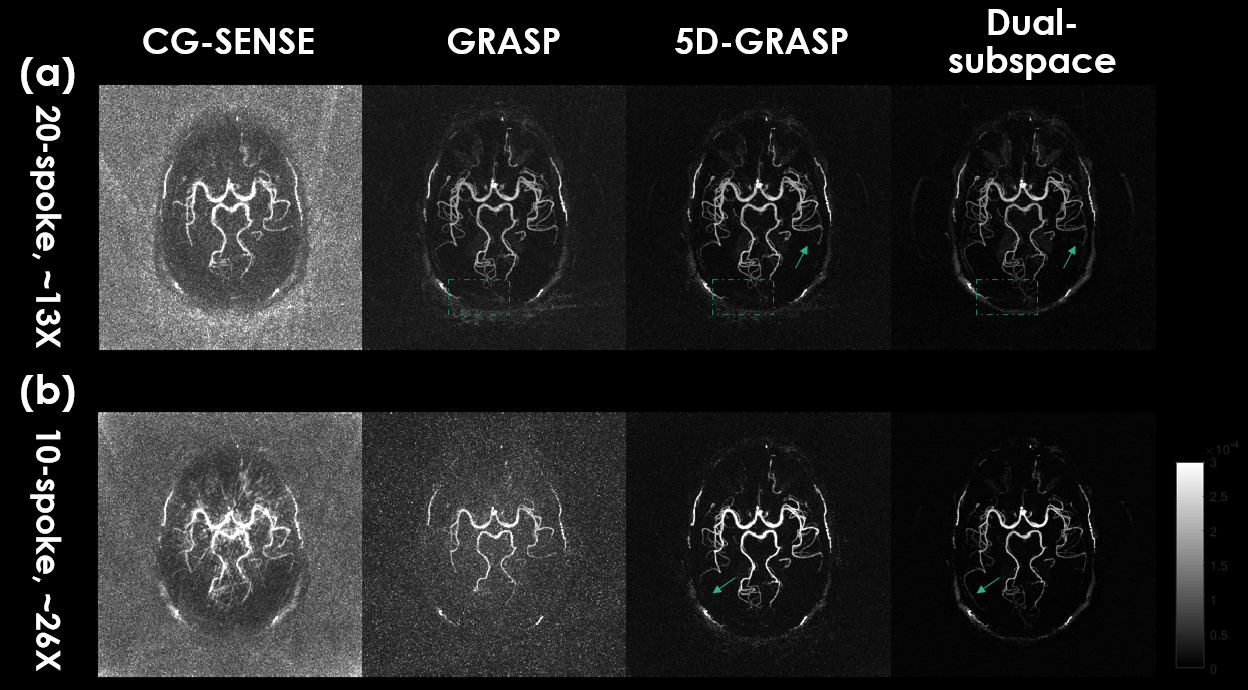
FIG. 4. The reconstructed results of CG-SENSE (first column), iGRASP (second column), 5D-GRASP (third column) and the proposed Dual-subspace model (last column). (a) 20-spoke results. (b) 10-spoke results.