3405
Cerebellar damage, by medulloblastoma and related surgery, induces global cerebral microstructural1Department of Diagnostic Imaging, St. Jude Children's Research Hospital, Memphis, TN, United States, 2Department of Pediatrics, St. Jude Children's Research Hospital, Memphis, TN, United States
Synopsis
Survivors of medulloblastoma patients frequently have cognitive impairment, which is currently thought to be due to radiation and chemotherapy. In this work, we have showed that there is widespread changes in diffusion tensor parameters in cerebral white and gray matters, suggestive of brain microstructure damage, even before start of radiation and chemotherapy and not related to hydrocephalus.
Introduction
Cognitive impairment following treatment of medulloblastoma (MB), the most common malignant brain tumor in children, is widespread. Processing speed, attention, working memory, and executive functions are the most affected domains, leading to academic failure, poor quality of life, and high unemployment rates.1-4 These decline in cognitive domains positively correlate with radiation dose and negatively correlate with age at diagnosis, 5,6 and have been associated with regional7-10 and global10,11 white matter structural changes and altered structural brain connectivity,12,13 as evidenced by diffusion tensor imaging (DTI). Craniospinal irradiation (CSI) and chemotherapy have long been thought to be primarily responsible for these microstructural damages.5,14,15 In this work, we compared DTI measures of microstructural damages (fractional anisotropy, FA; apparent diffusion coefficient, ADC; radial diffusivity, rD; axial diffusivity, aD) in cerebral gray and white matter in MB patients before CSI and chemotherapy have begun.Methods
Subjects: In this study we included 30 medulloblastoma patients (range, 12 to 21; mean age 15.8 years, 19 male) imaged after resection of the tumor and before start of any therapy and compared them to a group of 35 healthy controls (range 12-22; mean 18.0 years, 17 male).Image acquisition: Both the study and control population were scanned on Siemens 3T magnets (Prisma and Skyra) using identical imaging protocol that included 1 mm3 isotropic 3D T1 MPRAGE and 64 directions DTI sequence (b=0, 1500 s/mm2). B0 images were acquired twice with opposite phase encoding directions to accommodate for EPI distortion.
Image analysis: Diffusion data were corrected for eddy current distortions and EPI distortions before being fit to a tensor model. The diffusion and T1 image were registered together. The T1 image was used to segment the brain for all participants using Freesurfer 6.0 with brain regions parceled based on Desikan-Killany atlas. DTI parameters were extracted from each brain regions. The gray and white matter regions were further classified based on lobar distribution. The cumulative volume of all the ventricles were calculated from the Freesurfer output. Additionally, we calculated the volumes of the resected portion of the cerebellum via an automated template normalization and comparison approach. Resection maps were inspected and adjusted (if needed) by trained personnel. The gap between the surgery and date of MRI acquisition was also captured.
Statistical analysis: A t-test was then used to assess the group differences between the controls and patient population. A linear regression analysis was performed to find correlation of the DTI parameters with ventricle volume, resected cerebellar volume and the gap between the surgery and MRI acquisition within the MB group. A Bonferroni correction was used to adjust the threshold for significance for all statistical tests from 0.05 to 0.0007 due to multiple comparisons.
Results
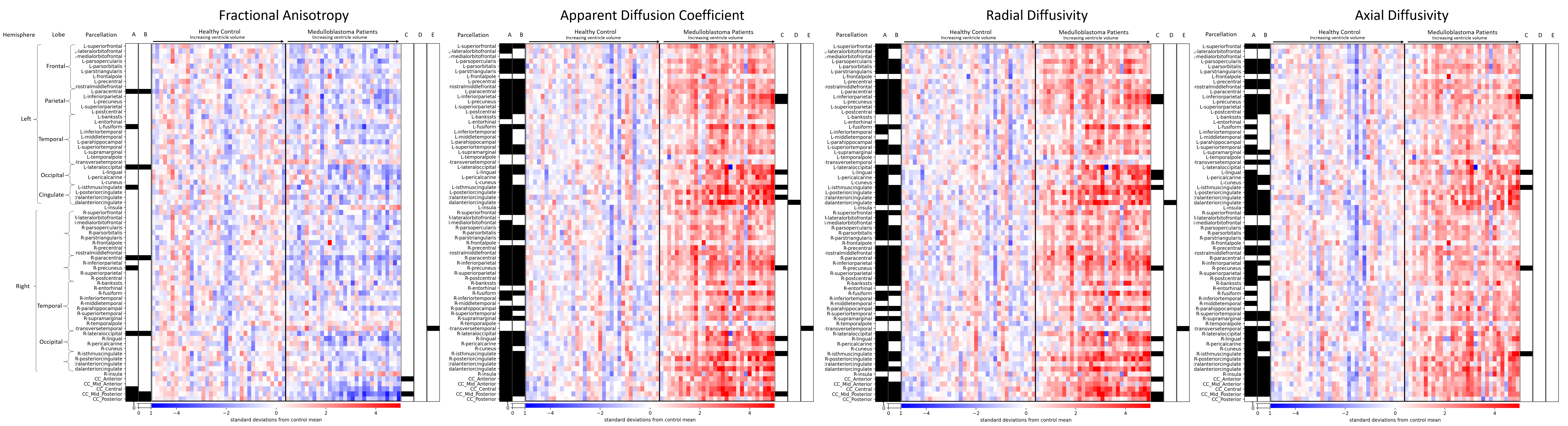
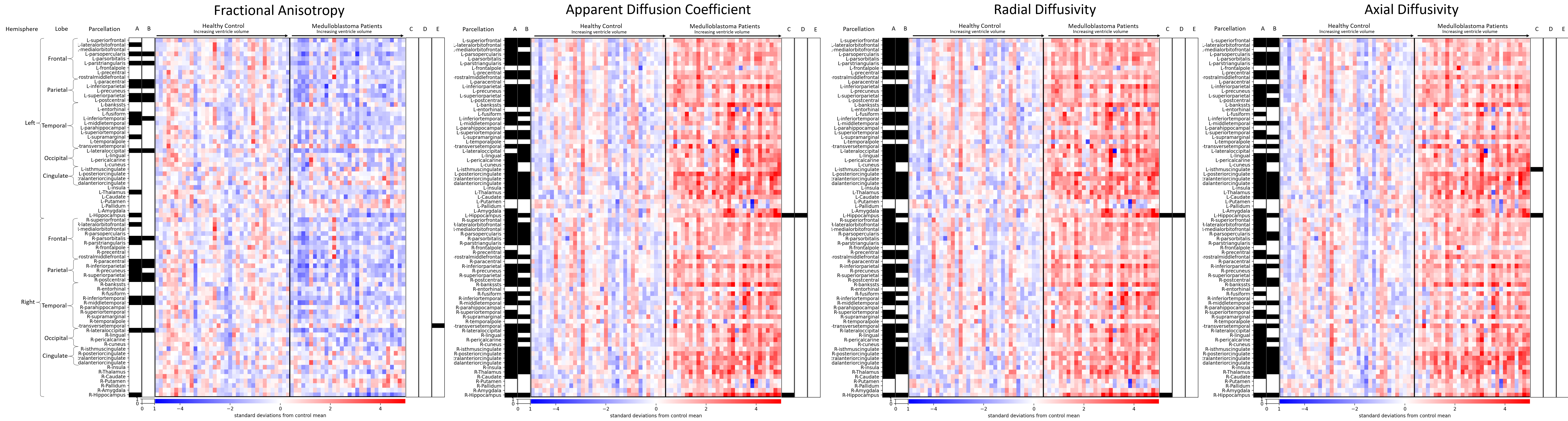
We find significantly increased diffusivity parameters (ADC, rD, and aD) across almost all the white (columns A, Figure 1) and gray matter (columns A, Figure 2) regions in group comparisons between control subjects and MB patients. FA (columns A, Figure 1) was different in many white and gray matter regions as well. Statistically significant similar differences were also observed across white and gray matter regions when we did another group comparison (columns B on Figure 1 & 2) between control subjects and MB patients with similar cumulative ventricular size, excluding all the MB patients who had ventricle volume larger than the largest ventricle volume of the control group from the analysis. Other than the corpus callosum, paracentral and lateral occipital lobe white matter areas and bilateral hippocampi, the regression analysis did not demonstrate any correlation (r2<0.01) of diffusion parameters (FA, ADC, rD, and aD) with cumulative volume of the ventricles (column Cs on Figure 1, & 2). There was also no correlation (r2<0.01) between diffusion parameters (FA, ADC, rD, and aD) with resected cerebellar volume (Column Ds on Figure 1 & 2), and the gap between surgery and MRI acquisition (Column Es on Figure 1 & 2) in any gray and white matter regions.Discussion
This work shows that there are global, statistically significant differences in diffusion parameters between healthy controls and medulloblastoma patients even before start of CSI or chemotherapy, not explained by large size of the ventricles (hydrocephalus). We then hypothesized that the volume of the resected cerebellum and gap from surgery might be contributing to these differences, which we proved not to be the case. We believe that disruptions of the cerebellum in MB patients, by the tumor or by the surgical resection or by combination of these two, influence these widespread cerebral microstructural abnormalities.Conclusion
The results of this study show that widespread cerebral microstructural abnormalities are present even before start of CSI and chemotherapy and are not contributed by ventricular enlargement. This suggests that there might be additional mechanisms contributing to cerebral microstructural alterations in the post treatment setting in MB patients, in addition to the currently known factors such as hydrocephalus, radiation therapy and chemotherapy.Acknowledgements
The authors thank St. Jude/ALSAC for funding and support on this project.References
1. Ris MD, Packer R, Goldwein J, Jones-Wallace D, Boyett JM. Intellectual outcome after reduced-dose radiation therapy plus adjuvant chemotherapy for medulloblastoma: a Children's Cancer Group study. J Clin Oncol. Aug 1 2001;19(15):3470-6. doi:10.1200/JCO.2001.19.15.3470
2. Szentes A, Eros N, Kekecs Z, et al. Cognitive deficits and psychopathological symptoms among children with medulloblastoma. Eur J Cancer Care (Engl). Nov 2018;27(6):e12912. doi:10.1111/ecc.12912
3. Yoo HJ, Kim H, Park HJ, Kim DS, Ra YS, Shin HY. Neurocognitive Function and Health-Related Quality of Life in Pediatric Korean Survivors of Medulloblastoma. J Korean Med Sci. Nov 2016;31(11):1726-1734. doi:10.3346/jkms.2016.31.11.1726
4. Saury JM, Emanuelson I. Cognitive consequences of the treatment of medulloblastoma among children. Pediatr Neurol. Jan 2011;44(1):21-30. doi:10.1016/j.pediatrneurol.2010.07.004
5. Northcott PA, Robinson GW, Kratz CP, et al. Medulloblastoma. Nat Rev Dis Primers. Feb 14 2019;5(1):11. doi:10.1038/s41572-019-0063-6
6. Camara S, Fournier MC, Cordero P, et al. Neuropsychological Profile in Children with Posterior Fossa Tumors with or Without Postoperative Cerebellar Mutism Syndrome (CMS). Cerebellum. Dec 12 2019;doi:10.1007/s12311-019-01088-4
7. Glass JO, Ogg RJ, Hyun JW, et al. Disrupted development and integrity of frontal white matter in patients treated for pediatric medulloblastoma. Neuro Oncol. Oct 1 2017;19(10):1408-1418. doi:10.1093/neuonc/nox062
8. Scantlebury N, Bouffet E, Laughlin S, et al. White Matter and Information Processing Speed Following Treatment With Cranial-Spinal Radiation for Pediatric Brain Tumor. Neuropsychology. May 2016;30(4):425-38. doi:10.1037/neu0000258
9. Riggs L, Bouffet E, Laughlin S, et al. Changes to memory structures in children treated for posterior fossa tumors. J Int Neuropsychol Soc. Feb 2014;20(2):168-80. doi:10.1017/S135561771300129X
10. Moxon-Emre I, Bouffet E, Taylor MD, et al. Vulnerability of white matter to insult during childhood: evidence from patients treated for medulloblastoma. J Neurosurg Pediatr. Jul 2016;18(1):29-40. doi:10.3171/2016.1.PEDS15580
11. Rueckriegel SM, Bruhn H, Thomale UW, Hernaiz Driever P. Cerebral white matter fractional anisotropy and tract volume as measured by MR imaging are associated with impaired cognitive and motor function in pediatric posterior fossa tumor survivors. Pediatr Blood Cancer. Jul 2015;62(7):1252-8. doi:10.1002/pbc.25485
12. Duncan EC, Reddick WE, Glass JO, et al. Application of probabilistic fiber-tracking method of MR imaging to measure impact of cranial irradiation on structural brain connectivity in children treated for medulloblastoma. vol 9788. SPIE Medical Imaging. SPIE; 2016.
13. Oyefiade A, Beera K, Skocic J, De Medeiros C, Mabbott D. MBCL-34. STRUCTURAL CONNECTIVITY ABNORMALITY IN CHILDREN TREATED FOR MEDULLOBLASTOMA. Neuro-Oncology. 2018;20(suppl_2):i124-i124. doi:10.1093/neuonc/noy059.430
14. Palmer SL, Armstrong C, Onar-Thomas A, et al. Processing speed, attention, and working memory after treatment for medulloblastoma: an international, prospective, and longitudinal study. J Clin Oncol. Oct 1 2013;31(28):3494-500. doi:10.1200/JCO.2012.47.4775
15. Kieffer V, Chevignard MP, Dellatolas G, et al. Intellectual, educational, and situation-based social outcome in adult survivors of childhood medulloblastoma. Dev Neurorehabil. Jan 2019;22(1):19-26. doi:10.1080/17518423.2018.1424262
Figures