3383
3D T2-Weighted Rectal Cancer Imaging using a 3D Fast Spin Echo Sequence with Deep Learning Reconstruction
Sarah Palmquist1, Usama Salem1, Nir Stanietzky1, Jia Sun2, Xinzeng Wang3, Ersin Bayram3, Ken-Pin Hwang4, Jong Bum Son4, Peng Wei2, Randy Ernst1, Harmeet Kaur1, and Jingfei Ma4
1Abdominal Imaging, M.D. Anderson Cancer Center, Houston, TX, United States, 2Biostatistics, M.D. Anderson Cancer Center, Houston, TX, United States, 3GE Healthcare, Houston, TX, United States, 4Imaging Physics, M.D. Anderson Cancer Center, Houston, TX, United States
1Abdominal Imaging, M.D. Anderson Cancer Center, Houston, TX, United States, 2Biostatistics, M.D. Anderson Cancer Center, Houston, TX, United States, 3GE Healthcare, Houston, TX, United States, 4Imaging Physics, M.D. Anderson Cancer Center, Houston, TX, United States
Synopsis
Multiplanar
high resolution T2-weighted (T2W) imaging with a 2D fast spin echo (FSE)
sequence is currently an essential component of rectal cancer MRI. In this
work, we performed T2W imaging of rectal cancer with a 3D FSE sequence and
evaluated the quality and potential clinical value of the images after applying
a postprocessing deep learning reconstruction (DLR) algorithm. We found that
DLR images are non-inferior to conventional images and there are fair-moderate
inter-reader agreements in a large majority of the categories evaluated for
image quality and clinical usefulness.
Inrroduction
Multiplanar high resolution T2-weighted (T2W) imaging with a 2D fast spin echo (FSE) sequence is currently a fundamental part of rectal cancer imaging, both in the initial diagnosis/staging and assessment of treatment response. Compared to 2D FSE, a 3D FSE sequence can generate T2W images that are of contiguous thinner slice and formattable into any plane, thus potentially provide substantial scan time savings. However, 3D FSE images traditionally have the limitations of lower signal-to-noise ratio (SNR), lower image contrast, and increased susceptibility to artifacts. In this work, we performed T2W imaging of rectal cancer with a 3D FSE sequence and evaluated the quality and potential clinical value of the images after applying a postprocessing deep learning reconstruction algorithm (hereafter referred as DLR).Method
A total of 50 patients (all with a confirmed diagnosis of rectal cancer) were included in the study. All the patients were referred for a clinical MRI exam either for initial staging or for evaluation of treatment response. All the MRI exams were performed on GE 3T MR scanners with an external pelvic array coil. The typical scan parameters for 3D FSE imaging were: TR/TE=2500/132ms, ETL=100, FOV=18cm, acquisition matrix: 320x256, slice thickness=3.0/-15.mm, and a total of 72 slices in 3:56 minutes. In addition to the images by the conventional reconstruction (hereafter referred as conv), we applied a proprietary DLR algorithm provided to us by GE healthcare and obtained an additional set of images (hereafter referred as DLR).Three board-certified radiologists (with 23, 16, 8 years of experiences in abdominal imaging) reviewed and evaluated the conv and DLR images. Using a 3-point scale (1: good, 2: moderate, 3: poor) and based on their clinical experience in reading rectal cancer MRI, each radiologist independently scored overall SNR, motion artifacts, and overall image quality, as well as the clinical utility that includes definition of bowel wall layers, tumor invasion of muscularis propria, residual disease, fibrosis, nodal margin, and extra mural venous invasion. Further, each radiologist recorded their preferred images for each of the above category or a tie if there was no preference.
Summary statistics of the image quality evaluations were performed in frequency tables and percentages. Fleiss’ Kappa statistics was used to assess agreements between three readers. The proportion of DLR is preferred was estimated with 95% confidence interval by the method of Clopper and Pearson. The hypotheses of whether the proportions of DLR were preferred are greater than 50% were tested using the one-sided exact binomial test. Statistical analysis was carried out using R (version 3.6.3, R Development Core Team).
Results
All three readers have rated both DLR and conv images as moderate or good in >85% of the cases except for a few exception categories. These findings on an absolute scale indicate that 3D T2W images (either DLR or conv) are potentially acceptable for rectal cancer imaging. On a relative scale, the 3 readers rated DLR images as preferred or a tie in a majority of the cases (Table 1). Fair to moderate inter-reader agreements were found in the evaluation of all the categories except for fibrosis, tumor invasion of muscularis propria, and motion artifacts (Table 2).Conclusion
Our study demonstrated that 3D FSE or 3D FSE with DLR can be an acceptable option for T2W imaging of rectal cancer. Further, DLR was found to improve the overall quality and clinical usefulness of 3D FSE for imaging of rectal cancer. Future studies will include a direct comparison with the current standard of T2W imaging with 2D FSE.Acknowledgements
No acknowledgement found.References
1. Clopper, C.J. and Pearson, E.S. (1934) The Use of Confidence or Fiducial Limits Illustrated in the Case of the Binomial. Biometrika, 26, 404-413.2. Horvat N, Carlos Tavares Rocha C, Clemente Oliveira B, Petkovska I, Gollub MJ. MRI of Rectal Cancer: Tumor Staging, Imaging Techniques, and Management. Radiographics. 2019;39(2):367-387. doi:10.1148/rg.2019180114.
3. Kalisz KR, Enzerra MD, Paspulati RM. MRI Evaluation of the Response of Rectal Cancer to Neoadjuvant Chemoradiation Therapy. Radiographics. 2019;39(2):538-556. doi:10.1148/rg.2019180075.
4. Patel UB, Taylor F, Blomqvist L, et al. Magnetic resonance imaging-detected tumor response for locally advanced rectal cancer predicts survival outcomes: MERCURY experience. J Clin Oncol. 2011;29(28):3753-3760. doi:10.1200/JCO.2011.34.9068.
Figures
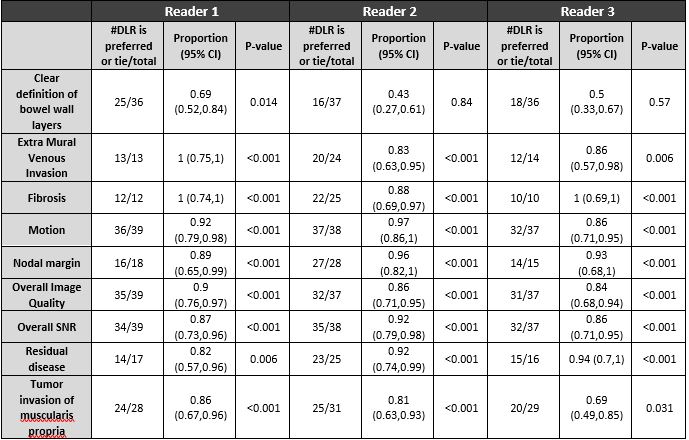
Table 1.

Table 2.
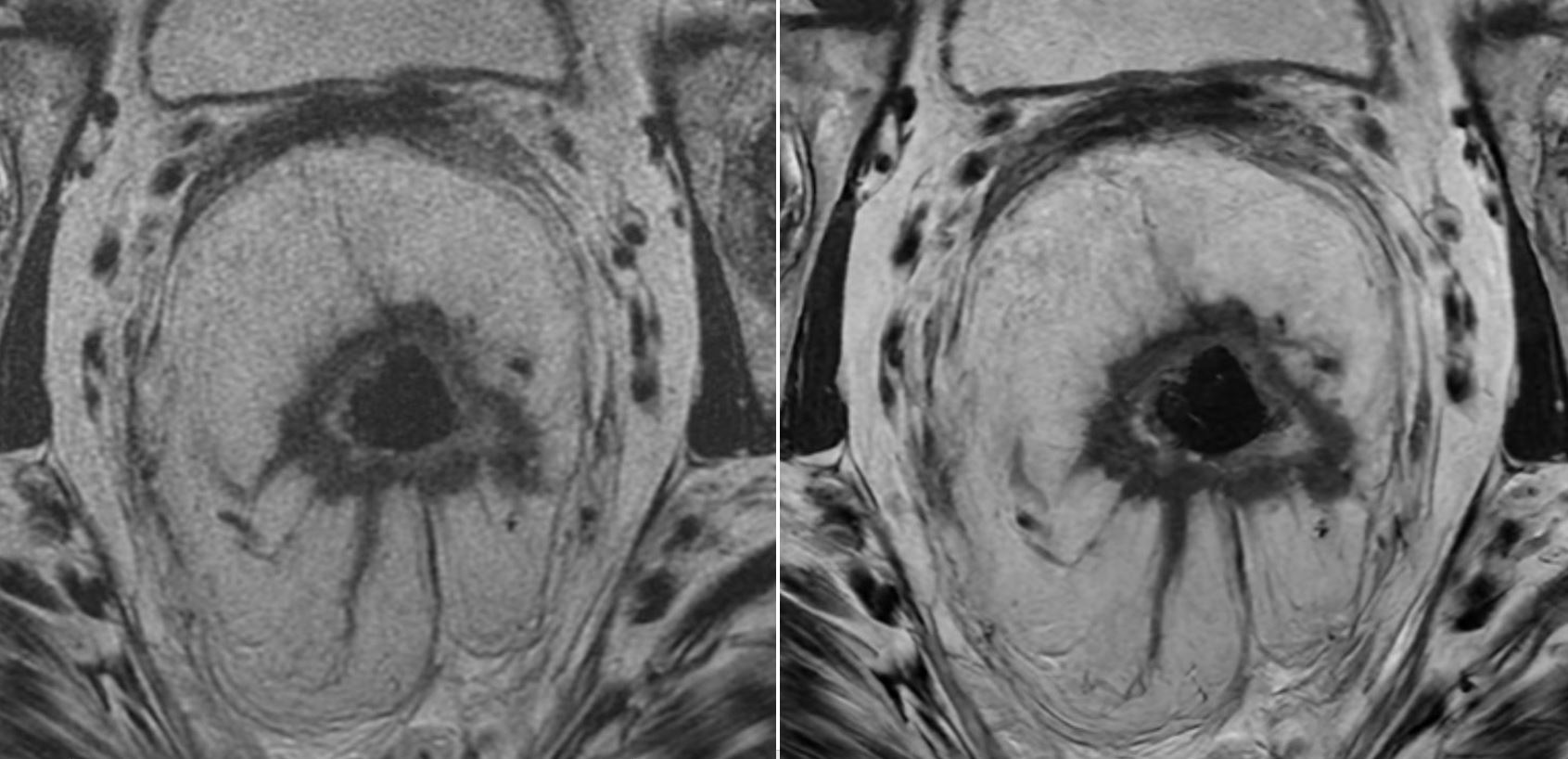
Figure 1. A 67 year-old female with cT3N2M0 rectal adenocarcinoma. Pretreatment MRI pelvis demonstrated a circumferential mid rectal tumor extending to the high rectum with extensive associated extramural venous invasion and significant extension beyond the muscularis propria. (A) 3D FSE Conventional and (B) 3D FSE DLR. DLR was preferred by all three radiologists in the following categories: overall SNR, overall image quality, clear definition of bowel wall layers, nodal margin, and extramural venous invasion.
DOI: https://doi.org/10.58530/2022/3383