3380
Intra-rectal gel suppression effectiveness on rectal cancer MR diffusion-weighted images
Edward M Lawrence1,2 and David H Kim1
1Radiology, UW-Madison School of Medicine and Public Health, Madison, WI, United States, 2Radiology, WS Middleton VA Hospital, Madison, WI, United States
1Radiology, UW-Madison School of Medicine and Public Health, Madison, WI, United States, 2Radiology, WS Middleton VA Hospital, Madison, WI, United States
Synopsis
Retrospective evaluation of intra-rectal gel suppression on DWI from 60 rectal MRIs. The DWI, including b1000, computed synthetic b1500, and ADC maps were evaluated by 2 radiologists independently using a 5 point Likert scale with scores of 4-5 considered fully diagnostic. The median suppression score was significantly greater than 3 for both readers (p<0.05) with fully diagnostic suppression achieved in 57/60 (95.0%) and 53/60 (88.3%) cases for reader 1 and 2, respectively. No study was given a score of 1 or 2 by either reader. These results suggest that gel does not impede reader evaluation for tumor restriction at DWI.
Purpose
There is a lack of consensus regarding the necessity or appropriateness of intra-rectal gel administration for rectal cancer MRI.1 Recently, one point of concern was that poor suppression of the gel on diffusion-weighting imaging (DWI) sequences might result in T2 shine through and significantly effect a radiologist’s ability to evaluate the presence and extent of disease.1 However, this remains largely untested. Adequacy of DWI evaluation is important to the accurate assessment of rectal cancer, especially in the evaluation of possible treatment response.2-5 Thus, the purpose of this study was retrospectively to investigate the effectiveness of intra-rectal gel suppression on rectal cancer MR diffusion-weighted imaging (DWI) and its effect on diagnostic adequacy of the study for tumor evaluation.Methods
Patients who underwent rectal cancer MRI for initial staging, treatment response assessment, or surveillance from March 29-August 20, 2021 were included. Standard preparation included rectal enemas, administration of rectal gel (100 mL), and intravenous glucagon. Reduced field of view DWI, using field-of-view optimized and constrained undistorted single-shot (FOCUS) acquisition, was obtained (b=0, 1000 s/mm2). Apparent diffusion coefficient maps and a computed synthetic high b-value series (b=1500 s/mm2) were created. GE Healthcare (Waukesha, WI USA) MR scanners were utilized. Fifteen MR examinations were completed on a 3 tesla scanner (GE Signa Premier, n=14; Signa Architect, n=1) and 35 examinations on a 1.5 tesla scanner (GE Signa Artist, n=34; GE 450w, n=1). DWI acquisition parameters were as follows: slice thickness/gap 4.8/0.2 mm, field of view 32 x 16 cm, 9 signal averages, repetition time of 4500 ms, echo time of 52.0-66.9 ms.Rectal gel suppression was graded independently by 2 board certified, abdominal radiologists, with 10 and 4 years of rectal MR experience respectively. Suppression was graded on a 5 point Likert scale with a score of 4-5 considered fully diagnostic and scores of 1-3 as demonstrating limitations causing diagnostic uncertainty due to incomplete signal suppression from gel (5, fully suppressed; 4, minimal non-suppression, but diagnostic; 3, mild diagnostic uncertainty due to suppression; 2, major diagnostic limitation; 1, no suppression). Luminal air and associated susceptibility artifact were also evaluated. Wilcoxon signed rank test was used to test the distribution of rectal gel suppression scores.
Results
Sixty patients were included (age 59.3±11.4 years; 26 female, 34 male). Study indications included initial staging (n=26), treatment response (n=23), and surveillance (n=11). Fully diagnostic suppression achieved in 57/60 (95.0%) and 53/60 (88.3%) cases for reader 1 and 2, respectively, and the median suppression score was significantly greater than 3 for both (p<0.05). Minor limitations but leading to an element of diagnostic uncertainty (score of 3) were present in 3 and 7 studies, respectively. No cases were given a score of 1 or 2 (i.e., marked incomplete suppression) by either reader. Gel completely filled the lumen at the level of interest in approximately half of cases, 32/60 and 30/60 respectively. If present, luminal gas typically caused a minor artifact involving <900 circumference (16/28 and 20/30, respectively).Conclusions
Rectal gel suppression was fully diagnostic in the vast majority of cases for both readers. When limitations were present due to incomplete suppression they were only minor in degree. These results suggest that gel does not impede reader evaluation for tumor restriction at diffusion weighted imaging.Acknowledgements
No acknowledgement found.References
- Beets-Tan R, Lambregts D, Maas M, et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2018;28:1465-1475.
- Ichikawa T, Erturk S, Motosugi U, et al. High-b-value diffusion-wieghted MRI in colorectal cancer. Am J Roentgenol. 2006;187(1):181-184.
- Dzik-Jurasz A, Domenig C, George M, et al. Diffusion MRI for prediction of response of rectal cancer to chemoradiation. Lancet 2002;360(9329):307-308.
- Kim S, Lee J, Hong S, et al. Locally advanced rectal cancer: added value of diffusion-weighted MR imaging in the evaluation of tumor response to neoadjuvant chemo- and radiation therapy. Radiology 2009;253:116-125.
- Lambregts D, Vandecaveye V, Barbaro B, et al. Ann Surg Oncol 2011;18(8):2224-2231.
Figures
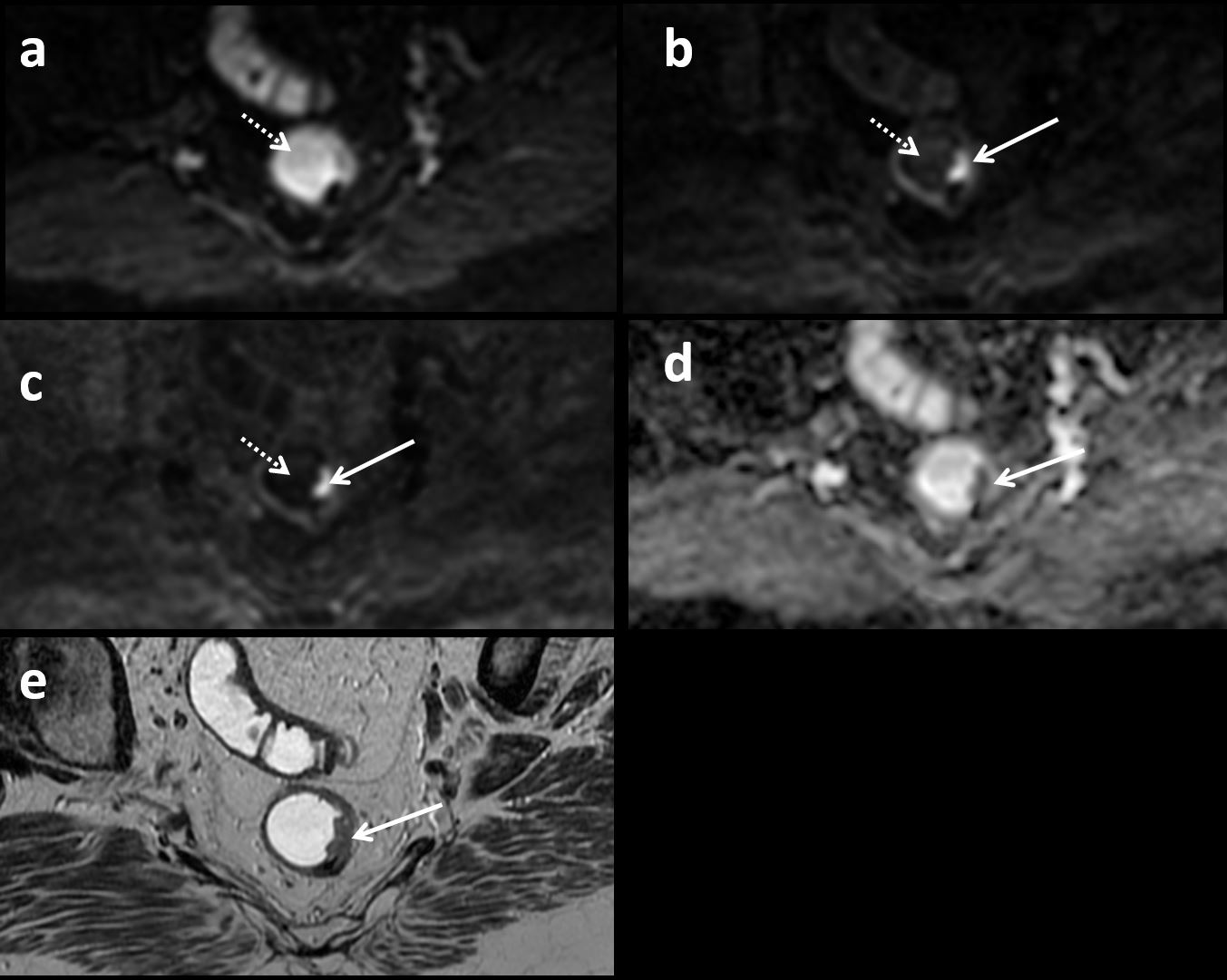
71-year-old with initial staging rectal
MR. Intra-luminal gel (dashed arrow) has high signal on the b0 image (A) but
with excellent suppression on the b1000 (B) and computed synthetic b1500 image
(C). In contrast, the sessile tumor along the left rectal wall at 3 o’clock
(solid arrow) demonstrates high signal on the b1000 and b1500 images as well as
restricted diffusion on the ADC map (D). This study was given a score of 5 by
both readers regarding gel suppression. (E) Matching oblique axial T2-weighted
image also shows the tumor (arrow).
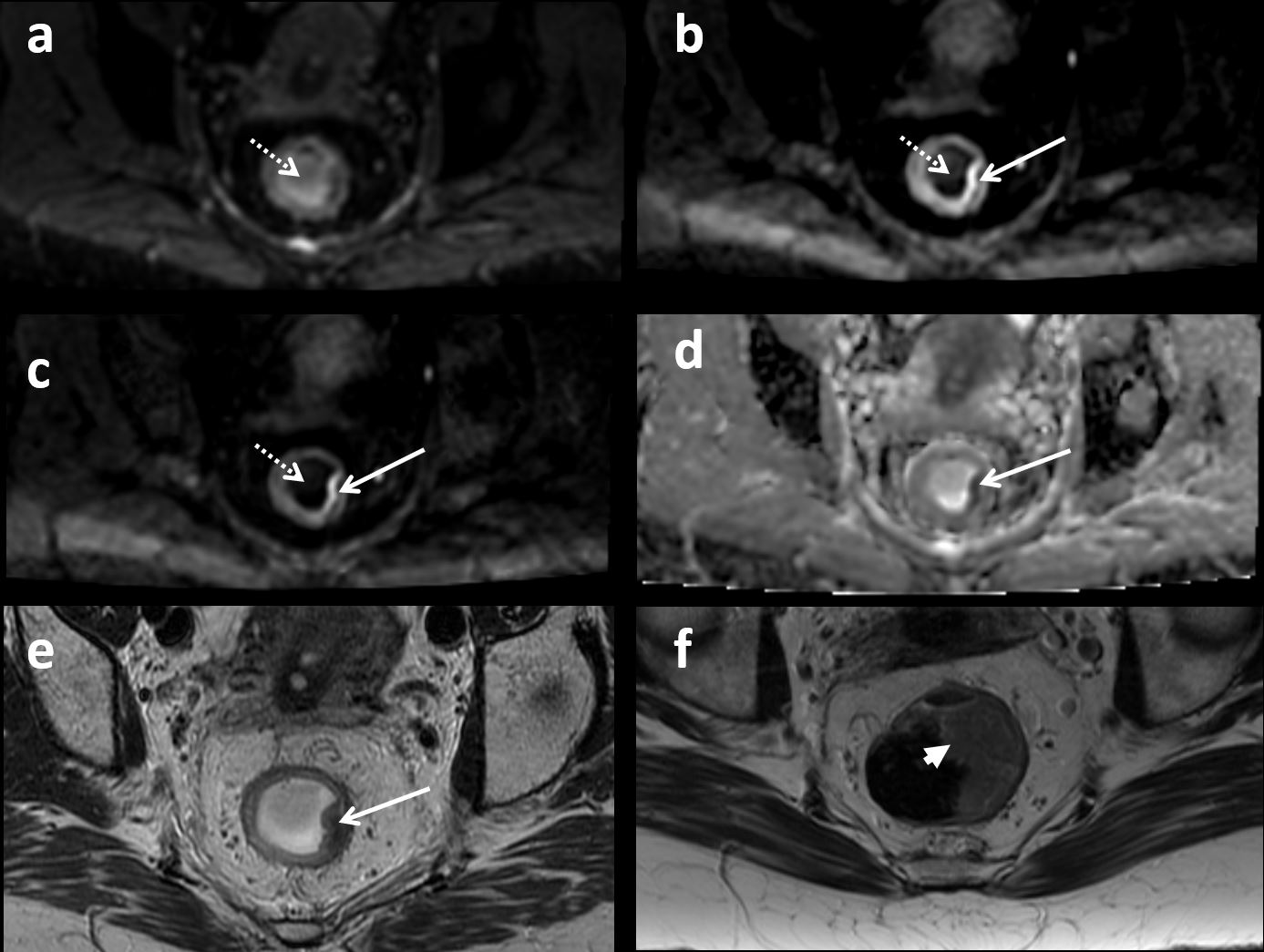
53-year-old with rectal cancer.
Intra-luminal gel (dashed
arrow) on
response assessment MRI has high signal on the b0 image (A) with
diagnostic suppression on b1000 (B) and b1500 (C). Tumor bulk (T2 image from staging MRI in
F, arrowhead) has significantly reduced; however, there is a residual focus of
diffusion restriction (solid
arrow) on the b1000
(B), b1500 images (C), and ADC map (D). This study was given a score of 5 by
reader 1 and 4 by reader 2 for gel suppression. (E) Matching oblique axial
T2-weighted image (tumor,
arrow). Residual
viable tumor was confirmed surgically.
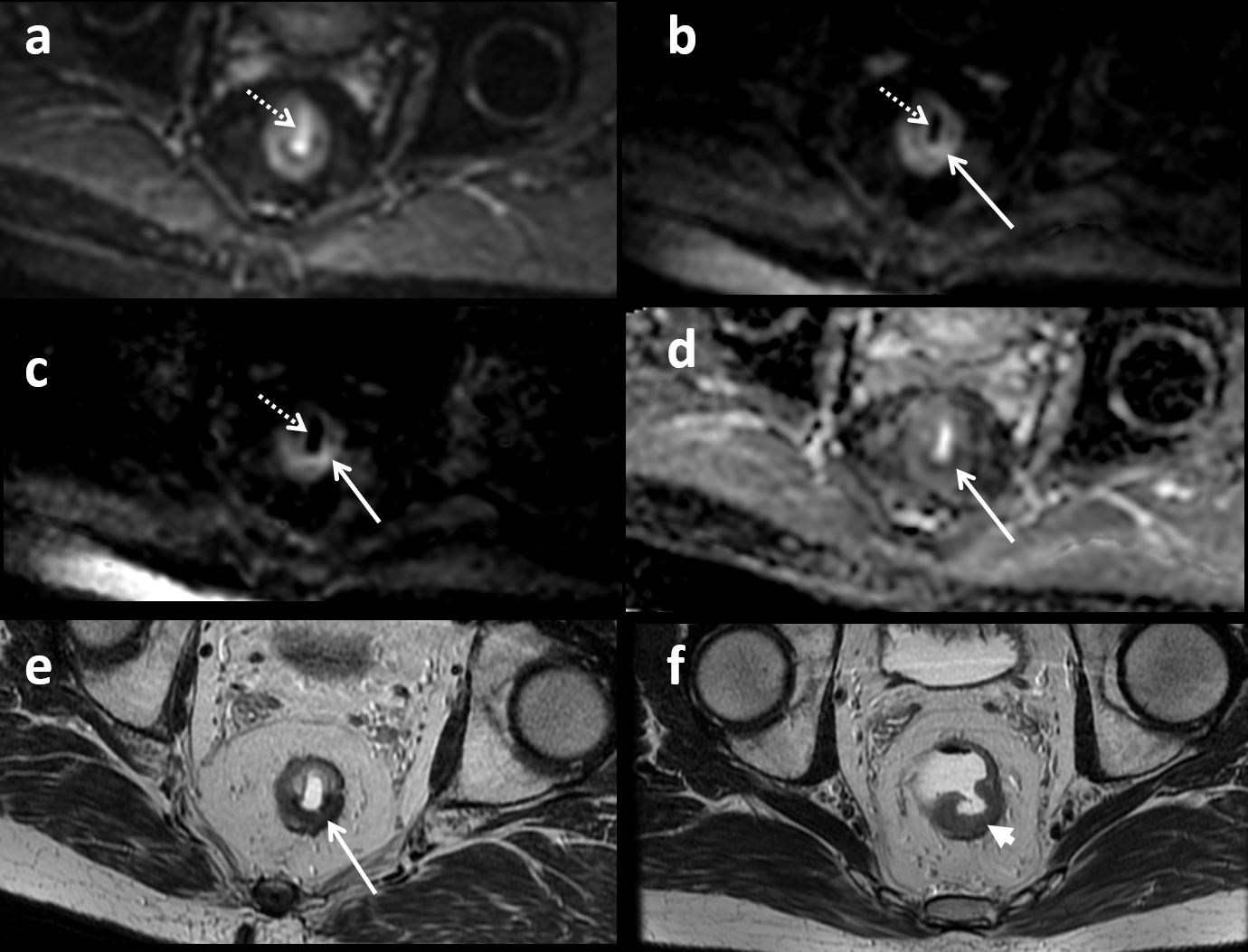
56-year-old with rectal
cancer. Intra-luminal rectal
gel (dashed arrow) on
treatment response MR demonstrates high signal on the b0 image (A) but with
excellent suppression of signal on b1000 (B) and b1500 image (C). Prior tumor (T2 image from initial
staging MRI in F, arrowhead) has reduced size and mostly T2 dark fibrosis now
seen (arrow in E); however, there is evidence of residual diffusion restriction
(solid arrow) on the b1000 (B), b1500 images (C), and ADC map (D). This study
was given a score of 5 by both readers for gel suppression. Residual viable
tumor was confirmed surgically.
DOI: https://doi.org/10.58530/2022/3380